
Abstract
Background and Objective:
Cancer screening rates remain low in rural, racial and ethnic minority, low-income, and uninsured populations. Prior studies showed that cancer screening recommendations vary based on clinicians’ factors. We conducted an exploratory study on primary care clinicians’ beliefs about new or updated cancer screening guidelines according to clinician demographics.
Methods:
This cross-sectional study involved administering a web-based survey in July and August of 2021 to primary care clinicians practicing in diverse ambulatory settings in the Pacific Northwest belonging to the same health system. The survey assessed clinician demographics, attitudes about the impact of cancer screening on mortality, and how clinicians stay up-to-date with guidelines.
Results:
Of the 191 clinicians, 81 responded (42.4%), after removing 13 incomplete surveys, we analyzed 68 (35.6%). The majority agreed/strongly agreed that breast (76.1%), colorectal (95.5%), and cervical (90.9%) cancer screening, and HPV vaccination (85.1%) prevent early cancer mortality: there were no differences according to clinician gender or years in practice. Female compared to male clinicians were more likely to agree/strongly agree that tobacco smoking cessation (female: 100% vs male: 86.4%, P = .01) prevents early cancer mortality, whereas male compared to female clinicians were more likely to agree/strongly agree that lung cancer screening (male: 86.4% vs female: 57.8%, P = .04) prevents early cancer mortality. One-third (33.3%) of clinicians were unaware of the 2021 update on lung cancer screening and females were more likely than males to say they did not know about this change (females: 43.2% vs males: 13.6%, P = .02).
Conclusions:
This study suggests that clinicians’ attitudes are not likely the primary factor affecting low cancer screening rates in some populations and that few differences exist in beliefs based on gender, and none based on years in practice.
Introduction
Evidence that screening for breast, cervical, and colorectal cancer reduces mortality in certain age groups is well-established.1-3 Yet, cancer screening rates remain low in rural, racial and ethnic minority, low-income, and uninsured populations.4-11 For example, in 2019/2020, the American Cancer Society reported that 31% of U.S. women without health insurance received mammography screening in the past 2 years; 21% of women without insurance aged 30 to 64 had received both a human papillomavirus (HPV) and a Papanicolaou (Pap) test within the last 5 years; and, 63% of those over age 50 were up-to-date for colorectal cancer screening. 12 There are many potential reasons for low screening rates, including patient and clinician factors, setting, and health system policies.13,14 Primary care delivers the majority of cancer screening and preventive services recommended by national organizations.15,16 Therefore, clinician factors that influence receipt of cancer screening are important to understand.
A study by Lugtenberg et al 17 found clinician barriers to screening included lack of agreement with recommendations, lack of knowledge about the recommendations, and unclear guideline recommendations. Haas et al 18 found that despite high agreement with guidelines, such as those from the U.S. Preventive Services Task Force (USPSTF), clinicians reported barriers to following guidelines including patient concerns (74% for breast, 36% for cervical), disagreement with the recommendations (50% for breast, 14% for cervical), lack of consistency between health system performance measures and screening guidelines (40% for breast, 21% for cervical), concern about malpractice (33% for breast, 11% for cervical), and lack of time to discuss the benefits and harms with their patients (17% for breast, 8% for cervical).
