
Abstract
Background:
The Links to Care Community Grants Project was developed to improve breast cancer outcomes by increasing access to appropriate follow-up care, improving processes for care transitions, and enhancing care coordination between community health centers (CHCs) and hospital partners.
Methods:
This 24-month multi-pronged project encompasses quality improvement (QI) coaching, technical assistance support, and evaluation. QI coaching follows the Model for Improvement to test and adapt to changes. Local and centralized technical assistance supports the individual needs of the health system. A data collection tool was developed to evaluate implemented interventions and assess changes in breast cancer screening and diagnostic testing completion rates, time between care transitions, and process improvements made throughout the project period.
Results:
Seven CHCs comprised of 27 clinic sites with 26 255 patients eligible for breast cancer screening agreed to participate. Baseline findings demonstrate an average screening rate of 51.1%.
Conclusion:
The Links to Care Community Grants Project will evaluate the effectiveness of implemented patient, provider, and/or system-level interventions and care coordination process improvements on reducing delays along the breast cancer care continuum.
Keywords
Introduction
About half (52.4%) of women aged 50 to 74 served by Health Resources and Services Administration (HRSA) funded health centers received a mammogram in 2023. 1 Suboptimal breast cancer screening rates contribute to morbidity and mortality, which remain disproportionately higher in Black women compared to White women, regardless of age. 2 Screening challenges at the system, provider, and patient level are well documented,3 -6 including provider orders placed at one clinical encounter while scheduling and mammogram completion occur at another time and location. 7 Additionally, patients experience delays along the cancer continuum due to a lack of transportation, paid time off, or childcare 6 ; challenges with multi-appointment scheduling with specialty oncology or physical rehabilitation; or in the communication of results.8 -10 While most research to date has focused on increasing screening rates,11 -14 less work has centered on improving timely follow-up after abnormal screenings, particularly for people of color and socioeconomically under-resourced groups.
Several studies have demonstrated the effectiveness of individual and multicomponent interventions in increasing breast cancer screenings.15 -17 These studies report success with increasing community access, community demand, or provider delivery. Similarly, a comprehensive literature review has shown interventions at the patient level have the greatest impact on increasing follow-up after abnormal findings. 18 However, research has traditionally focused on the use of multicomponent interventions to increase screening rates rather than follow-up care.
To address the literature gaps in methods to advance follow-up care beyond screening, the American Cancer Society spearheaded the breast cancer Links to Care Community Grants Project (LTC) adapted from the successful Links to Care Pilot Project previously focused on colorectal cancer screening. 19 The current project is designed to address challenges along the breast cancer care continuum between community health centers (CHC) and hospitals, including timely follow-up after an abnormal screening mammogram by increasing access to screenings, diagnostic care, and treatment within underserved populations served by CHCs.20 -22 The purpose of this paper is to describe the development, implementation, and anticipated impact of the LTC Community Grants Project. We aim to 1) improve timely access to diagnostic testing and follow-up care through quality improvement process changes and interventions; and 2) strengthen referral relationships and care coordination between CHCs and hospitals in target communities, as called upon by previous literature,13,22 thus resulting in fewer patients experiencing delays along the breast cancer care continuum.
Methods
Setting and Timeline
The American Cancer Society (ACS) and the National Football League (NFL) have expanded a 15-year relationship to include the breast cancer LTC Community Grants Project. 23 Invited for participation by ACS associate directors, 6 hospitals worked with 1 or more CHCs to improve access to follow-up care for patients with abnormal screening mammograms across the continental United States (U.S.). Each hospital is affiliated with a NFL team and must be a pre-existing referral site for their CHC partner. This 24-month (January 2023 to December 2024) multi-pronged quality intervention (QI) quasi-experimental pre-post design with multiple data collection points project includes a 6-month capacity building phase (months 1-6), an initial intervention implementation phase (months 7-12), a revised intervention implementation phase (months 13-24), and 3 periods of data collection that encompass the previous 12 months before project start, project year 1, and project year 2 (Table 1). This project was reviewed by the Institutional Review Board (IRB) at the Morehouse School of Medicine and was deemed to not be human subjects research (eIRB #2124431-2). As such, patient consent was waived by the IRB. Participation, data use, privacy and confidentiality agreements have been established between ACS and each health system.
