
Abstract
Introduction/Objectives:
Patients returning to the community from incarceration (ie, reentry) are at heightened risk of experiencing trauma when interacting with the healthcare system. Healthcare professionals may not recognize patients’ trauma reactions or know how to effectively respond. This paper describes the development and pilot evaluation of a single-session training to prepare primary care teams to deliver trauma-informed care (TIC) to patients experiencing reentry.
Methods:
A multidisciplinary team including community members with lived experience engaged in a multiphase human-centered design process that incorporated interviews, discussions, and a participatory process to design and evaluate a single-session interactive pilot training targeting providers’ attitudes toward formerly incarcerated patients and confidence to deliver TIC.
Results:
Both pre- and post-training surveys were completed by 12 TIC training attendees, which included primary care providers and staff. Trainees reported significant increases in confidence to reduce potentially re-traumatizing practices and improved attitudes toward formerly incarcerated individuals. They also expressed interest in receiving additional TIC training and learning how best to care for and meet the needs of persons with a history of incarceration. Trainees described the panel of community members with lived experience as one of the most rewarding aspects of the training.
Conclusion:
Centering people with lived experience in the training design and delivery produced a single-session TIC training that was both well-received and effective. Our TIC training helped primary care providers and staff move from being merely informed on trauma to having the self-efficacy to prevent and respond to trauma reactions during encounters with all patients, particularly those with a history of incarceration.
Keywords
Introduction
Trauma—the intense, overwhelming experiences that involve threat, harm, or serious loss to a person’s physical and/or psychosocial well-being or the witness thereof—crosscuts the United States’ prisons and jails, impacting nearly all 1.9 million individuals confined therein.1 -3 Beyond the significant trauma of incarceration itself, 4 up to 99% of persons who have been incarcerated report a prior history of trauma, including adverse childhood experiences (ACEs).5,6 Additionally, incarceration disproportionately targets communities with historical trauma, or the collective multigenerational trauma experienced by people with a shared history of targeted systemic oppression (eg, colonization, slavery, and segregation).7 -9 Trauma exposures, particularly when early or chronic, negatively affect health by altering neurological, hormonal, immune, and genetic functions10,11 and are associated with an increased risk for the leading causes of morbidity and death. 11 Ninety-five percent of incarcerated persons are expected to ultimately exit the carceral system to return to the community (ie, reentry). 12 While linkage to healthcare helps to curb the significantly high risk of recurrent substance use, fatal overdose, and reincarceration during reentry,13 -18 community-based healthcare professionals may be unaware of their potential to support health during reentry and/or feel unprepared to address the complex needs of patients experiencing reentry. As such, patients are at risk of experiencing further trauma during individual-level (eg, encounters with the healthcare staff and providers) and systemic-level (eg, health policy and healthcare access) interactions with the healthcare system. 19
Trauma reactions, or the adaptive and maladaptive psychological and physiological responses that occur as a result of experiencing or witnessing a traumatic event, can overwhelm a person’s coping capacities, thereby eliciting feelings of fear, helplessness, hopelessness, and feeling out of control. 1 Healthcare encounters can mirror traumatizing experiences within a carceral setting through restrictions on autonomy or self-determination, power differentials, challenges to an individual’s sense of psychological or physical safety, and lack of privacy and/or limited confidentiality. 19 Trauma reactions can include overly anxious or fearful behavior, hypervigilance, increased startle responses (hyperreactivity), physiological distress, feeling numbed or detached, strained communication, and difficulty trusting healthcare providers. 19 Healthcare professionals may not recognize this range of trauma reactions in their patients or know how to effectively respond; they may feel frustrated, unprepared, or uncertain about how to deliver effective care. 20 They may also have limited knowledge about reentry challenges. Further, some medical providers may exhibit negative attitudes toward individuals experiencing reentry based on stigma or lack of understanding. 21
Trauma-Informed Care (TIC) is a treatment philosophy and practice that equips providers to recognize the high prevalence of trauma in society and trauma’s impact on health and functioning, and apply this knowledge to inform care delivery.1,11 TIC describes how trauma-based behaviors can be misinterpreted (eg, as volitional resistance, noncompliance with care recommendations) and exacerbated, to the detriment of patients and staff alike. 5 TIC promotes the physical and psychological safety of patients, providers, and staff; fosters opportunities for collaboration and patient empowerment; advocates for transparency across interactions; and values patients’ unique experiences. 1 TIC improves patient care and satisfaction and reduces burnout in healthcare professionals. 22 TIC encourages providers to practice “universal trauma precautions” by delivering care with the expectation that any patient, regardless of presentation, may have a trauma history. 1
Across the United States, more than 20 states have requested Medicaid Reentry 1115 waivers to temporarily waive the federal prohibition on Medicaid coverage during incarceration (ie, Medicaid Inmate Exclusion Policy) and provide Medicaid coverage of healthcare and care coordination services up to 90 days prior to release.23,24 As the leading evidence-based model for reentry care transitions was developed in a primary care setting, 25 primary care providers should expect an increased demand to participate in reentry care transitions during the implementation of Reentry 1115 waivers. Although TIC training has increased, training practices vary, and TIC is not yet a universal standard of care. 26 Efforts to integrate TIC into standard practice have occurred in primary care,27 -32 but these TIC trainings typically do not focus on the specialized contexts and lived experiences of highly stigmatized populations, such as individuals with a history of incarceration. To address this training gap, the authorship team developed and evaluated a single-session pilot training to prepare primary care teams to deliver TIC to patients experiencing reentry with the goal of enhancing providers’ knowledge, attitudes, and confidence in delivering TIC to formerly incarcerated individuals.
