
Abstract
In response to persistently low enrollment in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) across Tennessee, the WIC Champions group conducted a statewide survey to evaluate healthcare providers’ practices and barriers in screening for food insecurity and referring patients to WIC. The survey, conducted from November 2023 to February 2024, included 70 diverse healthcare professionals across 28 Tennessee counties. Findings revealed that 88% of providers screen for food insecurity and 95% believe it is vital to patient health. However, only 67% felt familiar with local resources for referrals, and significant barriers including limited staff, time, and resource availability were reported. Despite 90% of respondents being familiar with WIC, only 39% made direct referrals, with many relying on less structured methods such as verbal encouragement or providing contact information. Surveyed providers identified the need for improved outreach materials, better integration with electronic health records, and dedicated referral staff. The findings highlight the critical role of healthcare settings in addressing food insecurity but underscore systemic barriers that impede effective WIC referrals. Enhanced support, training, and infrastructure are necessary to empower providers and expand WIC access, aligning with key national strategies to combat hunger and improve public health outcomes.
Introduction
In 2023, 47.4 million individuals in the US reported living in a household experiencing food insecurity. 1 Healthcare providers can play a crucial role in screening for social needs and connecting patients to community and government resources. While many pediatricians are motivated to screen for food insecurity and other social needs, there are structural barriers to conducting screening. 2 Physicians expressed concern about knowing how to handle a positive screen. However, even when a family is referred, there can be a gap in referral acceptance and ultimate connection with food resources. This highlights the need for evidence-based interventions for resource engagement.3,4
Food insecurity disproportionately affects vulnerable groups, such as women and children, contributing to maternal health complications, poorer pregnancy outcomes, and incidences of depression. 5 In 1972, the federal government launched the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) to support the nutritional health of these groups, specifically low-income pregnant, breastfeeding, and postpartum women, as well as infants and children aged 5 years and below.6,7 Studies have shown that WIC enrollment is associated with better birth outcomes, decreased incidence of mental health issues in childhood, and improved school performance.8,9 However, despite these known benefits, WIC resources are often underutilized in marginalized communities.
In 2021, the United States Department of Agriculture reported that over 12 million individuals were eligible for WIC benefits each month; however, around 50% of these eligible individuals did not receive them. 10 In the state of Tennessee, only 41% of eligible individuals were enrolled in WIC in 2021. 11
The impetus for this survey was a partnership known as the WIC Champions group, which is a state-wide collaborative including food security advocates and all those who serve WIC-eligible clients in Tennessee. The USDA WIC Community Innovation and Outreach Grant sponsored the WIC Champions workgroup, which aims to increase enrollment in the Tennessee WIC program. To better understand current WIC referral practices in primary care settings, the WIC Champions group surveyed healthcare providers in Tennessee on how and to what extent they conduct social needs screenings and connect patients to WIC and other food resources in their communities. This report discusses the survey results and outlines strategies and recommendations to enhance WIC referral and enrollment in Tennessee.
Methodology
Eligibility and dissemination: For this survey, we engaged a cross-sectional group of healthcare professionals, including physicians, nurses, nurse practitioners, social workers, front desk staff, midwives, lactation consultants, and medical assistants. Recruitment occurred among providers who interacted with women and children, served a low-income population, or conducted social needs screenings. We recruited respondents who were healthcare personnel from the Tennessee WIC Champions group, the Cumberland Pediatric Foundation, the Memphis Pediatric Foundation, and the Tennessee Charitable Care Network. Our survey assessed the prevalence of practitioners screening for social needs, specifically whether they screen for food insecurity. If they conducted social needs screening, we attempted to determine who was making connections to local resources and how they were achieved.
The online survey was modeled after a similar survey of healthcare providers addressing food insecurity among adults, sponsored by the Food Resource Action Council in 2023. 12 Our survey was adapted to reflect our focus on connections to the WIC program. Our survey, conducted from November 16, 2023, to February 15, 2024, was a comprehensive assessment of providers’ attitudes and current practices regarding social needs screening and referrals in their respective settings. It was administered by an email link to participants in the aforementioned healthcare provider groups, submitted anonymously, and had a reach of over 400 providers. The survey response rate was approximately 17%. The survey took 5 to 10 min to complete and had 15 questions. There was no remuneration for participation in the survey. Some questions allowed multiple answers, and some permitted free-text responses, ensuring a thorough understanding of the subject.
