
Abstract
Food insecurity is a household-level economic and social condition characterized by limited access to nutritious food. This study explored dental practitioners’ views on food insecurity screening and its impact on oral health. A five-question survey (“Quick Poll”) was conducted through the National Dental Practice-Based Research Network (PBRN) in the United States. A total of 332 dental practitioners responded. Preferences for food insecurity screening in dental practice settings showed substantial variability: 30% in favor, 39% neutral, and 29% against. When identifying the primary oral health issue influenced by food insecurity, 68% pinpointed dental caries. Over half (53%) expressed comfort in directing patients experiencing food insecurity to relevant resources. Notably, 61% of respondents expressed interest in being involved in future food insecurity clinical studies. This preliminary study underscores the relevance of food insecurity in the professional dental setting and suggests that the clinical setting may be well suited for educational programs designed to improve the oral health of patients experiencing food insecurity. Future research may achieve this goal, including a PBRN clinical study of interventions to improve oral health among patients experiencing food insecurity.
The Social Determinants of Health (SDOH) model includes conditions in the environments where people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks (U.S. Department of Health and Human Services, n.d.). The importance of SDOH for shaping health and wellbeing necessitates a health care system that proactively engages SDOH (Gurewich et al., 2020). Food insecurity—the limited or uncertain availability of nutritionally adequate and safe foods—(Rabbitt et al., 2023) emerges as a critical SDOH due to its established connections with acute and chronic health conditions (Gundersen & Ziliak, 2014). Considering the widespread prevalence of food insecurity—impacting an estimated 44.2 million people in the United States in 2022—(Rabbitt et al., 2023) and the associated health sequela, it is imperative to incorporate nutrition security strategies into health care and disease prevention.
Emerging literature demonstrates that food insecurity harms oral health because irregular eating patterns and nutrient-poor diets can contribute to an environment where harmful biofilms thrive, and inflammation occurs (Dent et al., 2021). Recent systematic reviews and meta-analyses have found a strong association between food insecurity, dental caries, and poor oral health in children, adolescents, and adults (Drumond et al., 2023; Sabbagh et al., 2023). Considering the connection between food insecurity and oral health, a better understanding of dental practitioners’ knowledge of and views toward food insecurity is needed to foster a more holistic integration of food insecurity screening, service referral, and treatment within dental settings.
In our current study, we report results from a 5-question brief survey (called “Quick Poll”) among dental practitioners who are members of the National Dental Practice-Based Research Network (“Network”; PBRN), an infrastructure supported by the National Institute of Dental and Craniofacial Research. Specifically, the study through this survey aims to understand their views regarding (1) screening for food insecurity as part of the professional dental role, (2) the impact of food insecurity on oral health, (3) comfort in directing patients experiencing food insecurity to services, and (4) interest in participating in future research about food insecurity.
Methods
This study was performed in the Network, a collective of community dental practitioners (i.e., dentists, dental hygienists, and dental therapists) that attempts to bridge knowledge gaps, inform treatment choices, and promote quality through research participation (Gilbert et al., 2022). Dental practitioner engagement in the Network is partly accomplished via Quick Polls, brief surveys that serve as a timely, simple, and cost-effective way to involve members in pertinent clinical issues that require the development of future clinical studies (Mungia et al., 2020).
Distributing a brief five-item survey allows for the prompt gathering of valuable data, ensuring that the perspectives of dental professionals are captured. Due to the rapid nature of Quick Polls, development does not go through a formal validation and pilot testing process that is typical for the Network’s national questionnaire studies. Polls are generated by experts in the subject area that is the focus of a Quick Poll, and feedback is gathered from Network leadership before being disseminated. The process involves defining the Poll’s purpose, brainstorming questions, narrowing it to five questions, drafting clear and concise questions, seeking feedback from Network directors, refining questions based on feedback, and finalizing for deployment to Network members.
Network members were invited to participate in the Quick Poll through email and social media. Accordingly, their responses comprise a nonrepresentative sample of Network members who replied. The Quick Poll email invitations were sent to all members: one in the Network’s monthly newsletter sent on July 21, 2023, and one as a follow-up email sent on July 31, 2023. The Quick Poll was also announced on the Network’s social media accounts (Facebook, LinkedIn, and Instagram) and was open from July 21, 2023 until August 20, 2023. It included these five questions:
Please indicate how much you agree with the following statement: Dental practitioners should screen patients for food insecurity as part of the professional dental role.