Links to Care Community Grants Project Timeline.
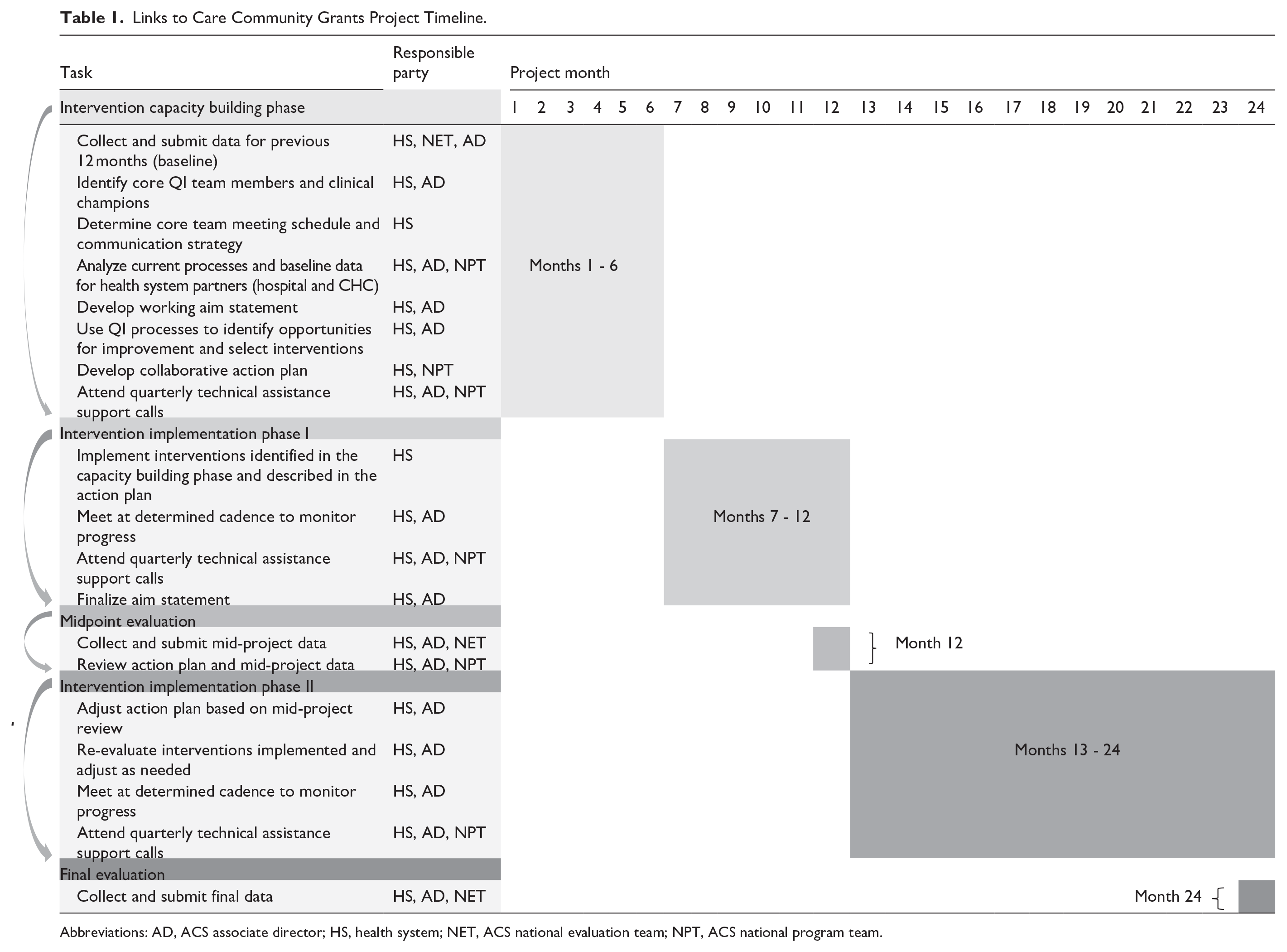

Abbreviations: AD, ACS associate director; HS, health system; NET, ACS national evaluation team; NPT, ACS national program team.