The survey utilized RedCap (Research Electronic Data Capture), a secure web-based application that helps researchers collect and manage data for research studies. This platform ensured the confidentiality and integrity of the data collected. Our team sent the survey by email to healthcare professionals across the state of Tennessee. The questions assessed how providers felt about screening for social needs, which categories of needs they screened for (housing, food, etc.), and how they connected patients to community resources. We also evaluated healthcare providers’ knowledge of and referral practices to the WIC program.
We used descriptive statistics to summarize provider-reported responses. Because respondents could select multiple responses in some questions, we calculated the percentage of total respondents who endorsed each category. For each item, the count represents the number of respondents who selected that option, and the corresponding percentage reflects the proportion of the total sample that selected that item. Percentages do not sum to 100% because of the multiple-response format. All analysis was conducted using Microsoft Excel. No inferential statistical tests were applied, as the study was descriptive in nature.
Respondent demographics
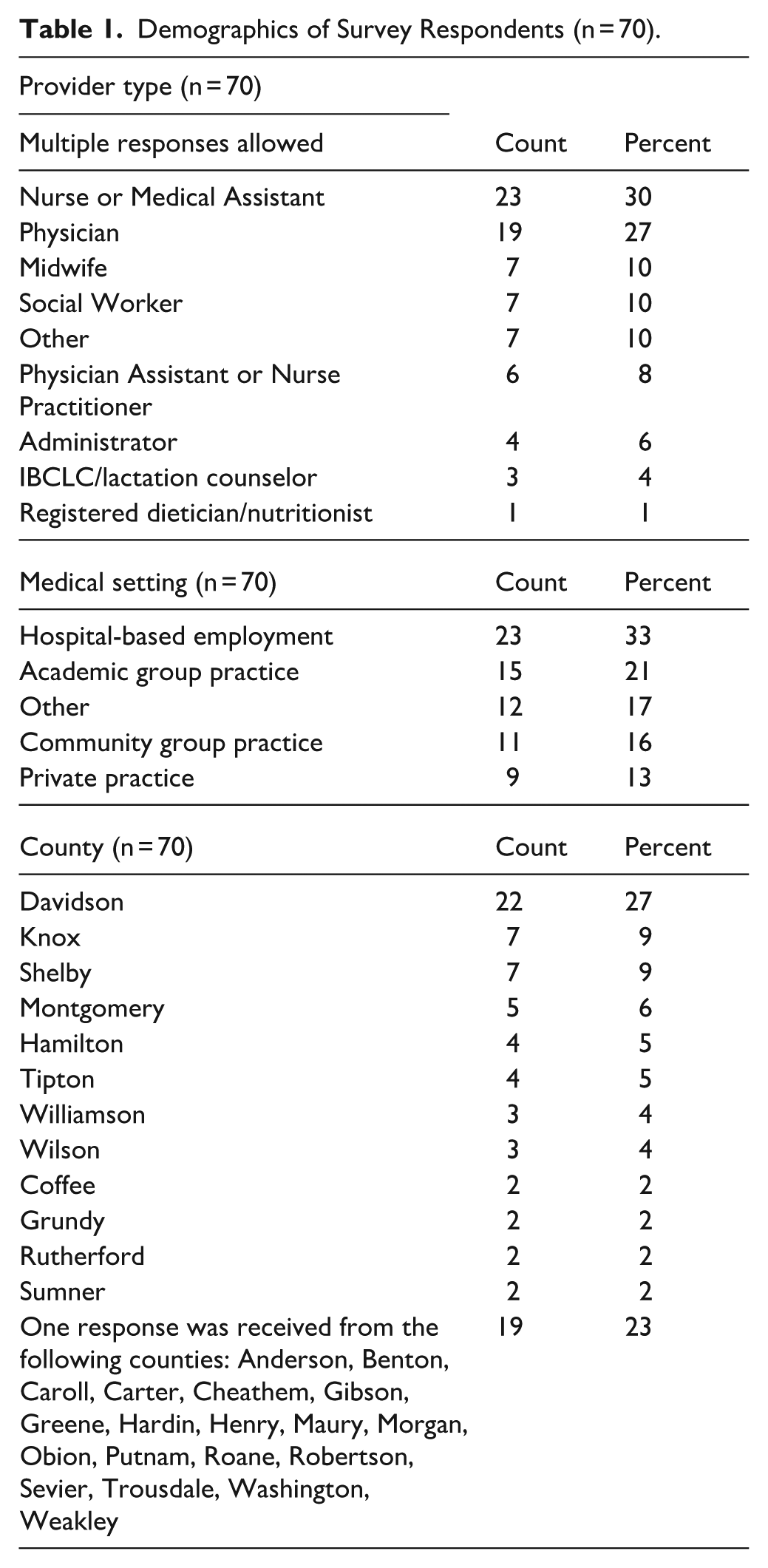
Seventy individuals responded to the survey, including all respondents in the analytic sample. As detailed in Table 1, our survey included a diverse group of healthcare professionals, reflecting the multidisciplinary nature of patient care. Twenty-three nurses, 19 physicians, 7 social workers, 7 midwives, 6 nurse practitioners, administrators, lactation counselors, nutritionists, medical students, community health workers, and doulas responded to the survey. Respondents represented primarily academic or hospital-based settings, with some experience in small community clinics. The sample included 28 counties clustered in the major metro areas of Nashville, Knoxville, Memphis, Clarksville, and Chattanooga.
Demographics of Survey Respondents (n = 70).
Results
