
Abstract
Background:
This study examines disaster preparedness and response in Federally Qualified Health Centers (FQHCs), which serve vulnerable populations, including individuals with non-communicable diseases (NCDs). Hurricanes Irma and Maria revealed gaps in chronic disease management, contributing to significant mortality. Climate change will likely exacerbate these challenges, necessitating a deeper understanding of preparedness factors.
Methods:
Using the Exploration, Preparation, Implementation, Sustainment (EPIS) framework, we conducted a qualitative study of 2 FQHCs in Puerto Rico and the U.S. Virgin Islands, analyzing inner (leadership, organizational culture, and staff dynamics) and outer (funding, networks, and policies) contextual factors. Twenty-four semi-structured interviews were analyzed thematically utilizing the EPIS framework.
Results:
Interviews with 24 staff members highlighted strong leadership valuing both employees and patients, prior disaster experience, and a culture of continuous improvement as essential for preparedness. Personal support systems improved staff engagement, while external collaborations with relief organizations enhanced response efforts. Flexible policies allowing access to medication and healthcare services beyond insurance coverage were critical for NCD patients during disasters.
Conclusion:
The EPIS framework successfully contextualized chronic disease management in extreme weather events, identifying strategies to mitigate climate-related health disparities. Strengthening inter-organizational networks and policy adaptability can enhance FQHC resilience, ensuring continued care for at-risk populations during disasters.
Keywords
Background
At least 30% of the mortality after Hurricane Maria can be attributed to poorly managed non-communicable diseases (NCDs). 1 With the advent of climate change, we will see an increasing frequency and intensity of extreme weather events. 2 These disasters are not experienced in the same way by all persons. In fact, persons living with NCDs are among the most vulnerable. Often, the same populations with a higher burden of NCDs and poorly controlled NCDs at baseline experience the greatest devastation from climate-induced disasters. This combination leads to the realization that climate change will worsen existing NCD disparities.3,4
The Caribbean is an example of this, suffering the highest premature mortality from NCDs and significant levels of exposure to climate-induced disasters. 5 The US territories of Puerto Rico (PR) and the US Virgin Islands (USVI) exemplify this, given their climate vulnerability, weaker health care system infrastructure, worse hospitalization outcomes, and higher burden of various NCDs. 6 This “double burden” of higher NCD rates and climate-related severe weather events exacerbating NCDs will worsen territorial NCD health disparities unless action is taken.
We partnered with federally qualified health centers (FQHCs) in PR and the USVI to develop strategies to reduce morbidity and mortality from poorly controlled NCDs after disasters. FQHCs are government-supported health centers that deliver care for underserved communities. Through government assistance, FQHCs can care for uninsured and underinsured (Medicaid) persons and offer care and services at a significantly subsidized rate. Their patient population represents the most vulnerable in these territories, given lower socio-economic status, limited insurance, high burden of NCDs, and limited means for evacuation.
In the project’s first phase, we used the Exploration, Preparation, Implementation, and Sustainment (EPIS) framework to explore the barriers and facilitators to NCD management in FQHCs to inform intervention selection and implementation during disasters. The EPIS framework is a widely used public health framework designed to help understand the implementation process in a systematic manner. 7 This framework was preferred over other frameworks as it emphasizes evidence-based practices (EBPs), has a clear progression for guiding implementation efforts, and is adaptable to various systems and populations. 7 EPIS does have similarities with other widely used frameworks such as the Consolidated Framework for Implementation Research (CFIR) in the contextual domains of inner context, outer context, and innovation or EBP 8 ; however, unique to EPIS is the focus of those factors to the public health service setting, its review of those factors across all 4 domains of implementation (exploration, preparation, implementation, and sustainment) and its focus on the interconnectedness of the contextual domains through the bridging factors. This made EPIS an ideal choice for this project.