On a scale of 1 (very impactful) to 10 (not impactful at all), what impact do you feel food insecurity has on a person’s oral health?
Which oral health issues does food insecurity most impact?
On a scale of 1 (very comfortable) to 10 (not comfortable at all), how comfortable would you feel directing a patient to resources that support people with food insecurity in your local community, such as information on a local food bank or providing information on receiving Supplemental Nutrition Assistance Program (SNAP) benefits?
How interested would you be in participating in a study about food insecurity among dental patients?
The study conformed to the U.S. Federal Policy for the Protection of Human Subjects by obtaining Institutional Review Board (IRB) approval for the Network—National Dental PBRN Administrative & Resource Center, from the University of Alabama at Birmingham (IRB-040903006).
Results
The Quick Poll was sent to all U.S. Network members. It was opened 1,434 times, and 332 respondents completed the Quick Poll. The response rate is unknown because we cannot calculate the number of invitees who were eligible (not deceased and confirmed to be in active clinical practice). A completion rate of 23.1% was calculated by dividing the number of members accessing the link by the number completed. Because some members may have accessed the link multiple times before completing the Poll, this completion rate is a conservative estimate.
Figure 1 represents findings from this survey. Regarding the role of dental practitioners in food insecurity screening, respondents appeared divided: 39% (n = 129) were neutral about the statement, while 30% (n = 100) supported food insecurity screening, and nearly an equal proportion (29%, n = 99) opposed it. On a scale of 1–10, a majority (73%, n = 247) recognized the impact of food insecurity on oral health (responses 1–4). Conversely, a minority of 11% (n = 41) deemed food insecurity as not influential on oral health (responses 7–10), with the remaining 12% (n = 43) maintaining a neutral stance (responses 5–6).
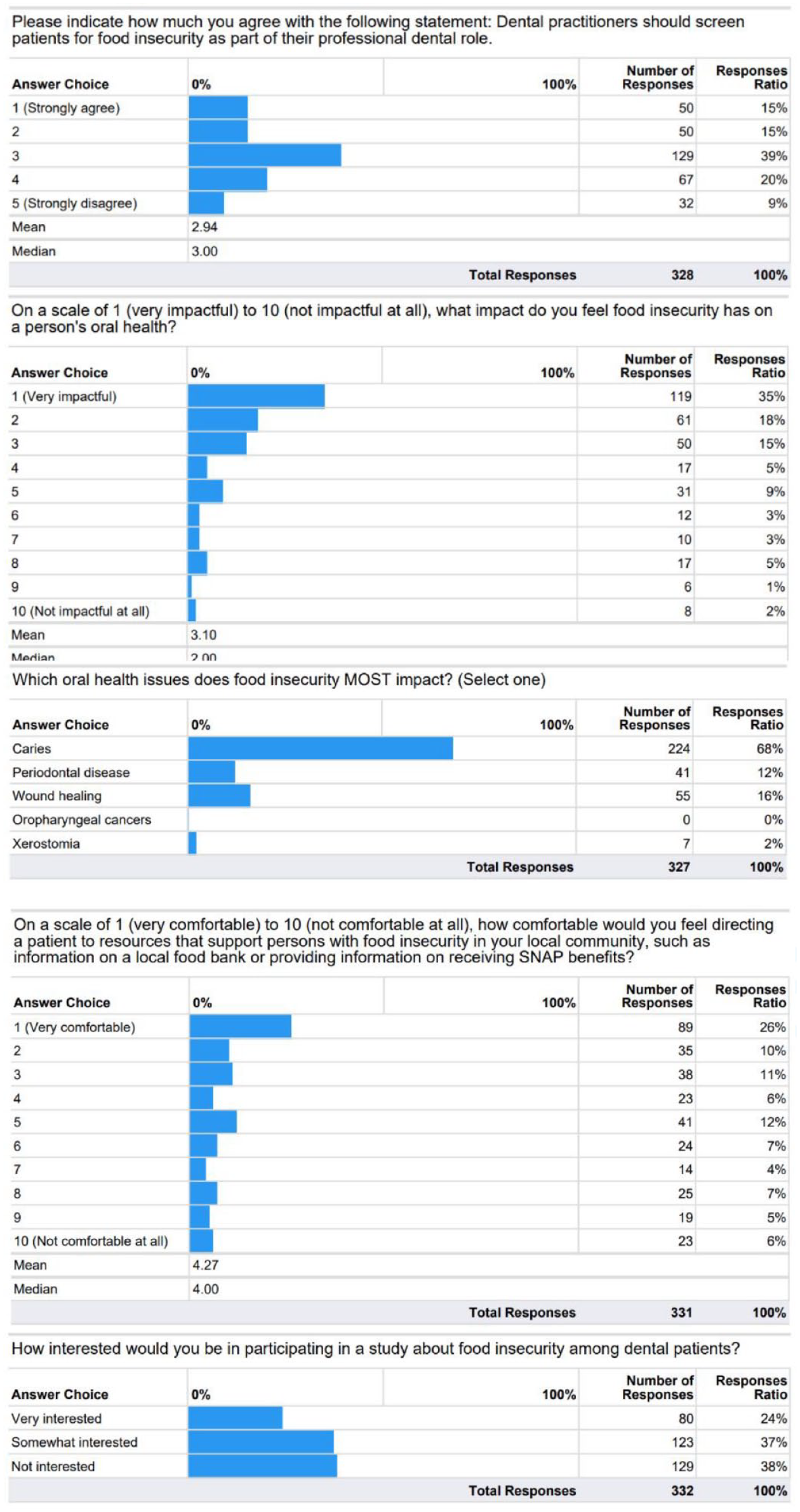
Results of National Dental PBRN Quick Poll