Seventy-seven percent of respondents’ practices accepted Medicaid (TennCare) in their practice settings. Respondents were also asked if their practice performed social needs screenings. 81% of respondents selected ‘yes’ to the fact that they performed social needs screenings, 9% selected ‘no’, and 10% were ‘unsure’ if their practice performed screenings.
Table 2 illustrates the variation in responses regarding who among their staff responds to positive social needs screening in the clinic. More than 50% of the respondents selected that social workers respond to positive social needs screenings in their clinics. ‘Other’ was selected by 32% of respondents, and those who selected this choice had the option to write in a response. The written text responses provided by the respondents included those from case managers, community health workers, educators, and benefit specialists.
Position Responding to Positive Social Needs Screenings (n = 57).

The next question asked whether respondents screen patients for various social needs, including access to childcare, education and literacy, financial insecurity, food insecurity, housing insecurity, personal safety, transportation, and utility strain. The type of visit where the screening occurred was open and not limited.
As shown in Table 3, 88% of respondents reported screening patients for food insecurity. Other social needs, including personal safety, housing insecurity, transportation, and financial strain, were screened for over 50% of the time.
Social Needs Screened for at the Provider’s Practice (n = 57).

To assess their attitudes regarding screening for social needs, healthcare providers were asked if they agreed with the statement, ‘Healthcare providers play an important role in screening for social needs’. They overwhelmingly expressed their commitment. Over 95% of providers agreed or strongly agreed with the statement.
Respondents were also asked about screening for food insecurity specifically and its importance to overall patient health. As shown in Figure 1, 95% of respondents agreed or strongly agreed with the statement ‘Screening for food insecurity is an important measure to promote patient health and well-being’.
