
Abstract
Introduction/Objective:
Reducing inappropriate emergency room (ER) visits is a major health management objective. While Hispanic patients reportedly have the highest percentage of avoidable ER visits (4.89%), empirical research is scarce. Effective provider communication can increase appropriate ER utilization. Our objective was to examine associations between safety net primary care providers’ communication with Hispanic patients and Hispanic patients’ ER use.
Methods:
We used 2022 Health Center Patient Survey data collected by the United States Health Resources and Services Administration. Our predictors were patient-reported provider communication and nonclinical staff evaluation items from the Consumer Assessment of Healthcare Providers and Systems (CAHPS) instrument. Our outcome variable was patient-reported ER visits in the previous year. We used binary logistic regression to examine the association.
Results:
Patients who had used health centers longer had significantly lower odds of ER visits (44%-46%). Patients who had initiated conversations about their health issues had 55% higher odds of ER visits. Healthier patients and women had lower odds while insured patients and those with frequent visits to health centers had higher odds of ER use.
Conclusions:
Primary care continuity, stable medical home, and effective interactions with providers may reduce ER use.
Keywords
Introduction
Research on emergency room (ER) costs in the United States emphasizes declining ER revenues due to increased Medicaid, Medicare, and uninsured visits.1,2 In 2019, Medicaid and uninsured costs exceeded ER revenues by $3.7 and $2.4 billion, respectively. 2 Many ER visits are for continuing and ambulatory sensitive health conditions and could be avoided.3,4 Additionally, some ER visits are for conditions that ERs cannot fully address (eg, dental, mental health, back pain, etc.) and would be more effectively and efficiently treated on an outpatient basis.3,5,6 Reducing avoidable ER visits is a major health management objective as it could decrease ER costs, overcrowding, and waiting time.
Certain population groups are more prone to use emergency services for avoidable or non-urgent health conditions.5,7 For instance, Black and Hispanic patients reported higher ER use for continuing health conditions and were more likely to have 3 or more ER visits in previous 6 months. 8 In a national sample, Hispanic patients had the highest percentage of avoidable ER visits (4.89%). 5 Hispanics are the largest minority group in the United States representing 19.5% of the total population. 9 Approximately one-third (32%) of Hispanics were born outside the United States 10 and may have difficulties accessing and using health care services.
One way to reduce avoidable ER visits is the availability of robust primary care. Extensive research evidence11,12 demonstrates how strong primary care systems contribute to better population health and lower mortality. Effective primary care is accessible, continuous, coordinated, and community-based.11,12 Effective primary care is also associated with lower emergency services utilization and costs.13 -16 However, even when primary care is available, affordable, and accessible, it is inaccessible if a patient cannot easily communicate with a provider. 17 While physical access to care is critical, the way providers interact with patients may influence whether patients choose to disclose or not to disclose certain health information or return or not to return to the provider.
Effective provider communication, characterized by kindness, caring, shared decision making, clear explanations, cultural sensitivity, and trust, 18 positively influences objective and subjective health outcomes, 19 increases up-take of preventive screenings among racial and ethnic groups, 20 and improves the quality of health care. 21 High-quality provider communication may be particularly important for underserved and marginalized populations 22 as they are associated with reduced use of emergency services.16,23 -25 The National Institute for Minority Health and Health Disparities 26 recognized patient-clinician interactions as a priority research area to improve health care quality and patient outcomes. While Hispanics disproportionately use community health clinics (33% of Hispanic patients) compared with 13% of Black patients, and 16% of White patients, according to the Kaiser Family Foundation, 27 empirical research on Hispanic patients’ use of emergency care is scant. This study examines associations between safety net primary care providers’ communication with Hispanic patients and Hispanic patients’ use of emergency services.
Methods
Study Design
Our study used 2022 Health Center Patient Survey (HCPS) data collected by the United States Health Resources and Services Administration (HRSA) in 2021 to 2022. 28 The dataset contains self-reported information from low-income, publicly insured, and uninsured patients using primary care clinics funded by HRSA. Primary care facilities funded by HRSA include community health centers, public housing primary care programs, health care for the homeless, and migrant health care programs. The dataset contains information on patients’ socio-demographic characteristics, chronic health conditions, health behaviors, and access to health care facilities and services, and utilization of satisfaction with health care services received at these centers, among others.
