
Abstract
Introduction
Development of clinical care pathways to reduce health care costs has become an international agenda. Specifically, pathways associated with the integration of behavioral health services in primary care settings have received particular attention. 1 This model, known as integrated care (IC), was generated in part as a response to the fact that 50% to 70% of individuals seen in a primary care setting suffer from a clinically relevant behavioral health problem. 2 By integrating behavioral health consultants (BHCs) in the primary care setting, patients are able to see both their primary care provider (PCP) and receive behavioral health intervention in the same location and at times, during the same visit. Perhaps more important, BHCs and PCPs can develop a collaborative treatment plan to address complex symptom presentations. This integration can increase quality of care and reduce stigma traditionally associated with behavioral health care. Furthermore, IC also has been shown to reduce overall medical costs by leveraging PCPs’ time and reducing the use of specialty and emergency care. 3
Although there has been a proliferation of guidelines regarding implementation of IC,4-6 data indicating the best way to achieve optimum integration are lacking. 1 The use of quality improvement (QI) initiatives by IC systems can aid in generating these sorely needed evidence-based answers. 7 QI is a philosophy and set of tools that systematically identify measurable and meaningful outcomes in an attempt to understand the processes that influences them. 8 Through this systematic evaluation, learning trials are performed in an attempt to continuously improve outcomes. These learning trials also help enhance the QI system of measurement because of the fact that they may generate hypotheses regarding possible systematic change.
An important BHCs metric in an IC program is their productivity. 7 Analysis of productivity and no-show rates, 2 factors that are interrelated, may help identify possible gaps in the IC program (eg, low productivity and low no-show rates may indicate that referrals from PCPs are not occurring effectively). This case study presents the use of a QI system to increase the productivity and reduce the patient no-show rate of behavioral health care providers, in order improve patient access to behavioral health services.
Setting
Community Health Alliance: Federally Qualified Health Centers in Northern Nevada
Community Health Alliance (CHA) was founded in 2012 to address the need of low-income families with inadequate access to health care, via a merger of 2 existing Northern Nevada health care systems: Health Access Washoe County (HAWC) and Saint Mary’s Mission Outreach. Since the merger, CHA has provided primary medical, behavioral, and dental care for both adult and pediatric populations at 4 distinct locations. In 2013, X served a total of approximately 26 300 patients. Of these patients, the majority identified as either Hispanic/Latino (49%) or Caucasian (41%). The overwhelming majority of patients that receive services at X live at or below 100% of the federal poverty line.
Integrated Care at Community Health Alliance
In August 2012, X began integration efforts by collaborating with the University of Nevada, Reno. This partnership resulted in the hiring of a 20 hours per week psychological extern (a doctoral student in Clinical Psychology at the University of Nevada), who was trained specifically in IC. During the initial months, clinical pathways and IC practices were created (eg, behavioral health screening of all patients) to support the extern’s role. This BHC role included brief psychological assessment, intervention (ie, 20-30 minute appointments), and patient consultation with PCPs. A second 20 hour per week psychological extern was hired to provide care at 2 additional X health centers in August 2013, which resulted in IC services at 3 of the 4 health centers operated by CHA.
Productivity and No-Show Rates Analyses at Community Health Alliance
Productivity and no-show rates are important metrics for PCPs at CHA. However, since the BHC externs are not eligible to bill insurance companies, administration did not initially analyze productivity and no-show rates reports. Therefore, it was uncertain how optimally BHCs time was being used.
When the topic of BHC productivity was initially addressed, both administrative and medical staff reported high satisfaction with the productivity and accessibility. However, both externs reported that they were under the optimal productivity goal of two patients per hour. This concern spurred the analysis of productivity and no-show data for both BHCs and implementation of QI initiatives.
Data Source
Behavioral health consultant productivity and no-show reports, assessed by the electronic health record, were generated for the period from August 2013 to May 2014. Potential areas for improvements were identified and changes to the IC system were implemented. Data were continually analyzed to determine if the intervention had met the objectives of increased productivity and decreased patient no-shows.
Results
In October 2013, concerns regarding productivity and patient no-shows were raised and a retrospective analysis was conducted between the months of August 2013 and October 2013 (Figures 1 and 2; Tables 1 and 2). The 2 BHC externs, across the 3 locations, had provided 248 individual services (extern 1 = 155). During that time, they both averaged a productivity rate of 0.85 patients per hour. Patient no-show rates during that time period for extern 1averaged at 30% and for extern 2 averaged at 19%. These data remained consistent for the months of November and December.
Total productivity.