Methods
Design and Approach
The single-session TIC training was developed as part of a larger qualitative improvement (QI) project deemed non-human subjects research by the Dartmouth Health Institutional Review Board. Briefly, the larger QI project was funded by the Susan & Richard Levy Healthcare Incubator, which equips multidisciplinary teams to pursue rapid, sustainable, scalable, and transformational healthcare redesign. 33 The project aimed to improve the reentry care transition process for adults released from state prisons in New Hampshire (NH), a state with a then-pending, now-approved Medicaid Reentry 1115 waiver. 23 The QI team met weekly via teleconference (ie, Zoom) from January 2023 to December 2023 with a 4-phase human-centered design process that included: (1) team formation and project initiation, (2) exploration and diagnosis of the targeted problem, (3) community-partnered intervention design, and (4) sustainment (ie, identifying strategies to scale the intervention with fidelity and stable funding streams).
During phase 1, the team defined the problem as:
Adults returning to the community after incarceration experience unexpected difficulty connecting to healthcare and social resources and are at risk for lowered quality of life,
During phase 2, the team used several methods to identify targets for improvement, including: 19 community interviews with 29 staff recruited from NH state prisons, community-based clinics, and social service organizations; secondary analysis of 19 interviews with adults exiting NH prisons and jails; project feedback meetings with representatives from multiple systems (eg, healthcare, carceral, and social services); and project feedback meetings with team members with lived experience of incarceration. These methods identified 2 priorities for reentry: (1) the need for a primary care-based reentry care clinic, and (2) healthcare staff TIC training. For phase 3, the team formed 2 subgroups to address these priorities. This paper describes the activities of the TIC training development subgroup, which included a peer support specialist (RS), legal advocates (JL), health services researchers (MAY, SHB, and AAM), a reentry case manager, and a family physician-researcher specialized in reentry care (MFS); this group included 3 members with lived experience of incarceration (2 of whom are social service professionals). A clinical psychologist with TIC expertise (LES) led the training development. The subgroup met weekly for an hour during October and November 2023 using a participatory process that leveraged the specific expertise of the team and proactively invited input from all perspectives.
Through iterative design of training objectives and learning approaches, the team created a single-session, 60-min training that included a PowerPoint presentation, interactive panel discussion, and an opportunity for questions and answers (Table 1). The training incorporated the Substance Abuse and Mental Health Administration’s 4Rs framework, 1 which describes the 4 assumptions essential to TIC:
Single-Session Training Objectives and Learning Approaches.