Methods
EPIS Framework
The EPIS framework was selected because it specifically guides the implementation of evidence-based programs in publicly funded settings. 7 It identifies the key inner and outer setting contextual factors important to consider during all phases of implementing EBPs in an organization. EPIS also bridges factors between the organization, community, and academic partners.
Study Design and Setting
The larger study used a convergent mixed-methods research study design to identify strategies to address the needs of persons living with NCDs in the setting of disasters. 9 The NCDs included high blood pressure, diabetes, high cholesterol, mental health disorders (depression and anxiety), cardiovascular disorders, respiratory disorders, rheumatoid arthritis, pre-diabetes, kidney disease, liver disease, HIV/AIDS, cancer, systemic lupus erythematosus, and epilepsy. This study took place in the US territories of the USVI and PR between 2021 and 2022. Study sites included FQHCs in St. Thomas and PR. This study focuses on the results of qualitative 1-time in-depth interviews. The Emory University Institutional Review Board approved this study protocol.
Provider Recruitment
We invited providers, staff, and administrators at the study sites to participate. The study objective and methods were introduced at monthly staff meetings, and a QR code delivered the survey in English and Spanish to all eligible participants. All FQHC employees working at the FQHC during the 2017 hurricanes (Irma and Maria) were eligible. Within the survey for the parent study, participants indicated their willingness to participate in a qualitative, in-depth interview in person or via a video-conferencing platform. Participants signed informed consent for the parent study. To ensure confidentiality of participants, demographics were limited, and there was de-identification of specific role titles. To ensure the representativeness of interviewees, individuals were purposively recruited to ensure diversity in role, seniority, and years at the FQHC. Of the 150 total survey participants, 40 agreed to be contacted for a 1-time follow-up interview. Repeat interviews and participant checking were not included in this study. We interviewed 24 participants from 2 unique clinics (one on each island). No participants refused to participate or dropped out. Interviews were approximately 30 to 69 minutes long and took place in a private room where only the participant and the researcher were present. Interviews were audio recorded only; field notes were made during the interviews and were refined post-interview. Transcripts were not returned to participants for comments or corrections. Participants received a $25 gift card upon completion.
Interview Guide Development
The interview guide was developed independently of the EPIS framework, using open-ended questions to capture providers’ experience with NCDs during recent disasters. The guide was reviewed and refined through stakeholder and community advisory board input, then piloted with staff members at the FQHCs. Interview guides were developed to best fit this target population and research study.
Research Team Experience, Training, and Characteristics
The person conducting the interview (SP) self-identified as male, lived in the USVI for 2 years, and was a Master’s in Public Health student at [institution redacted]. He had extensive experience in qualitative research, including conducting interviews and qualitative analysis. The interviewer did not have previous relationships with the interviewees and was trained by SH in conducting interviews on how to minimize interviewer bias. SH and MW supported data analysis. MW and SH have not lived in the USVI but have worked with partners there for over 6 years. They both have extensive experience in qualitative research methods.
Qualitative Data Analysis
Interviews were recorded and transcribed verbatim. Transcripts were reviewed for accuracy and de-identified. Thematic content analysis was used for initial inductive coding. Two team members did line-by-line coding for at least 40% of transcripts. A third-party resolved discrepancies, and a final codebook was developed. All transcripts were re-coded with the final codebook using Dedoose software. Thematic saturation was achieved by analyzing the completed interviews. Emergent themes were derived from the data. Emergent themes were mapped to EPIS domains. Guideline recommendations were followed as shown in the Consolidated Criteria for Reporting Qualitative Studies (COREQ) checklist (Supplemental Appendix 1).
EPIS domains were separated into those that included factors that should be leveraged in future disaster preparedness and response, and those that presented challenges that need to be overcome in future interventions. The challenges were discussed with leadership within each of the FQHCs to determine which challenges could be addressed by the organization and the community leaders they work with, while others would require interventions at a more extensive system or policy level.