When discerning which specific oral health issue is most exacerbated by food insecurity, dental caries emerged as the primary concern, identified by 68% (n = 224). Other conditions noted included periodontal disease (12%, n = 41), wound healing (16%, n = 55), and xerostomia (2%, n = 7). None selected oropharyngeal cancers.
Approximately, half (53%, n = 185) felt comfortable (scoring 1–4) guiding patients affected by food insecurity to relevant resources, while 19% (n = 65) remained neutral (scoring 5–6), and 22% (n = 81) expressed discomfort (scoring 7–10). Finally, 24% (n = 80) expressed high interest in engaging in future food insecurity-focused research, 37% (n = 123) were moderately interested, and 38% (n = 129) showed no interest.
Discussion
This study provides insight into dental practitioners’ views on food insecurity-related issues, suggesting the following results: (1) mixed opinions about screening for food insecurity in dental practices, (2) acknowledgment of food insecurity’s substantial impact on oral health, (3) identifying dental caries as the primary oral health issue influenced by food insecurity, (4) comfort in directing patients experiencing food insecurity to resources, and (5) mixed interest in future food insecurity studies.
Regarding the findings that many dental practitioners were neutral about food insecurity screening during dental visits, this could be due to a lack of appropriate training or knowledge of the concept. However, straightforward and effective screening tools are suitable for use in a dental practice setting. The Hunger Vital Sign, comprising two items, is extremely sensitive against the 18-item Household Food Security Survey in adult populations (>97% sensitivity and >83% specificity; Gundersen et al., 2017; Hager et al., 2010; Radandt et al., 2018). It was first validated by Hager in a pediatric clinic (Hager et al., 2010), then by Gundersen in adults (Gundersen et al., 2017), and then by Radandt in a pediatric dental clinic (Radandt et al., 2018) and can be better integrated into dental practices to detect food insecurity among patients. Assessing food insecurity screening and detection among broader populations across a range of dental clinics would be a valuable next step. Screening could enable timely detection and intervention by directing patients to resources such as local food pantries and connections with critical public benefits such as SNAP.