Clinician beliefs, knowledge, and behavior differ according to type of cancer screening and clinician characteristics. For example, patients of clinicians who believed mammography was somewhat effective were less likely to receive the screening than patients of clinicians who believed it to be very effective. 19 Another study found female clinicians were more likely to have female patients up-to-date for cervical cancer screening than male clinicians. 20 In addition, 74% of primary care physicians and pulmonologists endorsed lung cancer screening, though knowledge of screening eligibility, documentation, and nodule management was suboptimal. Key barriers included inadequate time (36%), inadequate staffing (36%), and patients having too many other illnesses to address screening (38%). 21 A study by Kanodra et al 22 reported similar findings. Lung cancer screening is still a relatively new recommendation compared to breast, cervical, and colorectal cancer screening, which may explain why physicians were more likely to endorse the importance of colorectal cancer screening, as found in one study. 23 Another study found physicians were more likely to order lung cancer screening tests if they believed that expert groups recommended lung cancer screening or that screening tests were effective.24,25
Three issues emerge regarding existing literature on this topic. First, a significant number of currently published studies were published before recent guideline changes and updates, such as the 2021 lung cancer screening update by the USPSTF. 26 Second, few studies examined where clinicians specifically sought information about screening guidelines, 27 and third, few studied the impact clinician gender or years in practice have on the delivery of early detection services. 28
To address these gaps in existing literature, we undertook an exploratory survey study with primary care clinicians to: (1) assess current beliefs about cancer screening and guidelines; (2) assess their knowledge and behaviors about where to find guideline information; and (3) determine if any of these differed according to demographics (ie, gender or years in practice) of the clinician surveyed.
Methods
Study Design, Setting, and Participants
In this cross-sectional study, we surveyed a convenience sample of 191 clinicians, including 135 MDs/DOs and 56 NPs/PAs, based at 7 family medicine clinics associated with an academic health center based in the Pacific Northwest. Although all clinics: (1) provided care to patients across the lifespan, (2) were certified Patient-Centered Primary Care Medical Homes, and (3) used a cooperative, team-focused approach for patient care needs, their care settings were very diverse. All clinics were located throughout the Portland metropolitan area with the exception of one each at a federally qualified health center (FQHC), a Rural Health Center, and an academic health center.
Survey Development and Variables
The survey was developed by adapting an existing questionnaire 29 that addressed cancer screening services and the research question of interest. The survey had 4 sections with a total of 23 questions. The first section ascertained demographic characteristics of participants, including race, ethnicity (Hispanic, non-Hispanic, prefer not to answer), age, gender identity (male, female, non-binary, another gender, prefer not to answer), and length of time in practice. The second section assessed participants’ beliefs about: (1) the impact of cancer screening (breast, cervical, colorectal, and lung), and receipt of HPV vaccines and tobacco smoking cessation has on cancer mortality reduction (6 items), and (2) attitudes about cancer screening guidelines (5 items). The third section asked clinicians where they look for cancer screening guideline information to stay up-to-date and where they preferred it be located. Question response formats used either a Likert scale (1 = Strongly Disagree, 2 = Disagree, 3 = Neither Agree nor Disagree, 4 = Agree, 5 = Strongly Agree), a Likert type scale with various 4-scaled responses, or response options with one or more choices, such as check all statements that apply. For reporting purposes, response categories were combined for the Likert scale (1 = Strongly Disagree/Disagree, 3 = Neither Agree nor Disagree, 4 = Agree/Strongly Agree).
After development, the questionnaire was pilot-tested and clinical sensibility tested to ensure readability, understandability, comprehensiveness, and acceptability. 30 Modifications were made based on input from pilot testers and to ensure we could differentiate between cancer screening guidelines and clinician implementation of these guidelines, as they were deemed separate concepts.
Data Collection
A list of all faculty clinicians and their contact information was assembled by Department of Family Medicine staff members. The survey was built into a web-based survey system (Qualtrics) and the link to the survey was distributed via email invitation, which described the purpose of the survey. Two follow-up e-mail reminders were sent: one 2 weeks after the original invitation and another 2 weeks after that. We administered the survey between July and August of 2021 and ended data collection 2 weeks after the final email reminder was sent. We chose a 3-attempt outreach approach to minimize clinician burden. 31 All study activities were reviewed and approved by our Institutional Review Board (IRB #00020262).