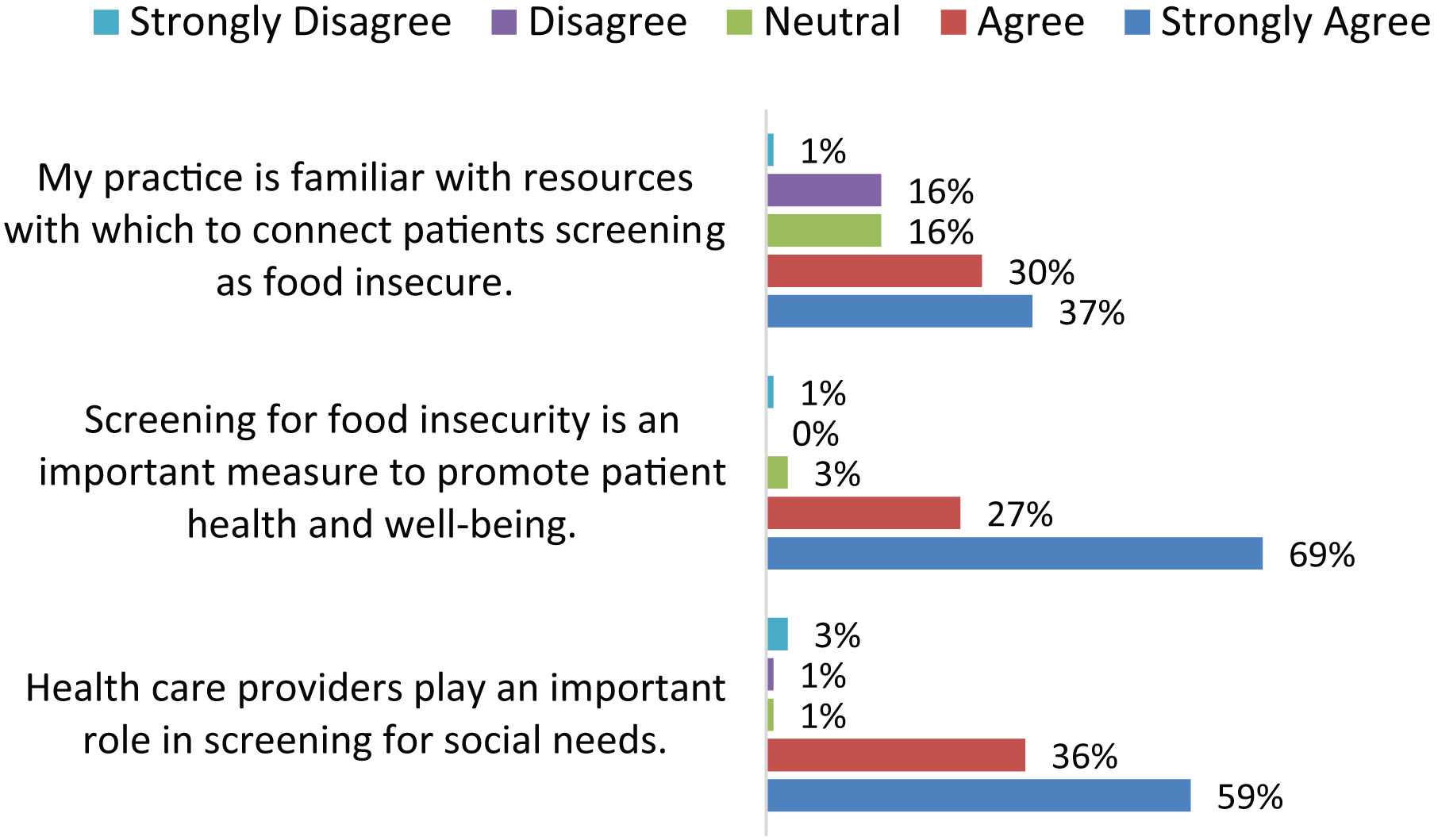
Attitudes and comfort with screening and referrals among healthcare providers (n = 70).
Survey respondents overwhelmingly understand and agree with the importance of screening for social needs. However, survey results show that healthcare providers are not always knowledgeable about resources with which to connect patients who are food insecure.
In assessing knowledge, only 37% of respondents strongly agreed that they felt familiar with local resources to connect patients who screened positive for food insecurity, as shown in Figure 1. About one-third of respondents disagreed or were neutral about whether their practice was familiar with resources to connect patients who screened positive for food insecurity.
Table 4 shows that the barriers most frequently faced by practitioners screening for social needs are the limited availability of resources to offer patients, the limited time available to counsel and connect patients with resources, and the limited staff available to provide resources to patients.
Barriers to Screening for Social Needs (n = 70).