Most respondents (53% responded “1” or “2” to the 10-point impact scale) believed food insecurity impacts oral health, especially dental caries. The perception of dental practitioners on the harms of food insecurity for oral health is consistent with findings in the literature demonstrating the oral health sequela of food insecurity (Drumond et al., 2023; Sabbagh et al., 2023), underscoring an important practitioner belief about food insecurity’s role in oral health. Our Quick Poll results showed that, while most dental practitioners felt comfortable directing patients to resources, many highlighted the need for better awareness of available supports. This finding highlights the need for training and knowledge regarding food insecurity and the resources that support persons experiencing food insecurity in dental clinical settings.
Understanding dental practitioners’ perspectives is important for comprehensive public health education and research. Dental professionals are at the forefront of oral health care and offer unique insights into food insecurity (Kane, 2017). Their experiential knowledge can illuminate nuances not readily apparent in quantitative data, guiding intervention design and policy recommendations (Northridge et al., 2020). Engaging practitioners enriches the multidimensionality of research and fosters interprofessional collaboration, which is essential for addressing complex health disparities. Our results indicated varied interest among dental practitioners in future food insecurity studies. This diversity could be attributed to the Quick Poll questions not addressing aspects such as clinic compensation, potential staff involvement (which might act as a deterrent), or assisting in the study’s implementation. Incorporating qualitative data collection in future endeavors can enhance the granularity of information gathered.
Despite the study’s contributions, it is important to highlight a few limitations. Notably, the survey was a one-time snapshot of dental practitioners’ views and should not be considered representative of all practitioners. It was also impossible to determine whether the survey participants were dentists or hygienists, potentially leading to significant response variations based on their professional roles. The study included a selective sample, necessitating future research replication of the findings in a more representative sample. It is also possible that responses were impacted by self-selection and nonresponse bias, given the number who opened the survey compared to the number who completed it.
There were also limitations in the collection and analysis of the data. For example, we know all Network members were sent the newsletter, but there was no confirmation that each had an opportunity to respond. Also, the poll was limited to five questions and lacked details on dental practitioners’ knowledge of food insecurity or their experiences treating oral manifestations. We did not collect demographic characteristics from respondents, precluding the determination of how responses varied by sex, age, years in practice, race/ethnicity, or geographic location. In addition, this limited the ability to assess the sample’s representativeness. Future studies would benefit from collecting demographic questions to understand how perceptions and views toward food insecurity in professional dental practice vary by socio-demographic characteristics.
This preliminary study underscores the relevance of food insecurity in dental settings and highlights the potential for educational programs to improve the oral health of patients experiencing food insecurity. Future research, including a dental PBRN clinical study of interventions, can further this goal. Dental practitioners and public health professionals can take actionable steps such as integrating structured food insecurity screening protocols, partnering with local food assistance programs, and incorporating relevant training into continuing education. The expressed interest in further research provides a strong foundation for comprehensive studies that could lead to improved oral health outcomes and reduced health disparities associated with food insecurity.
Implications for Research and Practice
These preliminary results provide new insight into dental practitioners’ knowledge and views of food insecurity in professional dental practice. Considering the link between food insecurity and poor oral health, these findings underscore the importance of addressing food insecurity in dental practices and the need for enhanced practitioner training. These insights can help shape future dental practitioner-based research and improve care related to food insecurity, including developing educational initiatives. This will further research on food insecurity and oral health within clinical settings.
Footnotes
Authors’ Note:
We are very grateful to the Network Staff (Brittni M Ball, MS), who managed the implementation of the survey discussed in this article, along with network practitioners who participated in the study. This work was supported by NIH grant U19-DE-28717. Opinions and assertions contained herein are those of the authors and are not to be construed as necessarily representing the views of the respective organizations or the National Institutes of Health. An internet site devoted to details about the Nation’s Network is located at ![]() . The informed consent of all human subjects who participated in this investigation was obtained after the nature of the procedures had been explained fully.
. The informed consent of all human subjects who participated in this investigation was obtained after the nature of the procedures had been explained fully.
Author Contributions
Rahma Mungia and Alexander Testa: Conceptualization, Methodology, Formal analysis, Writing—Original draft.
Daphne Hernandez, Kayla Garcia, Joana Cunha-Cruz, and Gregg Gilbert: Writing—Reviewing and editing.
Data Availability Statement
The data supporting this study’s findings are available from the first author on request.