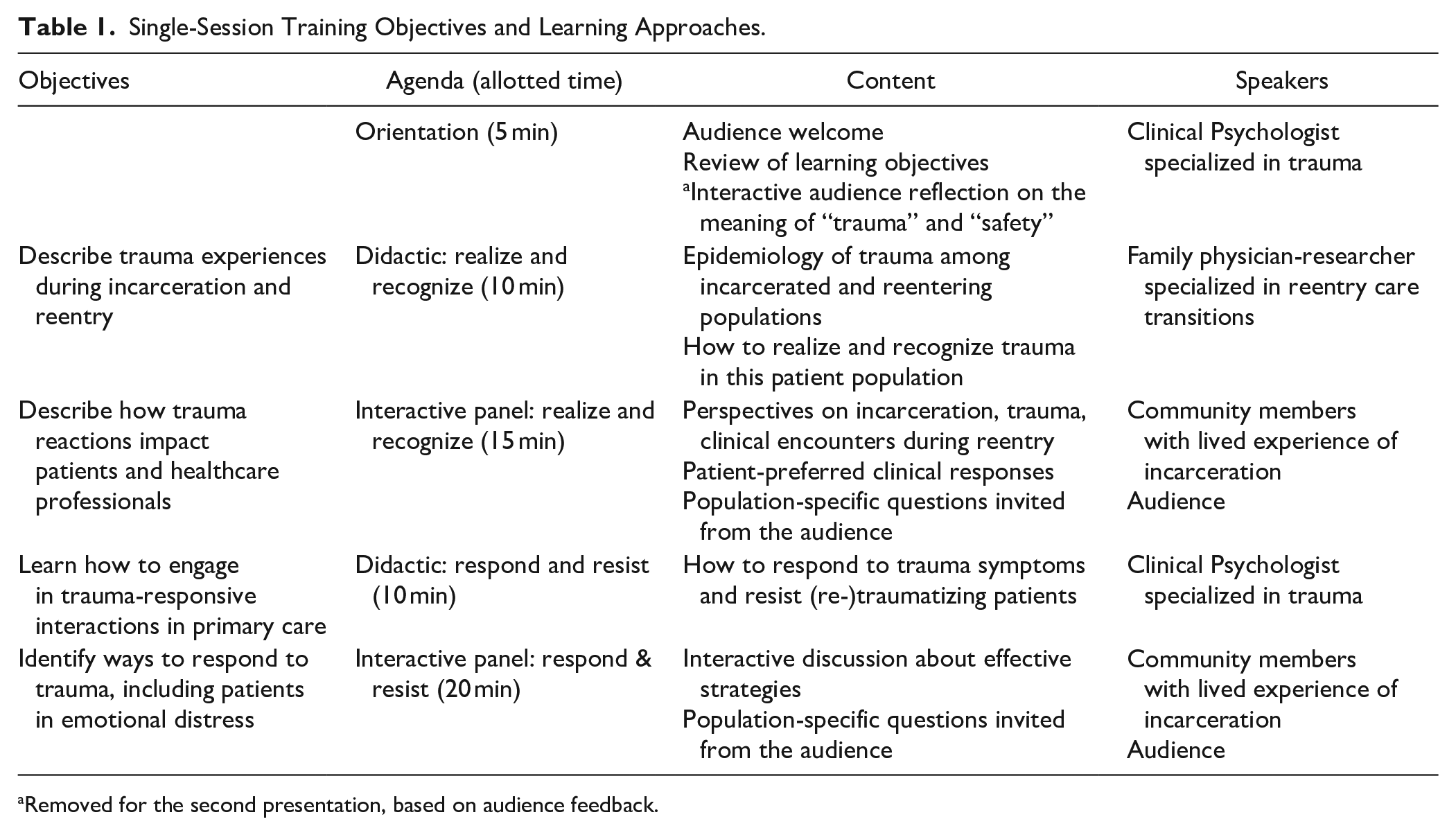
Removed for the second presentation, based on audience feedback.
The training design drew upon the subgroup’s lived experience of traumatic clinical encounters during reentry, clinical expertise regarding trauma symptomatology and management, research expertise on the epidemiology of trauma across the lifespan of incarcerated populations, experience with primary care staff’s existing workflows and priorities, and communications expertise on presentation style and interactivity.
Non-subgroup primary care staff, including a nurse care manager and clinical provider, reviewed iterations of the training to provide target audience feedback. After reaching team consensus on the content and delivery, 4 members of the TIC training development subgroup—including a clinical psychologist, 2 social service professionals with lived experience of incarceration, and a physician specialized in reentry care—collaboratively rehearsed the training and received feedback prior to delivering the pilot training.