Results
Twenty-four interviews were conducted with FQHC staff, administrators, and healthcare providers, with healthcare providers making up half of the sample (Table 1).
Interviews with Providers and Characteristics.

Emergent themes that further our understanding of NCD management in disasters are mapped to the outer context, inner context, and bridging domains of EPIS (Table 2). Within the outer context, themes highlighted inter-organizational factors, the service environments, and patient characteristics. Within the Inner context domain, organizational and individual employee characteristics emerged as important factors. Lastly, the relationship between the community and FQHC emerged as an essential bridging factor.
Emergent Themes Organized by EPIS Domain.
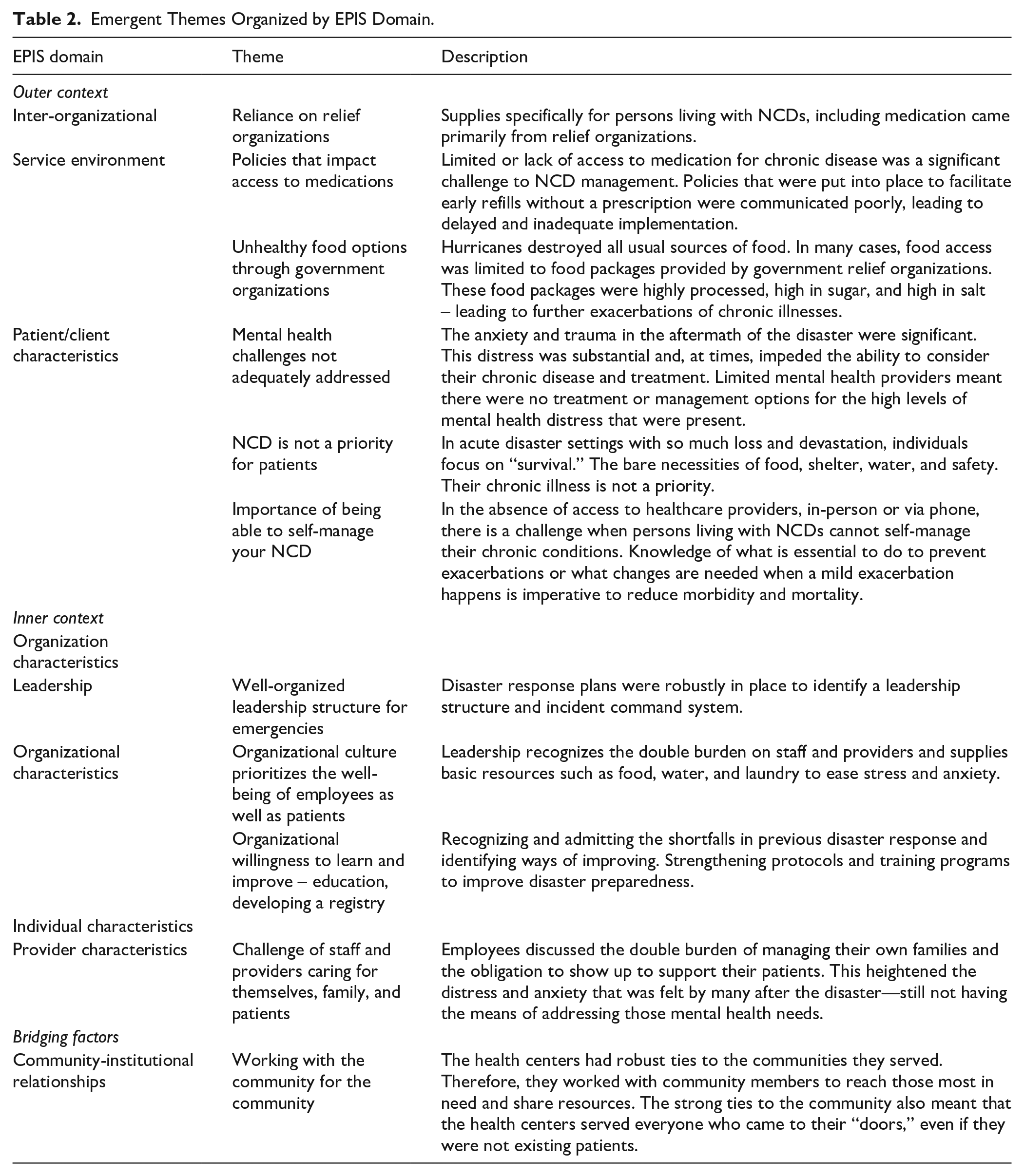
Outer Context
The outer context domain speaks to the critical actors outside the implementing organization. This includes relationships with other organizations, service/policy sectors, and the persons the implementing organization serves. The outer context played a prominent role in the challenges faced when managing NCDs during recent disasters. This included the inter-organizational and service environments and patient/client characteristics. FQHCs uniformly reported on the vital role of relief organizations in providing critical resources and services for everyone, particularly addressing the needs of persons living with NCDs through the provision of NCD-related medication. One staff member reported on how critical relationships with NGOs were in ensuring access to medications: “I think that’s probably about the only thing that we have under control is medications that we can get out for people, um, because we do have this relationship with Americares and Direct Relief, so that’s about the only thing that I think is-is pretty well handled.” Similarly, in Puerto Rico, a staff member commented on the role of these organizations in ensuring access to insulin: “So we were–we had to work with, uh, humanitarian organizations like [-] to be able to acquire insulin to distribute to the centers so that they could share it with, right, the patients use it.” (PR Staff)
At the same time, there were mixed views on the role of government-related services in supporting persons living with NCDs. Policies supporting medication access during a disaster were implemented late and inadequately disseminated, making it difficult for those who lost their medication to refill it. The lack of access to medication had direct health consequences, as 1 USVI Staff member stated: “I can’t think of any like one person, but just generally, um, the blood pressures were pretty out of control, um, a-as were the blood sugars. ‘Cause like I said, people did not have access to their medications’.” (USVI Staff). Similar challenges in accessing medications due to delays in policy implementation and communicating those policies were seen in Puerto Rico, 1 staff member stated, “Well, I would tell you that things happened little by little, that is, this access to medications was not the same speed . . . Then there were communication problems, eh, eh, um . . . that is, difficulties in notifying changes and, for example, eh, eh, the openness that there was to access to medications, right?” (PR Staff)
Government agencies providing food and nutrition services did not seem to consider the needs of persons living with NCDs, as food packages contained high salt and high sugar-containing options, potentially exacerbating most NCDs. One USVI staff member clearly outlined the unhealthy food options available to persons living with NCDs, “ . . . Um, they didn’t have access to good foods or healthy foods. Um, even those patients who typically don’t eat all that great to begin with, it was worsened by this because what they would get in those pre-formed things was just, you know, all this processed, sodium-packed food, M&Ms and Butterfingers and Twix bars in their little bags. I’m like come on. Give ‘em a granola bar if you can d—I mean something other than M&Ms and Twix bars . . ..’ That’s the stuff that came in-in the little MREs (Meals, Ready-to-Eat), and so the government somehow was providing this” (USVI Staff). Staff in Puerto Rico similarly spoke to the challenge of accessing food for persons with chronic diseases, “And these diabetic people, what they need is more treatment but also meals on time, all this type of things, and they didn’t have that type of provisions, it was very hard to handle it . . . And I would tell you that there was no resource right there because there was no food, it was good, there was no gasoline.” (PR Staff)
Three important themes emerged within the patient domain, speaking to the characteristics of those served by the institution. Firstly, the vital role of mental health. Across all FQHCs, there was recognition that trauma from the disaster induces significant distress, anxiety, and depression, impeding self-care and impacting NCD management. One staff member in Puerto Rico emphasized the burden of mental health: “We can see many patients who come for mental health situations, but more than anything, eh, we talk about mental health, the management of emotions, how to work with depression, anxiety . . .” (PR Staff 2) Interviewees recognized that this included the exacerbation of underlying and existing mental health disorders as well as new-onset problems. In both cases, mental health challenges were exacerbated by the lack of mental health providers. Basic mental health support fell on the staff and providers who learned to listen when needed, as 1 staff member in the USVI stated, “Um, like I said, they were traumatized. They’re too stressed. And so just a lot of-of-of kind of redirecting. Let’s see how we can still take care of you. How can we get you in to see someone? Um, we have a-a psych on staff, so we’re trying to get that sort of arranged for the people who really, really needed it. Um, but really just be an ear at that point. Um, no form—no medication, no formal counseling, but just someone to listen, someone to-to be I’m there with you type of things. Um, come back if you need to talk to us type of thing, um, just to kinda get them through the day.” (USVI Staff)
Secondly, providers recognized the importance of patient knowledge of disease self-management when access to healthcare providers was limited. The basic principles of NCD self-management are critical so that individuals can manage their chronic conditions when access to healthcare providers is disrupted. One USVI staff member stated this need clearly, “We need take care of our community by arming our patients with the knowledge and empowering them and teaching them, um, to take care of themselves and prepare themselves for a disaster, so that afterwards we’re just giving them a little bit of support and we’re not trying to pick up all of the pieces of all the damage that’s been happening, uh, post—” (USVI Staff)
Lastly, staff and providers reflected that people are not thinking about NCD management during a crisis. They are more likely to focus on immediate basic needs (housing, food, and water), placing their NCD management on the back burner. One staff member in Puerto Rico stated, “Well, they were concentrating on the immediacy of their housing, of food, of-of-of eh, situations, right? pressing for your immediate environment and why do I say that?” (PR Staff). There was limited awareness that continued management of one’s NCD is just as critical as basic needs. One USVI staff member emphasized this and the need to educate patients on the importance of addressing their NCDs in the immediate aftermath: “When people are going through, their whole mindset and their perception changes because, now, they’re in survival mode. And survival mode does not always entail, for them, taking my medication. Survival mode is havin’ water, bein’ able to take a bath, be able to put on some clean clothes, bein’ able to put some food in my mouth. But they’re not necessarily thinkin’ on the health. So finding ways to make them understand that taking medication and maintaining health is important during these hard times is one of the areas that I think that we need to consistently work on.” (USVI Staff)