Data Management and Statistical Analyses
Incoming surveys were assessed for completeness, and 12 were excluded from analyses because respondents did not complete any questions on cancer screening or guidelines (they completed the demographic section only). Another survey was excluded because they did not respond to the gender identity question. Descriptive statistics, including frequencies and percentages were calculated to describe findings. Categorical data comparing responses according to gender and years in practice were analyzed using Pearson Chi-square or the Mann-Whitney U test. For questions where multiple responses were possible, selected options were coded as 1 and unselected options were coded as 0. All tests were 2-tailed, and alpha levels to determine statistical significance were set at <.05. IBM® SPSS Version 28 was used for all analyses.
Results
Of the 191 clinicians, 81 responded (42.4%). After removing 13 incomplete surveys, 68 surveys were left for analyses (35.6%). The majority of respondents were female (67.6%), white (89.7%), non-Hispanic (95.5%), and had been in practice for less than 5 years (29.4%) (Table 1).
Demographic Information by Clinician Gender.
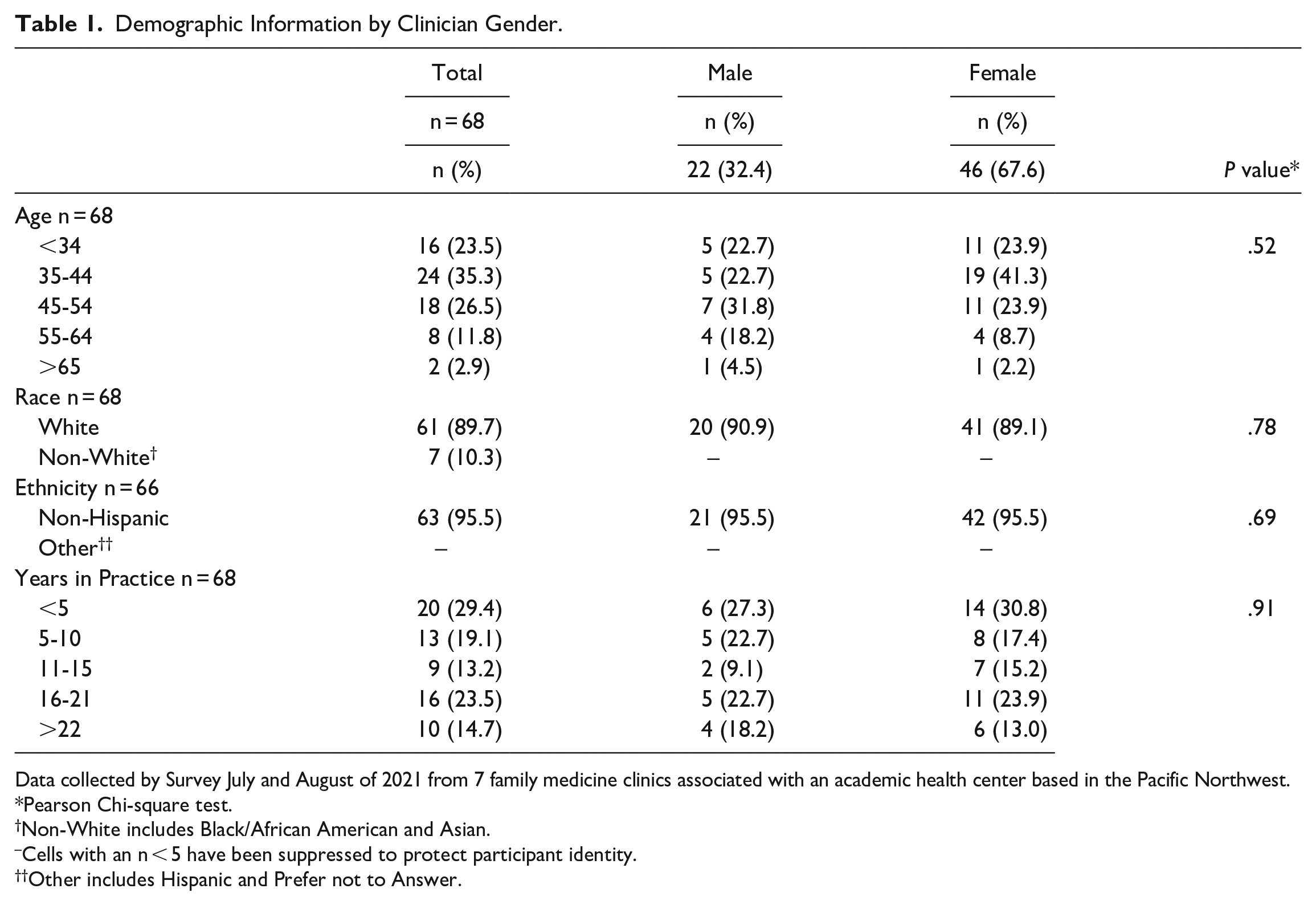
Data collected by Survey July and August of 2021 from 7 family medicine clinics associated with an academic health center based in the Pacific Northwest.