Total no-show rates.
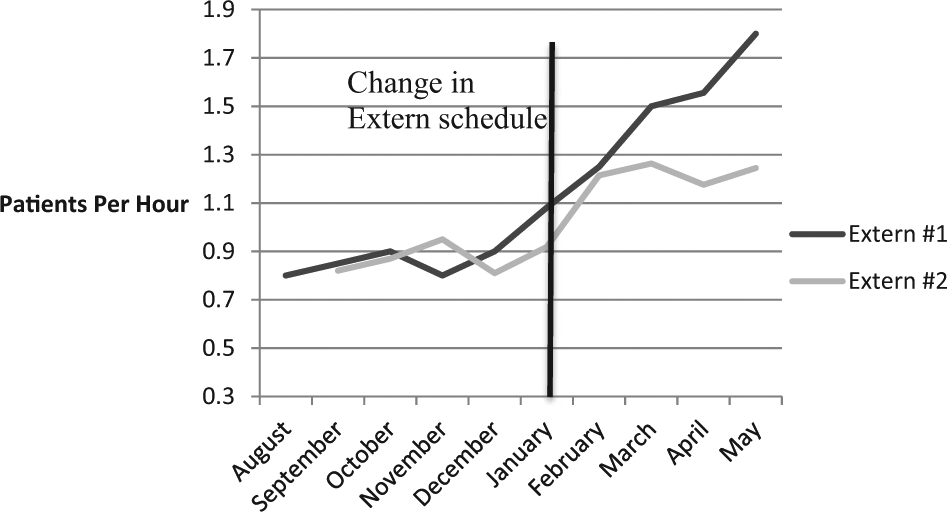
Psychology Extern Behavioral Health Consultant (BHC) Productivity August 2013 to May 2014.

Psychology Extern Behavioral Health Consultant No-Show Rates August 2013 to May 2014. a

Values are given as percentage.
In December 2013, a QI approach was taken to address the underutilization of the BHC externs. After deliberation regarding the process of care map (see Figure 3), it was decided by the IC team that the appointment blocks for patients would be scheduled for 20 minutes, instead of 30 minutes, starting in February 2014. By reducing appointment times by 10 minutes, it was hypothesized that patients would be provided with more options to schedule an appointment, given that the extern’s hours were limited. This change would also reduce the impact of no-shows on reaching the productivity of 2 patients per hour by allowing for maximum of 3 patients, instead of 2, to be seen. Finally, it was hypothesized that this change would allow for more appointment times to be available for “warm” hand-offs to occur, for patients to receive behavior health services immediately. Immediately after this scheduling change took place, productivity was affected for both BHC externs. The 2 BHC externs, across the 3 locations, had provided 635 individual services (extern 1 = 389). In comparison with baseline (0.85 patients per hour), extern 1 averaged a productivity rate of 1.52 patients per hour—t(7) = 6.62, P < .001)—with the last point of 1.8 patients per hour. Extern 2 average productivity rate was 1.22 patients per hour—t(6) = 9.87, P < .001.

Process map of behavioral health referral and appointment scheduling.
To further improve services, QI was also used to address, the discrepancy of no-show rates between the 2 externs was also addressed. It was hypothesized that the reminder calls that patients who were scheduled with BHC extern 2 were receiving made a significant impact on no-show rates. To address this, starting in February 2014, reminder calls were made for all patients at CHA who were receiving behavioral health services. This resulted in an end result of a 5% average decrease in no-show rates for extern #1—t(7) = 5.78, P < .001.
Discussion
Through the use of QI, CHA was able to improve the efficiency and access of its BHC externs. Analyzing productivity data for the BHC externs led to specific systematic change in care processes that were followed by statistically significant increases in total patients per hour and reduction in no-show rates. By engaging in this quality improvement process, 1 BHC extern yielded almost an 80% increase in productivity. Also, by placing reminder calls for extern 1, there was average 5% drop in the total of no-show rates.
Through the use of QI, other potential factors that may influence productivity and no-show rates are currently being addressed at CHA. For example, it is hypothesized that new medical providers may not effectively use or understand the referral process to BHCs and the importance of the “warm” hand-off. This in turn may impact productivity and no-show rates. As a result, CHA has begun an initiative to provide refresher training to all staff and providers in IC practice.
This case study provides preliminary evidence of the utility of QI in IC. Through the use of data gathered from the electronic health record, areas that were not initially a concern with administration and staff were identified. By collecting these data and using items, like the process map, areas that may have been influencing outcomes were identified and changed on a systematic level. These changes were followed with statistically significant improved outcomes across multiple providers in various settings. This provides some support that QI programs are an integral and important aspect of successful implementation of integrated care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.