Measures
Our predictor variables were provider communication and clinic staff helpfulness and respect items from the Consumer Assessment of Healthcare Providers and Systems (CAHPS) Clinician and Group Surveys instrument, 29 which were part of the HPCS. The HPCS asked patients whether the provider listened carefully, gave information about patient’s health questions/concerns, knew important information about patient’s medical history, showed respect, spent enough time with patients, and talked about the prescriptions and over-the-counter medications patients were taking (always, usually, sometimes, never). The HCPS also asked whether provider’s explanations were easy to understand (always, usually, sometimes, never), and whether patients talked with the provider about health questions/concerns (yes/no). Clinic staff helpfulness and respect were captured by the following items: clerks and receptionists were helpful, and clerks and receptionists were courteous and respectful (always, usually, sometimes, never). Because over half of patient responses were Always, their responses were dichotomized as Always and Not Always as recommended by CAHPS. 30
Patient responses to our outcome variable, emergency room (ER) visits in the past 12 months, were dichotomized into No ER visits and ER visits.
Consistent with the literature on the topic, the study control variables included patient’s age (categorized as 0-17, 18-44, 45-64, and 65 years and older), sex assigned at birth (male, female), health status (good/very good/excellent vs fair/poor), insurance status (insured – Medicaid, Medicare, dual Medicaid and Medicare, and private vs uninsured), neighborhood safety (very safe/moderately safe vs very unsafe/moderately unsafe), length of going to the health center (less than 1 year, at least 1 year but less than 3 years, at least 3 years but less than 5 years, at least 5 years but less than 10 years, and 10 years and longer), number of doctor visits during previous 12 months (0 times, 1 to 2 times, 3 to 4 times, 5 to 7 times, 8 to 10 times, and 11 or more times), needing someone’s help to understand the doctor (yes/no), and being provided with a translator or interpreter (yes/no/did not need the services).
Statistical Analysis
We used binary logistic regression to examine the association between provider communication variables and ER utilization among Hispanic patients. The model was adjusted for demographic characteristics and other control variables including health care utilization at community health centers. Prior to modeling, we assessed pairwise correlations among all predictors, revealing weak to moderate associations. To address missing data and minimize potential bias from listwise deletion, we employed the multiple imputation method, 31 generating 5 imputed datasets. The regression results were pooled using Rubin’s 32 rules to account for the variability introduced by imputation. Adjusted odds ratios (AORs) were computed by exponentiating the estimated regression coefficients. For each AOR, we reported the corresponding 95% confidence interval (CI) and considered results statistically significant at the .05 level (P < .05). In addition, we conducted sensitivity analyses by re-estimating the logistic regression model using only complete cases, with 418 Hispanic patients compared to 1869 in the multiple imputed analyses. The results were broadly consistent with those from the imputed datasets. The direction and statistical significance of the predictors showed similar patterns, and the estimated odds ratios were of comparable magnitude, suggesting that the multiple imputation method is robust for handling missing data. All analyses were conducted using RStudio (version 2023.06.1+524).
Results
Our sample included 1869 Hispanic patients. Descriptive statistics are shown in Table 1. About 63% had no ER visits during the past 12 months. Overall, provider-patient communication was rated positively. Most patients reported that primary care providers (PCPs) always explained things clearly (62.9%), listened carefully (67.5%), showed respect (72.2%), and spent enough time with them (66.0%). In addition, 67.8% of Hispanic patients initiated conversations with their PCPs about their health concerns, and 53.9% were provided with relevant information. More than half (57.8%) felt that their PCPs always knew important information about their medical history. However, only 45.9% of patients indicated that their PCPs had talked about all prescribed and over-the-counter medications. Staff interactions were also favorable, with 62.0% finding clerks and receptionists helpful and 69.9% receiving courteous and respectful treatment.
Outcome, Communication Assessments, and Control Variables (n = 1869).

Abbreviations: ER, emergency room; PCP, primary care provider.
Among our Hispanic patient population, 33.9% were aged 18 to 44 years, 36% were 45 to 64 years, and 11.7% were 65 years or older. The majority were female (71.6%). Over half (54.3%) rated their health as good, very good, or excellent. Approximately half (50.5%) were insured by Medicaid. In addition, 16.6% were uninsured, 10.2% had private insurance, 9.4% were dually covered by Medicaid and Medicare, and 3.6% were enrolled in Medicare only. Most patients (88.9%) lived in very or moderately safe neighborhoods. Nearly one-third (29.1%) had been receiving care at the health center for 10 years or more; all other categories, ranging from less than 1 year to under 10 years, each represented between 12% and 16% of the sample. Roughly 30% of patients had 1 to 2 doctor visits, and a similar proportion had 3 to 4 visits in previous 12 months. Only 7.7% relied on ERs for most of their care. About one-quarter (24.2%) need help understanding the doctor, and 28% had received translation or interpreter services at the health center.