Pearson Chi-square test.
Non-White includes Black/African American and Asian.
Cells with an n < 5 have been suppressed to protect participant identity.
Other includes Hispanic and Prefer not to Answer.
The majority of study participants agreed/strongly agreed that breast (76.1%), colorectal (95.5%), and cervical (90.9%) cancer screening, and HPV vaccination (85.1%) prevent early cancer mortality: there were no differences according to clinician gender or length of time in practice. Female compared to male clinicians were more likely to agree/strongly agree that tobacco smoking cessation prevents early cancer mortality (female: 100% vs male: 86.4%, P = .01). Male clinicians were more likely to agree/strongly agree lung cancer screening (male: 86.4% vs female: 57.8%, P = .04) prevents early cancer mortality. In fact, 37.8% of women neither agreed nor disagreed that lung cancer screening prevents early mortality (Table 2). Length of time in practice did not affect beliefs on cancer screening or mortality risk reduction (data not shown).
Beliefs About Cancer Screening and the Impact on Mortality by Clinician Gender.

Data collected by Survey July and August of 2021 from 7 family medicine clinics associated with an academic health center based in the Pacific Northwest.
Mann-Whitney U Test.
Bold indicates the statistically significant values.
The majority of clinicians felt cancer screening guidelines were useful (50.7%), which did not differ according to gender or years in practice. Similarly, the majority of clinicians felt that implementing cancer screening guidelines was clear (65.7%), which did not differ by gender or length of time in practice. When asked about patients’ request for cancer screening, 19.4% indicated patients’ request screening less often, 32.8% indicated neither more or less often, 20.9% indicated as often, and 26.9% indicated more often than recommended by guidelines, which also did not differ according to gender (Table 3) or length of time in practice (data not shown).
Attitudes About Cancer Screening Guidelines by Clinician Gender.

Data collected by Survey July and August of 2021 from 7 family medicine clinics associated with an academic health center based in the Pacific Northwest.
Mann-Whitney U Test.
Bold indicates the statistically significant values.
When asked where clinicians look to find current cancer screening guidelines, the majority go to the USPSTF (98.5%). Other information sources included UptoDate (47.0%), electronic health record (EHR) best practice alerts (47.0%), American Cancer Society (31.8%), professional conferences (31.8%), academic literature (24.2%), a colleague (15.2%), grand rounds sessions (6.1%), or other (9.1%). Information resource seeking did not differ according to clinician gender (Table 4) or length of time in practice (data not shown). When guidelines were conflicting, the majority (92.6%) of clinicians indicated they choose the USPSTF.
Preferred Access to Cancer Screening Guidelines by Clinician Gender.

Data collected by Survey July and August of 2021 from 7 family medicine clinics associated with an academic health center based in the Pacific Northwest.
Totals and percentages represent the respondents selected option.
Mann-Whitney U test.
When asked about the 2021 USPSTF update on lung cancer screening, one-third (33.3%) were unaware of the change and females were more likely than male clinicians to not know about this change (females: 43.2% vs males: 13.6%, P = .02). The majority of those who knew of the change learned about it through the USPSTF (37.9%), academic literature (18.2%), or other (19.7%), which included local meetings/e-mail messages, podcasts, social media, or lay media, which did not differ by clinician gender.