Population and Recruitment
The TIC training targeted primary care staff with direct patient-facing interactions and/or administrative influence over such interactions at 2 existing venues for primary care staff: (1) an all-staff primary care departmental meeting held monthly at the NH clinic within which the main QI intervention (primary care-based reentry care clinic) was about to be introduced and (2) an annual conference for primary care practices within Northern New England (ie, Maine, New Hampshire, Vermont, and northern Massachusetts). At least 40 individuals attended at the first venue (NH primary care clinic), including front desk staff, clinical providers, support staff, and administrators, among whom 3 were members of the larger QI project team. Based on attendee feedback, the team completed a minor revision of the training (ie, removed the 3-min interactive audience reflection on “what is trauma/safety?” from the beginning of the presentation); otherwise, the training format and content was retained. At the second venue (regional primary care conference), registered conference attendees received the conference schedule in advance and were able to sign up in advance for the TIC training or join without reservation on presentation day. Registered conference attendees had the option to attend the TIC training, a separate workshop about medical trauma, or not attend either. At least 20 clinical providers, support staff, administrators, primary care researchers, and medical students attended the TIC training at the second venue. No attendee limits were imposed for either venue.
Surveys
At each venue, attendees were invited to complete pre- and post-surveys that were designed to assess prior exposure to trauma-informed care trainings, self-rated confidence in the ability to practice the 4Rs, and an abbreviated version of the Attitudes toward Prisoners Scale. 34 The latter was adapted to focus on reentry populations while balancing positively and negatively worded items; this abbreviated version is herein referred to as the Scale of Healthcare Attitudes toward Returning Persons (SHARP). The post-test survey also assessed interest in additional training in TIC and reentry care and provided an opportunity to share feedback about the single-session training.
The survey data were collected and managed using REDCap electronic data capture tools hosted at Dartmouth Health35,36 with an identical paper-based version also available. At the first venue, the nurse care manager overseeing primary care departmental staff meetings distributed the REDCap surveys via email to the full department listserv once before and twice after the single-session training; additionally, the presenters shared quick-response (QR) codes and short-text links to the surveys on the first and last PowerPoint slides. At the second venue, attendees were given the option to access the pre- and post-surveys via QR codes displayed on the PowerPoint slides or paper handouts of the survey.
Analysis
Descriptive statistics were used to describe respondents’ roles and characterize the frequency of exposure to prior TIC training; familiarity with incarcerated individuals; and confidence in recognizing, responding to, and preventing re-traumatization in patients. Responses of “not at all confident” and “not very confident” were considered to reflect a lack of confidence, and responses of “somewhat confident” and “very confident” were considered to reflect confidence. Responses to questions about confidence were also scored from 1 to 4, with higher scores reflecting a greater level of confidence. A summary confidence score was calculated using the average of the 3 questions about confidence. The SHARP scale was scored the same as the Attitudes toward Prisoners Scale, with each item scored from 1 to 5, with higher responses indicating more positive attitudes. In addition, a total score was calculated as the sum of the 9 items adapted from the original scale. The 2 newly created items about healthcare access and resources were similarly summed, with a separate summary score calculated for these 2 items. Assumption testing (ie, evaluation of histogram, skewness, and kurtosis) was conducted for each confidence and SHARP item and average/composite scores to assess the distribution of differences for paired data. For all variables except 3 sub-items of the SHARP scale, the distribution of differences sufficiently approximated a normal distribution, supporting the use of paired t-tests to assess the impact of the single-session training on attendee confidence and attitudes. To ensure appropriateness of the parametric test results, the analysis of paired data was repeated using the non-parametric Wilcoxon signed rank test which yielded the same results as the paired t-test. For ease of interpretation, paired t-test results are reported. A P-value <.05 was considered statistically significant. Statistical analyses were conducted by SHB using SPSS and rerun independently by MFS using Stata to ensure reproducibility.37,38
Results
Training Attendee Characteristics and Baseline Confidence and Attitudes
Across the 2 deliveries of the single-session TIC training, at least 60 individuals attended and 34 individuals completed the pre-training survey, referred to as the baseline survey. Most respondents participated in the primary care department meeting, just over half had clinical roles, half had no prior training in trauma-informed care, and approximately two-thirds had a personal connection with someone with a history of incarceration (Table 2).
Baseline Characteristics of the Single-Session Trauma-Informed Care (TIC) Training Participants.

Respondents could endorse more than 1 response so totals are greater than 100%.
At baseline (n = 34), the highest percentage of respondents endorsed confidence in recognizing signs and symptoms of trauma (62.5%), followed by 51.6% who endorsed confidence in responding to signs and symptoms of trauma, and 42.4% who endorsed confidence in preventing re-traumatization (Figure 1). Average confidence scores reflected this same pattern, with mean recognition scores of 2.63, responding 2.55, preventing re-traumatization 2.29, for a summary score of 2.52, with higher scores reflecting a greater level of confidence.

Baseline and post-training trauma-informed care confidence.