In our following questions, we attempted to examine referrals to local food programs such as the Women, Infants, and Children (WIC) program. Regarding the WIC program specifically, 90% of respondents were familiar with it and encouraged patients and families to participate. The few respondents who did not actively refer to WIC served a patient population that was most likely not eligible for WIC, such as serving an older patient population or having a clinic in a more affluent community where patients may not qualify.
Many healthcare providers in Tennessee are encouraging their patients to enroll in the WIC program. Respondents were asked how they encouraged their patients to enroll in the WIC program. As shown in Table 5, the various modalities in which providers encouraged WIC participation were:
Ways Providers Encourage WIC Participation (n = 57).
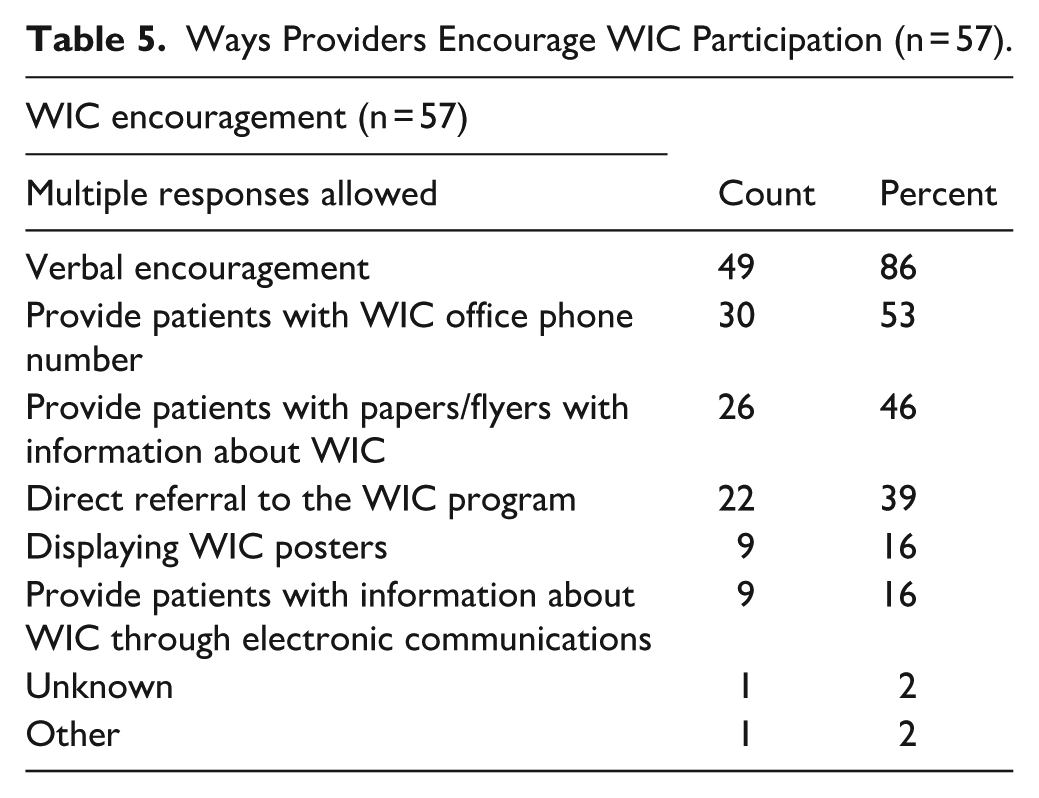
Verbal encouragement
Providing the WIC office phone number
Providing papers or flyers with WIC information
Direct referrals.
Respondents showed that they refer their patients to WIC in various ways.
As shown in Table 6, the various modalities in which providers made WIC referrals included:
Providing a phone number
WIC information provided to patients through electronic communications
In-clinic support with social workers
Referring patients to a local agency/community resource to facilitate connections to WIC
Electronic referrals.
However, 28% of respondents selected ‘NA’ or were not referring patients to WIC, and 9% were unsure if their practice did referrals. This may demonstrate that many providers lack understanding of potential WIC referral methods for connecting patients to the program.
Different Healthcare Providers’ WIC Referral Methods (n = 57).