Inner Context
The inner context domain of EPIS refers to the factors related to the organization and the organization’s workers. Both leadership and organizational characteristics were critical for the FQHCs to act and support persons living with NCDs. Even in the absence of formal disaster response plans, all FQHCs had a clear leadership structure that coordinated the efforts of staff and providers after the disaster. This coordinated effort was critical for service provision to be reestablished. In Puerto Rico, staff spoke about the incident command systems that were clearly instituted with specific protocols to follow to guide emergency responses: “Well look, the-the-the Emergency Management or Response Manual is-is developed by the of-the Occupational Safety officer. And basically we use a model of the Incident Command System, okay, which is a, um, universal, eh, model for emergency response. There is already an established protocol and they have, um, a flow chart of who are the people, um, who are going to be responding and what is the responsibility of each of them, right, um, yes. It’s basically how it works.” (PR staff) In the USVI, staff spoke to the importance given by leadership to contacting staff and making sure they and their families were okay: “Uh, my role here at the center was to ensure that the staff was okay. We make sure we-we contacted. We tried to contact everyone to make sure that all the pa—their families were okay. And so after we assessed that they were okay, then we would look at what our needs were in the center and for our patients.” (USVI staff) This was emphasized by another USVI staff member, “this behavioral health team, you have our contacts. We know how to reach out to each other. There was . . . somebody earlier this morning who said, ‘You know, the first thing we do is we tend to each other and call each other and see who’s okay and who’s not and who needs help.’” (USVI staff)
Organizational characteristics were critical to the effective implementation of ad hoc plans that saved lives. Leadership recognized the importance of the well-being of its staff/providers to better serve their patient population by addressing food, laundry, and water needs, and providing work hour flexibility. One USVI staff member spoke about how leadership prioritized staff, “Mr. X always says staff first—staff safety first, which is-which is great. He wants us to serve the community, but he wants to make sure that we’re doing it safely. So he’s made us a priority, which makes a difference.” (USVI Staff) In Puerto Rico, staff also commented on how their needs were being prioritized by leadership: “ . . . for example, there was a program providing lunch and breakfast for all employees. A, daycare was established for employees who had children so they could come into work. They brought, right I am giving an example, they brought washers, four washers so that employees could wash their clothes. And uh, there was special financial assistance for people who really had losses, right. For the employees who lost their homes, they had lost lots of things of value.” (PR staff) As the interview went on to discuss needs specific to NCDs, staff also highlighted the reality that many of them also live with chronic conditions that were also addressed as part of the response, “Yes and with the employees. I understand that-that it can be done as an organization of the employees of the organization by identifying how many of them suffer from chronic conditions and how we can provide, uh, service or space so that they, right, use that service as well.” (PR Staff)