In general, attitudes toward persons with a history of incarceration were positive, with average scores on the individual items ranging from a low, least favorable attitude, of 3.44 for the item indicating, “You have to be on your guard with people with a history of incarceration” to a high, most favorable attitude, of 4.56 for the item, “Trying to rehabilitate people with a history of incarceration is a waste of time and money.” Beliefs about priority access to healthcare and resources to support reintegration for individuals recently released from incarceration were generally positive. The summary score for the 9 items was 34.75, which is equivalent to an average individual item score of 3.86 (Table 3).
Baseline Confidence and Attitudes Scores—All Respondents (N = 34).

Abbreviations: M, mean; SD, standard deviation.
Reverse-scored items.
Baseline written comments in the pre-training survey expressed a range of attitudes, some of which are included verbatim as written by the participants; for example, 1 attendee stated,
Prison systems in other parts of the world show that recidivism CAN be reduced and made almost a nonissue if incarcerated individuals are given adequate support to establish themselves after incarceration.
as compared to another respondent who shared,
Just because you’ve been incarcerated doesn’t mean you should have preferential treatment over anyone else struggling to better themselves. They got where they were by their own actions and choices.
Post-training Confidence and Attitudes
Nineteen participants completed post-training surveys, among which approximately 94% expressed confidence in recognizing and responding to signs and symptoms of trauma and preventing re-traumatization (Figure 1). Twelve out of 19 post-test respondents could be matched from baseline to post-training to examine changes in confidence and attitudes following the single-session TIC training (Table 4). Among this small sample size of paired surveys, there was a statistically significant increase in both confidence in preventing re-traumatization and the composite confidence score from baseline to post-training. There was also a statistically significant improvement in attitudes toward returning persons, as indicated both by the individual item, “People with a history of incarceration should be under strict, harsh discipline” and by the composite measure. Attitudes toward priority access to healthcare and resources to support reintegration remained stable before and after the training session.
Changes in Confidence and Attitudes Following Training (N = 12).

Abbreviations: M, mean; SD, standard deviation.
Bolded P-values denote statistical significance (P < .05).
Reverse-scored items.
Training Feedback and Interest in Future Trainings
Qualitative comments in the post-training survey were overwhelmingly positive, with multiple respondents indicating that the most valuable part of the single-session TIC training was the speakers with real-life/lived experiences who were,
fantastic and informative.
Several expanded on this feedback; for example,
Their lived experiences and testimonies are powerful when trying to expand on trauma informed care. It allows people to hear a different perspective and to see that success can come after incarceration.
Several survey respondents also indicated appreciation for the discussion specifically around experiences with healthcare and that the presentation:
really stressed the importance of always approaching each person in good faith and to assume good/neutral intentions in all interactions.
One respondent indicated their appreciation,
Most of us have no knowledge of how inmates are treated. That knowledge is so helpful in allowing the care team to anticipate what may trigger them. Thank you for being so honest with us.
One respondent noted the focus on lived experience as a high-impact strategy for a one-hour session:
I thought it was impactful to show the lived experience of incarceration and trauma and provide the facilitation to hear towards healthcare. I thought this was very effective for an hour session.
All respondents who answered the question about interest in future training (n = 17) indicated being interested in future training on trauma-informed care; 16 were interested in receiving more training specific to the needs and care of persons with a history of incarceration. Suggestions for future training included wanting to learn more about incarceration-related trauma and strategies or communication approaches for responding to patients who show trauma-related stress/agitation.
Discussion
This evaluation suggests that primary care provider and staff training in reentry-specific TIC—even as a single session—may be effective at improving both confidence in care for and attitudes toward individuals with a history of incarceration. Trainees reported significant increases in confidence to reduce potentially re-traumatizing practices and improved attitudes toward formerly incarcerated individuals. In particular, the statistically significant decrease in trainees’ preference for strict, harsh discipline (SHARP item 6) suggests an improved recognition of the traumatizing aspects of the harsh, punitive processes enacted within our U.S. carceral systems. Trainees also expressed interest in additional TIC training including how best to care for and meet the needs of persons with a history of incarceration.