Participants
Adults served by a participating CHC with at least one medical visit in the 12 months preceding data collection, who are eligible for breast cancer screening, as recommended by the electronic clinical quality measure are the target population.12,24 For the purposes of this paper, CHCs include HRSA-funded health centers (n = 6) and non-HRSA funded health centers (n = 1). CHC participation is limited to those that:
Provide primary care regardless of financial status,
Provide care to marginalized populations with limited access to care,
Can report cancer screening rate data from a primary care patient population,
Can report, or demonstrate tracking efforts, on referrals to: Initial screening, Diagnostic testing,
Can report, or demonstrate tracking efforts, on length of time between: Abnormal screening and first diagnostic test, Cancer diagnosis and first visit with an oncology specialist, Cancer diagnosis and treatment initiation, and
Provide access to screening (may include referrals) for eligible patients for breast cancer,
Have a baseline breast cancer screening rate of <70%.
Participating hospitals will partner with CHCs which they are a referral site and provide follow-up care, including diagnostic care. Health systems that meet these criteria will receive grants supported by the NFL for the two-year project to aid personnel and project operational costs.
Partnership Structure
The ACS national program (NPT) and evaluation teams (NET), ACS associate directors (AD), and health system partners have a multi-layered partnership (Figure 1). The NPT provides QI training and centralized technical assistance (TA) to ADs and health systems. They will meet quarterly with all health systems for peer-to-peer learning and ADs, separately, both in a large virtual format for the projects’ duration to discuss promising practices, successes, and challenges. The NET provides data and evaluation expertise for the collection, management, and analysis of project data. They are available to assist and answer data-related questions health systems encounter throughout the project. ADs assist health systems with analyzing current QI processes, improvement planning, local TA, offer strategies following the Model for Improvement, practice QI coaching with the NPT, and guide collaborative action planning activities.25,26 ADs will meet monthly with each health system either in-person or virtually for the projects’ duration to review action plan progress, completed tasks to date, challenges, and advancement toward outcomes.

Links to care community grants project partnership structure.
QI Process
As part of the QI process, action plans are to be created between collaborating health system partners before project kickoff. Collaborative action planning allows partners to discuss gaps and barriers, determine QI strategy, develop solutions, streamline processes, and discuss interventions to implement or improve as patients move through the care continuum between institutions (Figure 2). QI strategies may include plan-do-study-act (PDSA) cycle designed to test and refine process changes to improve follow-up care, process mapping to integrate new patients from the CHC efficiently, and root cause analysis to explore the causes of gaps and barriers affecting an increase in screening and follow up care. Additional steps include core team identification, aim statement creation, and determination of meeting and communication frequency. Core project team composition varies by health system partnership but typically includes an AD, QI lead, provider champion, nurse and/or medical assistant, information technology, office manager, and patient care coordinator. Health systems work alongside their ADs to implement interventions, evaluate current QI processes, develop workflows, and submit data to measure project impact.27,28