Secondly, the organizations were, and continue to be, willing and eager to learn from prior experiences to improve upon their disaster preparedness and response. This attitude helped them adapt during the last disaster and provide necessary services. Today, they are better prepared from the lessons they learned. As 1 USVI Staff member stated, “ . . . because of experience, knowledge increase. Um, and then actually going through the disaster, you see where the loopholes are . . . and what needs to be improved. Um, hopefully not for the next time, but we have to say that because we know [laughter] disasters are not going anywhere.” (USVI Staff)
Individual characteristics of the staff, providers, and administrators are critical in understanding how the needs of patients with NCDs were or can be addressed in a disaster. One key theme that emerged was the double burden on providers who managed their distress and loss, and that of their families, while feeling the need to still show up to work to take care of their patients. One staff member in Puerto Rico put it bluntly as a struggle, “So, there is a struggle between I have to recover, I have to continue working, we have to make arrangements . . . ” (PR Staff) In the USVI, a staff member similarly spoke of the importance of having those at home being safe and cared for in order to be able to provide for the patients, “Because okay means that you are eating well; you got some rest; and, um, at home is as stable as possible. Because to come to work and function and knowing at home is not okay, it defeats the-the-the-the purpose of you being there and giving as much as you can give. Um once you are in that position, then you can think better; you could respond better; your attitude is better because things change in a disaster. Um, so I-I think, um, taking care of you emotionally and physically before you’re coming. That’s why after disasters we have debriefing, and there are people at the top because it’s-it’s so important so that you could function in a job.” (USVI Staff)
Bridging Factors
This domain reflects the interrelated nature of the inner and outer context. One theme emerged that embodied the critical interrelationship between the FQHCs and the communities they served. Across all FQHCs, providers described the importance of working with the community for the community. Longstanding relationships through community outreach, community advisory boards, and community-centered events led to bidirectional exchanges built on trust. This meant the FQHC was the first place that patients turned to for assistance. Similarly, FQHCs turned to community groups to reach vulnerable patients who needed care. The devotion and dedication to the community were exemplified in this quote from the USVI Staff: “ . . . then we were able to just give them the medication. Um, we would write it up, you know, put on a little, um, little pill bottle, then put the name on there, put the medication on there along with the instructions. The patient would sign it. Um, it didn’t matter who it was. We just wanted to treat the community.” (USVI Staff) In Puerto Rico, a staff member explained the special relationship they have with 1 community-based organization that facilitated their access to those most in need, “-and since that same day we began to make contact with the different community groups with whom we have this . . . a close relationship and I would tell you that particularly with the ENLACE project of Caño Martín Peña and the, the G8 group . . . Which are the eight communities surrounding Caño Martín Peña where, well, I recognize that they have a eh, that is, for me, those people are wonderful because even with all the limitations, shortcomings and difficulties in their surroundings and their environment . . . They are very organized, very structured.” (PR Staff)
Following the analysis of the emergent themes, we divided them into factors we could leverage and factors that were challenges needing to be addressed, highlighted in Table 3.