Recommendations
Various suggestions were obtained from healthcare providers in free text comments in the survey and from the larger WIC Champions group on what would be helpful, including
Updated WIC flyers to be available for all their offices and a database of WIC clinics in more rural areas.
A dedicated WIC outreach office in larger metropolitan areas could assist with connecting patients to the WIC program.
Dedicated staff in the clinic who coordinate WIC referrals or
Direct contact at a local agency to facilitate WIC referrals.
Improved communication with the local WIC office to understand programmatic rules and requirements.
In technical assistance, a suggestion for an online training session for case managers, social workers, or other clinic personnel, like a webinar, would help smaller clinics develop screening and referral programs tailored to their specific setting. A referral mechanism that integrates with a clinic’s electronic health record would facilitate the process and save time and labor.
Limitations
Several limitations to this survey should be acknowledged. First, our sample size was relatively small and may not be representative of the larger primary care population of healthcare providers in Tennessee. Second, we could have employed qualitative methods in more detail and conducted interviews to assess healthcare providers’ perceptions of the most effective methods for making WIC referrals. Our survey did not explore various modalities for the practical identification of patients who qualify for the WIC program or address referrals for other social needs.
Conclusion
At present, 1 in 7 Tennesseans experience a degree of food insecurity. 13 Our survey results demonstrate that across a range of healthcare professions, there is a uniform consensus that screening for food insecurity is vital to ensuring patient health and well-being. While most respondents reported that their practices screen for food insecurity, many providers indicated they were constrained by time and staff availability to perform and respond to these screenings. These barriers were consistent with findings from other studies. 2 Also, over a third reported unfamiliarity with local resources to connect patients.
Healthcare providers face numerous challenges in their roles, including limited availability of resources, staff, and time, as well as unfamiliarity with screening and available resources. These barriers can make it more challenging to incorporate a screening for social needs and adequately respond to positive screenings, including food insecurity, in the clinical setting. Practical implementation strategies for social needs screening include using applicable screening tools, having dedicated staff to manage the program, building partnerships with community organizations, and utilizing technology for efficient tracking and referrals. 14 Other strategies identified include having measurable outcomes and payment structures to support such interventions in the pediatric clinical setting. 14
Improvement in WIC enrollment in primary care settings has been studied using quality improvement strategies and has demonstrated its feasibility in reducing barriers to enrollment. 15 Utilizing the Electronic Health Record (EHR) was considered a lower burden for providers than paper screening, as it is more anonymized; however, it can make the process more complex, and providers still encounter barriers to reconnecting with families.16,17 Federal and state initiatives are vital to supporting healthcare providers doing this work and encouraging more healthcare providers to identify and address food insecurity. In 2022, the White House National Strategy on Hunger, Nutrition, and Health released a call to action with clear, actionable strategies to advance connecting people to healthy and nutritious food. The first 2 pillars of the strategy directly address opportunities to strengthen connections to crucial federal nutrition programs, including WIC. These pillars support the increased identification of WIC-eligible individuals at the state level and provide more significant incentives for providers to conduct food insecurity screenings. 18
Food insecurity is a significant public health concern at both the state and national levels. Consequently, investing in improved screening and WIC referral practices will allow providers to better safeguard the health of families across Tennessee.
Supplemental Material
sj-pdf-1-jpc-10.1177_21501319251380489 – Supplemental material for Feeding the Gap: Screening for Food Insecurity and Linking Families to WIC Support
Supplemental material, sj-pdf-1-jpc-10.1177_21501319251380489 for Feeding the Gap: Screening for Food Insecurity and Linking Families to WIC Support by Rosemary Hunter, Sunaya Krishnapura, Anna Grace Breedlove, Anne Dobson Ball and Signe Anderson in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
Not applicable.
Ethical Considerations
The study received ethical approval from Vanderbilt University Medical Center Institutional Review Board IRB#231796 on Nov. 8, 2023.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding statement: This project has been funded in part with federal funds from the U.S. Department of Agriculture with the WIC Community Innovation and Outreach Grant. The contents of this publication do not necessarily reflect the view or policies of the U.S. Department of Agriculture, nor does it mention of trade names, commercial products, or organizations imply endorsement by the U.S. Government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplementary Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.