Table 2 presents the adjusted logistic regression results. Patients who initiated conversations/discussions with their PCPs about health concerns had significantly 55% higher odds of ER visits (AOR = 1.55; 95% CI = 1.05-2.30; P = .03), compared to those who did not. Patients whose PCPs always provided easy to understand explanations or gave information about health concerns had higher odds of ER visits, though neither association was statistically significant. In contrast, patients whose PCPs always listened carefully or knew information about their medical history (had lower odds of ER visits, though these results were also not statistically significant. Patients whose PCPs always showed respect had higher odds of ER visits, as did those whose PCPs always spent enough time with them; again, neither association reached statistical significance. While the odds ratios suggest a reduction in ER visits, ranging from approximately 3% to 25%, none of these associations were statistically significant for PCPs’ discussions about medications, staff helpfulness, or staff courtesy and respect.
Association Between PCP Communication and ER Visits During the Past 12 Months for Hispanics.
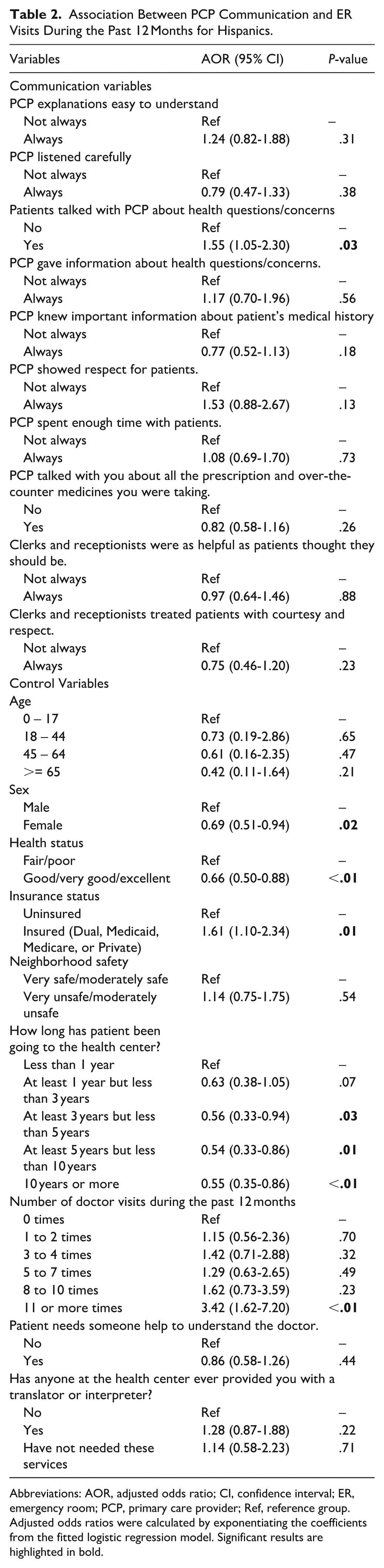
Abbreviations: AOR, adjusted odds ratio; CI, confidence interval; ER, emergency room; PCP, primary care provider; Ref, reference group.
Adjusted odds ratios were calculated by exponentiating the coefficients from the fitted logistic regression model. Significant results are highlighted in bold.
Patients in good, very good, or excellent health had significantly 34% lower odds of ER use (AOR = 0.66; 95% CI = 0.50-0.88; P < .01), compared to patients in poorer health. Females had 31% reduced odds of ER visits (AOR = 0.69; 95% CI = 0.51-0.94; P = .02), while having health insurance was associated with 61% increased odds (AOR = 1.61; 95% CI = 1.10-2.34; P = .01). Compared to patients with less than 1 year of care, those who attended health centers for a longer time (3-5, 5-10, and ≥10 years) had 44% to 46% significantly reduced odds of ER visits (AOR = 0.56; 95% CI = 0.33-0.94; P = .03); (AOR = 0.54; 95% CI = 0.33-0.86; P = .01); and (AOR = 0.55; 95% CI = 0.35-0.86; P < .01), respectively. Frequent primary care utilization was positively associated with ER use: patients with 11 or more doctor visits in previous 12 months had more than 3 times the odds of visiting the ER compared to those with no visits (AOR = 3.42; 95% CI = 1.62-7.20; P < .01). No significant associations were found for neighborhood safety, interpreter use, or age.