EPIS Factors to Leverage Versus Challenges to Address.

Of the EPIS factors that are challenges, FQHC leadership indicated that these could be addressed through interventions at the FQHC in collaboration with the community. These included inner context factors (individual characteristics), variable comfort and confidence in individual preparedness, and the double burden on providers during disasters. They also included outer context factors (patient/client characteristics) – the mental health challenges of patients that were inadequately addressed, and the need to raise awareness of the importance of managing NCDs in disasters.
FQHC leadership sought to leverage their strengths (well-organized leadership structure, prioritization of the well-being of staff and patients, and a strong relationship with the community) to identify EBPs to address the challenges. These included virtual and hands-on preparedness training, training of community members and staff/providers in psychological first aid, and distributing culturally and linguistically tailored educational material on NCDs in disasters through multiple modalities in collaboration with the community (pamphlets, social media, etc.).
Discussion
This paper used the EPIS framework to organize the barriers and facilitators to managing NCDs in climate-induced disasters as inner context, outer context, and bridging factors. In this exploratory phase, we analyzed in-depth interviews using an inductive approach and examined how emergent themes mapped onto EPIS domains. This provided a structured approach to discuss the challenges of managing NCDs in disasters and allowed the team to identify challenges that could be addressed through interventions within the FQHC and community by leveraging organizational characteristics and strong community-health center relationships.
This work confirms the complexity of NCD management in the setting of disasters as multi-level and multi-factorial. Prior studies examined the challenges faced by persons living with NCDs in disasters in the US territories, the US mainland, and other parts of the world.1,3,10 These studies elucidated common challenges, including access to medication, healthcare, and mental health services, and the fundamental life necessities of food, water, and electricity.4,11 To our knowledge, this is the first study to take a systematic look at the problem of NCD management in disasters through the lens of a healthcare facility. In so doing, we can inform an approach to overcome these challenges within the control and reach of the FQHCs and their communities. Using the EPIS framework allowed the team to differentiate outer context factors that would need a higher level of governmental engagement and policy change to support NCD management in disasters. While still important, these factors are not in the immediate control of the FQHCs and their communities. Instead, the team focused on what could be changed quickly through collaboration with the community. We also identified inner context factors that were facilitators for NCD management during prior disasters and should be leveraged in future endeavors to address the problem. This provides a robust example of how organizations can use the EPIS framework in study exploratory phases to address complex problems.
This work highlights the critical role of the community and its relationship with the healthcare organization serving it. While this can be labeled as a bridging factor within EPIS, its importance in the framework is undermined. For public-serving institutions like FQHCs, the relationship with the community is vital to gaining the necessary trust and fulfilling their obligations to the community. In such contexts, it would be helpful if the bridging factor could specifically call out the relationship between the organization and the community (not just community-academic partnerships as it stands now) and factors influencing the relationship (community outreach, engagement of community leaders, and historical outreach efforts).
These results are important in informing future work to implement strategies to reduce the impact of extreme weather events on morbidity and mortality of persons living with NCDs. In addition, in reviewing the results of this study, the following are specific policy recommendations that could improve health outcomes after a disaster:
Leverage the special relationship between FQHCs and the communities they serve. Disaster preparedness and response initiatives must reach the most vulnerable (elderly, bed-bound, and on chronic disease medication), which can be done through the trust and outreach that FQHCs have with the communities they serve. Disaster management agencies must work closely with FQHCs to make sure the needs of their communities are met.