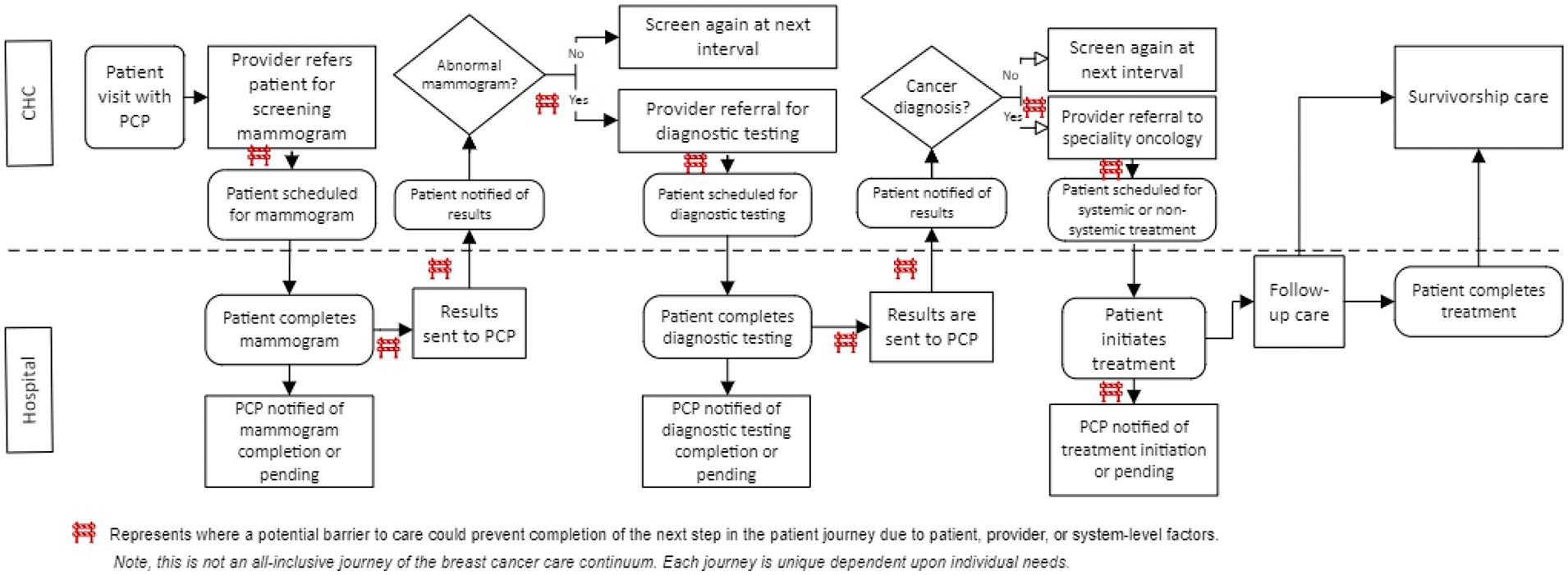
Example patient journey through the breast cancer care continuum.
Aim Statement
Aim statements help answer the first questions in the Model for Improvement “What are we trying to accomplish and how will we know if that change is an improvement?.” Each aim statement will follow the same format: target population, specific numeric goal, designated time between screening and follow-up, and the identified health system partner. Systems are to develop and evaluate their working aim statement during the first intervention implementation phase and submit the final aim statement during the midpoint evaluation. We anticipate health systems will strive to reduce barriers to care along the continuum and increase breast cancer screening completion rates by at least 10%.
Interventions
Health systems will select from a pre-determined list of 21 evidence-based or informed interventions shown to eliminate or minimize common barriers (Table S1 in Supplemental Material). The process for selection will vary by identified gaps and barriers between partnering health systems. Twelve interventions are evidence-based and supported by the literature: appointment reminders, 29 electronic health record enhancements,30 -32 implementation/improvement of patient navigation, 29 increased availability of financial support, 29 increased availability of screening and diagnostic services,29,33 increased availability of screening methods,29,34 increased availability of transportation services, 35 increased availability of translation services, 29 patient outreach and communication services, 29 provider/staff training, 29 service/care coordination across care transitions,29,36 and standardized pathways for continuum of care.37,38 The remaining interventions are evidence-informed based on expertise of the American Cancer Society. Interventions are provider (4), patient (2), or system-focused (19) and could represent more than one focus area; for example, patient outreach and communication improvements could represent either a provider or system-level focus. Health systems will be instructed to choose interventions that best suit their needs while reminded that multicomponent interventions lead to greater effects.14,15,39 We anticipate health systems will implement at least three interventions with most being system focused. Health system partners are given autonomy to implement similar or different interventions if the anticipated outcome aligns with partnership goals and follows the QI framework. We anticipate additional factors affecting selection of interventions may include limited resources, competing priorities, staffing, leadership buy-in, and capacity.39,40
Data Collection, Management, and Analysis
Health systems will use the Data and Reporting Tool (DART) to report aggregate patient demographics; number of participating clinic sites; breast cancer screening practices (ie, mammography option types, scheduling capacity, patient/provider communication, free or low-cost mammogram availability, assessment of barriers); electronic health record (EHR) software; breast cancer screening rate based on the electronic clinical quality measures described in CMS 125; completed screening and diagnostic testing; specialty/treatment referrals; time between continuum steps; and established processes for patient and provider follow-up for missed appointments. The objective measures on the DART were developed through key informant interviews, review of the evidence,29,41,42 and a staged review and pilot process including expert input. The DART uses open-ended, dichotomous, single/multiple choice selection, and matrix style questions.