The most notable finding from this pilot training is that centering those with lived experience as part of the training design and delivery can optimize the learning experience. Trainees described the panel of community members with lived experience as one of the most rewarding aspects of the training. Lived experience perspectives can offer insights into real-life challenges and needs, provide a nuanced and accurate picture of the complexities of trauma and incarceration, and challenge preconceived notions and biases. 39 Moreover, co-designing training with people with lived experience can deepen learning for both trainers and trainees, empower those with lived experience, and leverage their expertise. Our findings are consistent with studies that have shown that medical education opportunities that center lived experience and are co-developed with persons with lived experience can increase humanization, empathy, accuracy of experience, appreciation of the gravity of experience, and promote shared understanding. 40 Including individuals with lived experience in TIC training can dispel myths and stigma about those affected by incarceration. 41 Co-design and co-delivery of such trainings may also serve to model a shared understanding and openness to learning from those with lived experience, which are foundational to a collaborative and trusting patient-provider relationship. 42
Attitudes toward priority access to healthcare and reintegration resources (eg, housing and transportation) for people recently released from incarceration were generally positive at baseline and after attending the TIC training. This suggests most attendees hold stable positive beliefs about individuals’ right/access to healthcare, while some may believe priority access to this patient group is unfair. This training did not emphasize or directly target beliefs about healthcare engagement, which may additionally account for these stable responses.
Regarding limitations, this pilot did not include long-term, systematic measurement of practice change/implementation of TIC in practice providers who attended the training versus those who did not. Additionally, not all training attendees offered survey responses; those who completed the survey may have been more interested and/or experienced in caring for patients with trauma and/or incarceration histories than those who did not. Additionally, there were challenges in pairing pre-test and post-test results, resulting in a small sample size of paired individuals. Demographic data for respondents were not collected, preventing an ability to explore if the single-session TIC training is better suited to certain groups. Finally, the adapted SHARP instrument was not validated prior to administration. Despite these limitations, this evaluation demonstrated that TIC training that is co-produced and co-delivered with persons with lived experience can improve attitudes toward formerly incarcerated individuals. Further, given that half of the respondents had no prior TIC training, this training addressed a key gap.
Lived experience perspectives can enhance the learning environment and address current gaps in TIC training. These perspectives can promote measurable learning improvements, enhance empathy and understanding, and ultimately foster a compassionate approach to care. Individuals with lived experience can offer valuable insight into understanding the intersection of trauma and incarceration and the impact on health and functioning, as well as practical advice and strategies that have worked for them, which providers can then integrate into their TIC practice.
Conclusions
A single-session TIC training that integrates lived experience perspectives, pragmatic knowledge, theory, and application can be well received by and can enhance primary care provider and staff readiness to provide care to populations experiencing reentry. With the expansion of healthcare financing for reentry care transitions—supported by Medicaid Reentry 1115 waivers23,24—and existing and forthcoming guidance from primary care-based reentry care transition models,25,43,44 primary care can lead the way in preventing further harm to patients who have experienced incarceration. TIC training can move primary care providers and staff from being merely informed on trauma to having the self-efficacy to prevent and respond to trauma reactions during encounters with all patients, particularly those with a history of incarceration. It will be essential to identify effective strategies to broadly deliver such TIC trainings and evaluate their impact on healthcare engagement, health outcomes, and community reintegration.
Footnotes
Acknowledgements
The authors wish to thank all members of the trauma subgroup of our quality improvement team as well as the clinical subgroup members for their supportive input during the development and delivery of this training. We also thank the many patients, community members, and loved ones we have encountered over the years whose lived experiences with criminal legal systems and healthcare environments informed this work.
Author Contributions
All authors conceptualized the training. LES and MFS designed the surveys and developed the manuscript outline with feedback from all co-authors. LES, MAY, and MFS contributed to the literature review. SHB and MFS conducted the survey analysis. LES, MAY, SHB, AMA, and MFS contributed to the drafting of the manuscript. MAY finalized the manuscript citations and formatting. SHB, JL, RS, AMA, and MFS conducted a detailed review of the drafted manuscript and provided critical revisions. All authors read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Susan & Richard Levy Healthcare Incubator at Dartmouth College and Dartmouth Health. Dr. Satcher’s effort was additionally supported by a National Institutes on Drug Abuse training grant (R25DA037190), and a Health Resources and Services Administration training grant (T32HP32520). The funders played no role in the study design, data collection, analysis, and interpretation of data, or the writing of this manuscript.
Ethical Approval and Consent to Participate
The Institutional Review Board at Dartmouth Health reviewed this project and deemed it a quality improvement effort that was not human subjects research. The project was performed in accordance with the Helsinki guidelines and declarations.
Consent for Publication
Not applicable.
Data Availability Statement
Data may be made available by Dr. Milan Satcher upon reasonable request.