Discussion
Our study examined associations between safety net providers communication with Hispanic patients and Hispanics’ use of emergency care in the United States. The most notable finding is the role of primary care continuity in reducing ER use by Hispanics attending safety net health facilities. Compared to those going to the health center for less than a year, patients going to the health center for 1 to 3 years reported a marginally significant 37% reduced odds of an ER visit, while those reporting longer use of the center had a highly significant 45% to 46% reduced odds of an ER visit. These results affirm the importance of health care continuity. A systematic review stated that health care continuity has a protective effect on patient mortality. 33 Recently, Maarsingh, 34 in the review of empirical literature on continuity with the same provider (relational/interpersonal continuity) and having a regular source of care (clinic continuity), concluded that both types of continuity were associated with lower utilization of emergency care. Interpersonal continuity in primary care was associated with 28% lower odds of having ER visits for chronically ill Medicaid recipients. 35 Relational continuity of care is very important for Hispanic patients as over 80% of the patients would like to see the same PCP. 36 Our finding adds to the empirical evidence that using the same provider/clinic for prolonged periods of time is significantly associated with fewer ER visits for Hispanic patients.
The communication items were a mixed bag, with several behaving as expected and others opposite. The only communication item attaining significance (and of appreciable magnitude) was Hispanic patients initiating discussions of their health concerns. This finding suggests that voicing concerns and discussing health issues with a provider, which was associated with increased odds of ER utilization, may be reflective of an underlying serious or yet poorly managed health issue that prompted patients to voice concerns and providers to spend time explaining the condition and whether and when to use emergency care. Interestingly, the provider respect and easy to understand explanations items showed similar (although statistically insignificant) relationships. The findings suggest that patients and providers are more attuned to the importance of effective communication as health challenges rise.
These factors also likely help drive the observed and statistically significant relationship between continuity with a provider/clinic and reduced odds of ER utilization. Presumably having open discussions about health concerns is predicated upon patients feeling heard and respected which in turn leads to a sustained, effective provider-patient relationship. While not achieving statistical significance, a dose-response relationship with more visits associated with increased odds of an ER visit is suggested, perhaps indicative of active but unsuccessful attempts to manage complex conditions.
The usual correlates/predictors emerged as significant risk factors for higher ER utilization within our Hispanic only analytic sample – being a male, in fair/poor health, or insured. We found that women in our sample had 31% lower odds of using emergency services. This finding is unsurprising given that Hispanic men tend to work in injury-prone industries such as construction, mining, and material transportation, 37 which may lead to more ER visits. This result is also supported by the Kaiser Family Foundation 38 that reported that females on Medicaid use as many preventive services as privately insured women and, consequently, are healthier and do not use ERs as often as men.
We found that insured Hispanics used more emergency services than uninsured Hispanics. Generally, in the United States uninsured individuals use emergency care considerably less than publicly insured. 39 The National Center for Health Statistics 40 reported in 2024 that uninsured patients used less ER services than those insured by Medicaid or Medicare. Overall, Hispanics try to avoid or delay health care due to discrimination, insurance status, and language barriers, among other reasons.27,41,42
Limitations and Strengths
Ours was a correlational study and causality cannot be established. We could not differentiate between the interpersonal continuity (seeing the same provider) and having a regular source of care (health center or community health clinic). However, seeing a PCP regularly or having a consistent source of care are beneficial for patients in terms of reduced ER visits. 34 While our study rationale emphasized the aim of reducing avoidable/unnecessary ER visits, the HCPS dataset only captured if an ER visit occurred, without respect to its necessity. Nonetheless, the observed significant reductions in the odds of seeking emergency care reflect substantial clinical and non-clinical resource savings.
To our knowledge, research on emergency care utilization by Hispanic patients is sparse. Our research addresses this important issue. Future data collection efforts should seek to include measures of disease severity and comorbidities to better identify the presence and management of ambulatory sensitive conditions and other factors that might influence the likelihood of ER use.
Conclusions and Recommendations
Our study demonstrated the importance of primary care continuity in reducing emergency services use. A patient with a stable medical home has lower odds of seeking or needing care at an ER. Providers who focus on eliciting/addressing patient concerns enhance patient education, show respect for patients, and build trust, possibly leading to increased adherence and reducing unnecessary emergency care. PCPs should educate their patients about when it is appropriate to use emergency services. Health care managers should incentivize PCPs to retain patients and allocate funding for the development of provider training programs on how to improve communication with low-income and marginalized patients.
Footnotes
Ethical Considerations
We used a publicly available database with de-identified participant information. Ethical approval was not required.
Consent to Participate
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.