Health systems will complete the DART at baseline (month 1), mid-project (month 12), and final (month 24). Baseline data will cover the calendar year prior to the intervention. Mid-project data will cover Year 1 of the project, specifically QI programming and intervention implementation. Final data will cover Year 2 of the project, specifically process improvement and project maintenance. Brief, ad hoc questionnaires will be distributed between DART collection periods for optional completion as common barriers arise. These brief surveys are open-ended, and the feedback is intended to inform TA needs. Study data will be collected and managed using REDCap electronic data capture tools hosted at the American Cancer Society.43,44
We will perform data quality checks to verify data integrity, including but not limited to missing data, instances where screening rate denominator exceeds numerator, improbable screening rates, improbable screening rate change between time points, instances where screening mammogram completion exceeds referrals, and improbable time between stages of the continuum. Analyses may include descriptives, parametric tests, and non-parametric tests as appropriate, while exploring region, demographics, and QI activities. Analyses will occur within Microsoft Excel (Version 2503) and IBM SPSS Statistics (Version 30). Health systems that are unable to correct data issues will be excluded from analyses. Open-ended questions and aim statements will be analyzed by deductive thematic analysis to determine similarities and differences between health system goals.
Outcome Measures
Table 2 provides an overview of numeric or time-based short- and long-term effectiveness outcomes, including operational definitions, data source(s), health system type reporting the outcomes, and project timing of data collection.
Effectiveness Outcomes for the Links to Care Community Grants Project.

Abbreviations: HS, health system; EHR, electronic health record; CHC, community health center.
The short-term effectiveness outcomes include: 1) number of eligible patients completing breast cancer screenings reported by health systems at 12 and 24 months after initial intervention implementation; and 2) the number of eligible patients completing diagnostic testing reported by health systems at 12 and 24 months after initial intervention implementation. It is anticipated these short-term outcome data will be reported by CHCs as they initiate mammogram referrals, track order completion, and refer for diagnostic testing. As Table 2 demonstrates, the implementation of patient, provider, or system-level interventions is anticipated to increase screening and diagnostic testing completion, as well as reduce time along the care continuum.
To determine the strength of relationships between hospitals and CHCs and reductions in care transition delays, the long-term outcomes are: 1) the number of days between an abnormal primary screening mammogram and diagnostic screening; 2) the number of days between a breast cancer diagnosis and systemic or non-systemic treatment initiation; 3) the number of days between a breast cancer diagnosis and a first visit with specialty oncology; and 4) decreased barriers to care for CHC patients. All long-term outcomes will be a cross-sectional measure through a 24-month lookback. It is anticipated long-term outcomes related to screening will shift from the CHC to the hospital as a patient transitions care to the hospital system. Contrarily, both types of health systems should remain able to report changes in barriers to care.
Baseline Results
Intervention Capacity Building Phase
At baseline, the project included 7 CHCs comprised of 27 clinic sites representing 195 741 total patients. Each health system partnership is comprised of at least 1 CHC and 1 hospital in 4 continental U.S. regions: Midwest (2), Southeast (2), Northwest (1), Northeast (1). With exception, the Southeast partnership is composed of 2 affiliated CHCs partnering with 1 local hospital. Participating CHCs reported 26 255 patients eligible for breast cancer screening with an average screening rate of 51.1%. Of the participating CHCs that reported aggregate patient population demographics at baseline, most patients self-identified as non-White (80.5%), predominately identifying as Black/African American (38.2%) and Hispanic/Latino (26.3%); 43.7% of patients are insured by Medicaid/CHIP; 6.5% Medicare; and 28.9% are uninsured. Table 3 provides further baseline characteristics.
Health System Partnership Baseline Characteristics.

Abbreviations: AA, African American; AIAN, American Indian/Alaksa Native; C, CHC; CHIP, Children’s Health Insurance Program; H, Hospital; HSP, Health System Partnership; NH, Native Hawaiian; nH, non-Hispanic; OPI, Other Pacific Islander; UN, Uninsured.
Total row percentage may not equal 100% due to rounding.
Patient population includes individuals of all ages served by sites participating in Links to Care; reported by health systems.
Eligible patients are defined as women who were aged 50 through 74 with at least 1 reportable medical visit at a CHC between 1/1/2022 and 12/31/2022.
Reflects CHC average.
Unreported by health system.