Facilitate access to critical chronic disease medication in a disaster context through early planning and effective communication. Reduce reliance on NGOs and ad hoc groups for access to medication. Early communication of rules and regulations regarding early refills or alternative medication access should be conducted through multiple media approaches before the disaster.
Actively and proactively address mental health needs for staff, providers, and patients in the setting of a disaster. Training diverse groups of individuals on mental health and psychosocial support packages is critical, enabling community members, health providers, and other professionals to deliver this essential service in disaster settings.
Integrate NCD management into all sectors engaged in disaster preparedness and response. Disaster response teams responsible for nutrition, transportation, communication, and health must recognize and address the unique needs of persons living with NCDs in the setting of a disaster.
Support research to understand and optimize multi-level strategies to reduce the impact of disasters on NCDs. Increased support for Implementation Science studies is needed to further our understanding of which strategies are most effective in specific contexts, thereby reducing the impact of extreme weather events on health.
There are a few limitations to this study that should be noted. Firstly, this work focuses on the US territories of the USVI and PR, as well as within FQHCs and the communities they serve. Therefore, it may not be generalizable to other settings or organizations. However, the approach of using the EPIS framework to address a complex problem from the perspective of an organization in the preparation phase of the implementation process can be applied to multiple other contexts. Additionally, it is notable that the emergent themes were similar across the 2 contexts of the USVI and Puerto Rico, with no identified discrepancies. This suggests the potential generalizability of the themes and recommendations provided. Secondly, there is the possibility that staff and providers did not feel comfortable disclosing negative organizational characteristics that may have influenced disaster response. Lastly, this study did not employ participant checking, which could impact the validation of the study findings.
Conclusion
Despite these limitations, this work contributes significantly to understanding barriers and facilitators to NCD management in disasters from the perspective of publicly funded health centers. This work also furthers our understanding of the application of EPIS in the context of a complex problem of disaster response. It also calls out the important role of the organization and community relationship and provides specific policy-level recommendations to reduce the impact of extreme weather events on persons living with NCDs. Future work will identify strategies that can be implemented by FQHCs and the communities they serve, and will evaluate their effectiveness in reducing morbidity and mortality from NCDs during disasters in the U.S. territories.
Supplemental Material
sj-pdf-1-jpc-10.1177_21501319251371090 – Supplemental material for Lessons From Federally Qualified Health Centers in the US Territories on Managing Non-Communicable Diseases in the Setting of Disasters: A Qualitative Study Using the Exploration, Preparation, Implementation, Sustainment (EPIS) Framework
Supplemental material, sj-pdf-1-jpc-10.1177_21501319251371090 for Lessons From Federally Qualified Health Centers in the US Territories on Managing Non-Communicable Diseases in the Setting of Disasters: A Qualitative Study Using the Exploration, Preparation, Implementation, Sustainment (EPIS) Framework by Saria Hassan, Michelle Teresa Wiciak, Karla Escobar, Tess Richards, Hector Villanueva, Dabney P. Evans, Marcella Nunez-Smith and Adithya Cattamanchi in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We would like to thank the administration, staff, and providers of the 2 FQHCs for their time and dedication to this work
ORCID iDs
Ethical Considerations
This study protocol was approved by the Emory University Institutional Review Board.
Consent to Participate
Informed verbal consent was obtained from all participants prior to participating in the in-depth interviews.
Consent for Publication
Not applicable.
Author Contributions
SH and MNS conceptualized the study. KE, MG, HV, JR, and TR collected data from participants. KE, MG, SH, and MW conducted data cleaning and analysis. KE, MW, and SH wrote the first draft of the manuscript. AC provided oversight of the use of the EPIS framework. DE provided oversight on disaster preparedness concepts. All authors reviewed the manuscript and provided considerable feedback and edits.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: SH is funded by NIH/NHLBI K23HL152368.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.