Discussion
Study Findings
Overall, this exploratory study found the majority of clinicians believe cancer screening prevents early cancer mortality. We found 2 statistical differences according to clinician gender and none according to years in practice. Female clinicians were more likely to agree/strongly agree that tobacco cessation prevents early cancer mortality than male clinicians (female: 100% vs male: 86.4%, P = .01); whereas, male clinicians were more likely to agree/strongly agree that lung cancer screening prevents early cancer mortality compared to females (male: 86.4% vs female: 57.8%, P = .04).
Findings in the Context of Current Literature
Prior research by Henderson et al 32 found about 40% of clinicians believed lung cancer screening reduces mortality, so beliefs about lung cancer screening as a mode for mortality reduction have changed. However, gaps in knowledge between male and female clinicians may exist, which indicates the need for additional education. 33 Other studies highlighted that the benefits of lung cancer screening are not clear to clinicians, which may be affecting female clinicians more than males. 34 In fact, we found that one-third of our respondents were unaware of the 2021 USPSTF update on lung cancer screening (more female than male clinicians were unaware), which indicates that challenges continue to exist among clinicians in staying up-to-date with current guidelines. Khairy et al 35 further indicated knowledge differences of lung cancer screening guidelines between FQHC clinicians and academic providers, which may be related to patients of FQHCs being more likely to have Medicare/Medicaid health insurance compared to patients seen in academic settings. Because clinician knowledge of guideline recommendations may adversely impact historically underserved patients, there is a need for education and tools to assist clinicians in providing the most up-to-date care possible.34,35
We also found that USPSTF guidelines were predominantly used by respondents in our study, which is contrary to a 2011 national survey study, which reported that physicians rated American Cancer Society guidelines more influential than USPSTF guidelines. 36 Of note, previous research only asked about breast and cervical cancer screenings, whereas we asked about many cancer screenings. Another study confirmed our findings that most clinicians (88.4%) reported the USPSTF was influential to their practice. 37 We found no difference according to clinician gender or years in practice for any self-reported information seeking behaviors.
Collectively, study findings suggest that clinicians’ attitudes and perspectives may not be the primary factor affecting low cancer screening and risk reduction rates in some populations. It is the first step to help understand the reasons for a lack of cancer screening, but more research is needed to fully identify the barriers. Indeed, many factors affect cancer care across the entire healthcare continuum, including patient and system factors 38 and/or regional differences that have long been shown to affect patients’ receipt of services. 39 Ongoing observational and interventional research is needed to fully realize the benefits of cancer screening.
Strengths and Limitations
The strengths of this study include that we surveyed participants about very recent guidelines and updates for cancer screening and risk reduction strategies. Limitations include that the study population was associated with a single academic health center, which limits generalizability and may skew our findings toward greater knowledge of cancer screening guidelines. While we included male, female, non-binary, another gender, and prefer not to answer in our demographics variable options, we only received surveys from female and male respondents. In addition, the categories chosen were not cis or transgender specific. We had a response rate of 35.6% for usable data, which limits representation of the study population, but is higher than other reported physician survey response rates, which ranged from 18% to 35%.32,40 In fact, prior research found lower (compared to higher) response rates did not change survey results, 31 particularly among physicians. 41
Conclusion
In conclusion, clinicians agree that cancer screening reduces cancer mortality, with few differences according to clinician gender and none based on years in practice. Future research should focus on improving clinician awareness of lung cancer screening guidelines and strategies to educate clinicians when recommendations change.
Footnotes
Acknowledgements
We would like to thank the clinicians who spent time filling out this survey. We would also like to thank John Muench for helping with survey testing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Cancer Institute (NCI) under award number P50CA244289. This program was launched by NCI as part of the Cancer Moonshot. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.