Discussion
This project will apply a similar framework as the original Links to Care project focused on colorectal cancer, which showed success utilizing the three-tiered partnership model and linking a CHC with specialty care (ie, hospitals). We strive to further develop these linkages between health systems for underserved populations while improving care transitions. While the original project focused on providing no cost screenings, we will focus on identifying and removing barriers to improve care across the continuum.
The current project revealed 3 main findings: 1) an average baseline screening rate of 51.1% for participating CHCs; 2) a large percentage of CHC patients identifying as Black/African American or Hispanic/Latino; and 3) a large percentage of patients covered by Medicaid/CHIP, Medicare, or uninsured. While the baseline screening rate is above the national average for federally qualified health centers, it remains below the U.S. general population national average and Healthy People 2030 target of 78.2 and 80.3%, respectively.12,45 The ethnic and racial minoritized groups and uninsured patients within our project are higher than 2023 HRSA metrics, 1 thus, representing the disparate needs of each community. A strong body of literature demonstrates racial, ethnic, and insurance disparities and the need to increase access to screening and follow-up care for these populations.2,5,6,12
Strengths and Limitations
Directly targeting disparate populations and the communities they reside in is vital to overcome the existing cancer health disparities. Additionally, this project is designed to focus on care transitions as patients move between their CHC and hospital. The collaboration between health systems is unique as it utilizes a community-based approach, focusing on the patient, rather than systems to improve care transitions and coordination. Our multi-tiered partnership focuses on relationships, communication, and allows constant interaction with health systems to address gaps, concerns, and the provision of evidence-based or informed solutions.
This QI project did not utilize randomization or a comparison group; thus, it is possible changes observed could be attributed to factors outside the project. However, the two-year longitudinal design allows for closer examination of changes over time. Second, all continental U.S. regions were not included, so results may not be generalizable to the West or Southwest. While this project created relationships between CHCs and hospitals that did not previously exist, external validity may be limited to similar health systems, NFL designated hospitals, or CHCs serving similar disparate populations. A small sample size may limit the ability to detect statistical significance.
Future Implications
The LTC Community Grants project strives to improve breast cancer outcomes by enhancing care coordination between CHC and hospital partners, including mammograms and diagnostic procedures through process improvements and interventions. Measurement of the short- and long-term outcomes adds to the literature by expanding upon the importance of CHC and hospital relationships, process improvements, and barrier reduction to ensure timely and equitable follow-up and care coordination.46 -48 Results from this project may serve as a novel method for reducing breast cancer morbidity and mortality and increasing access to necessary care following an abnormal screening.13,22
Conclusion
Utilizing a QI-based, process improvement protocol has the potential to mitigate existing disparities, improve care transitions to reduce delays between health systems, and provide accessible breast cancer health services for patients served by CHCs. Additionally, this project demonstrates the feasibility of evidence-based and informed interventions to close gaps during care transitions. Future research should focus on how population demographics, region, and clinic resources affect transitions along the breast cancer care continuum to better inform best practices for care coordination between health systems.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319251357987 – Supplemental material for A Collaborative Approach to Improving Breast Cancer Screening and Follow-Up Through Multicomponent Interventions and Process Improvements: The Links to Care Community Grants Project study protocol and baseline findings
Supplemental material, sj-docx-1-jpc-10.1177_21501319251357987 for A Collaborative Approach to Improving Breast Cancer Screening and Follow-Up Through Multicomponent Interventions and Process Improvements: The Links to Care Community Grants Project study protocol and baseline findings by Emily A. Prentice, Abby Moler, Amanda Sweeney, Karla Wysocki and Michelle Burcin in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The authors would like to recognize the ACS Associate Directors, participating community health centers, and participating hospitals for their time and dedication to this project. We thank Laura Makaroff, Teri L. Malo, and Shaylen Foley of the American Cancer Society for their time and ideas in support of this effort and manuscript preparation.
Ethical Considerations
The Institutional Review Board at the Morehouse School of Medicine determined this project was not human subjects research (eIRB #2124431-2).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The American Cancer Society Links to Care Community Grants Project is supported by the National Football League’s (NFL) Crucial Catch. NFL team affiliated hospitals were the designated partner hospital for all participating health CHCs. The NFL had no role in data collection, analysis, or interpretation; decision to publish; or writing of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets presented in this article are not readily available due to privacy concerns. Reasonable requests to access deidentified datasets or evaluation tools should be directed to
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.