
Abstract
Introduction/Objectives:
Primary care organizations increasingly face pressures to implement evidence-based practices that can support patient-centered goals. Foundational to these implementation efforts is how prepared the organization is to change. The purpose of this study was to examine whether different types of external linkages among 47 primary care practices participating in a statewide, community-academic partnership/cooperative focused on improving cardiovascular health outcomes were associated with greater change preparedness. Relatively little research has examined these linkages among smaller primary care practices in the U.S. and the extent to which they may support or hinder efforts to adopt innovative, evidence-based practices.
Methods:
The study adopted a non-randomized, pre-post design with primary care clinics as the unit of observation. Cross-sectional regression analysis of data collected via surveys administered in 2022 to 2023. Our dependent variables included 2 summated scales related to change readiness (change commitment and change efficacy) and 1 summated scale related to change process capacity, while controlling for differences in clinic characteristics and community characteristics.
Results:
Clinics that were part of a network (structural linkage) were associated with lower levels of change commitment (b = −1.36, P = .006) and change efficacy (b = −1.16, P = .021). The other 2 types of external linkages (informational and consumer/patient) were not significantly associated with either change commitment or change efficacy.
Conclusions:
Study clinics exhibited relatively high levels of change preparedness, providing a solid foundation for efforts to reduce cardiovascular risks in critical primary care settings. However, primary care clinics that were linked structurally were associated with lower levels of change preparedness. Primary care leaders and policy makers may want to consider the relationships between primary care clinics and other entities in their environment when developing and implementing programs to reduce cardiovascular disease risks in these settings.
Keywords
Introduction
Most organizations face an inherent tension between stability and change.1,2 Stability allows organizations to develop predictable and efficient work processes and outcomes. 1 Efforts to support such stability can be observed in organizational artifacts such as clearly delineated authority structures, formalized professional roles, and highly institutionalized organizational work routines.3,4 Change, on the other hand, enables organizations to adapt their strategic and operational priorities in response to dynamic political, regulatory, economic, and social conditions.5,6 In the U.S. health care system, the movement toward patient-centered value-based care represents 1 such shift in the external conditions for health care organizations, particularly health care providers (eg, hospitals, nursing homes, and primary care clinics).7,8 Health care provider organizations increasingly face pressures to implement evidence-based practices that can support these patient-centered, value-oriented goals. Foundational to any effort to implement evidence-based practices in health care provider organizations is how prepared the organization is to take on such change.9,10 Organizations that are more prepared to undertake change are more likely to overcome, even if only temporarily, some intentional efforts to preserve the status quo (eg, authority structures and overlearned routines). Hence, an important question is how to foster organizational preparedness to undertake change?
Our analysis draws upon the theoretical literature related to inter-organizational relationships11 -14 and organizational readiness for change 10 that proposes these relationships can provide organizations with important tangible and intangible resources that prepare them to adopt innovations. An organization’s external linkages with other organizations and customers have long been acknowledged as playing an important role in fostering organizational innovation and change.11,12 One of the ways that these external linkages may foster organizational innovation and change among health care organizations is by cultivating greater organizational readiness and capacity to change. External linkages can take many forms for health care provider organizations, including referral networks, resource and informational sharing networks, and formal and informal advisory boards. In this study we focus on 3 types of linkages: (1) structural (ie, membership in a network and/or multiple sites/locations); (2) informational (ie, receive/share information with other outside organizations); and (3) customer/patient (ie, presence of a patient advisory board). These linkages can provide access to important resources and normative pressures 13 that may help health care organizations prepare for the implementation of evidence-based practices. To date, research on these external linkages has prioritized large, administratively complex organizations (eg, multihospital systems).14,15 Relatively little research, in contrast, has examined these linkages among smaller primary care practices in the U.S. and the extent to which they may support or hinder efforts to adopt innovative, evidence-based practices. The purpose of this paper was to examine whether different types of external linkages among 47 primary care practices participating in a statewide, community-academic partnership/cooperative focused on improving cardiovascular health outcomes were associated with greater change preparedness.
Change Readiness Climate
An accumulating body of research supports the importance of change readiness as an important antecedent to the implementation of innovations by organizations.16,17 The general premise is that higher levels of perceived readiness can foster greater effort toward implementing change, including greater likelihood of initiating change behaviors, more cooperative behaviors between organizational members, and greater persistence in these behaviors. 10 Change readiness is argued to be situational and varies across different organizational conditions.10,18 In our study, we follow the work of others in distinguishing between 2 dimensions of change readiness: change commitment and change efficacy.10,18 Change commitment was defined as clinic “members’ shared resolve to pursue the courses of action involved in change implementation.” 10 Change efficacy was defined as clinic members’ shared beliefs in their capabilities to pursue courses of action involved in implementing change.
Change Process Capacity
Change process capacity in our study refers to an organization’s ability to apply quality improvement strategies to improve care processes.19,20 Change process capacity differs from change readiness in its specific focus on the use of quality improvement strategies in health care settings (namely clinics), whereas change readiness refers more generally to an organization’s level of preparedness, both psychologically and behaviorally, to implement change. For example, change readiness survey questions typically refer to general organizational supports or barriers to implementing a new program or intervention (eg, “People who work here are committed to implementing this change”) while change process capacity questions refer to specific activities to improve quality (eg, “Setting goals and benchmarking rates of performance quality at least yearly”). Thus, while conceptually different, we expect change process capacity and change readiness to be correlated given that both focus on organizational conditions for pursuing change.
External Linkages and Change Preparedness
External linkages among primary care clinics may support efforts to pursue change by reducing some of the uncertainty surrounding the adoption of new programs. 21 That is, organizations are often reluctant to pursue innovations in boundedly rational situations where they must make decisions with incomplete information.22,23 External linkages can help organizations enhance the information available to make these decisions, and thus reduce uncertainty. 14
Types of External Linkages
Organizations can be simultaneously engaged in different types of linkages with external entities. We focus on 3 types of external linkages in our study: structural, informational, and consumer/patient.
Structural linkages are semi-permanent relationships between organizations, oftentimes with a governance structure that is legally distinct from the management structure of the individual organizations. 14 Structural linkages can provide access to capital, product and market information, opportunities to share management expertise, and economies of scale for some strategic priorities that can be centralized (eg, information technology). 24 Thus, structural linkages may provide access to resources that can support primary care clinics’ efforts to prepare for change. Thus, we hypothesize that:
Hypothesis 1: Relative to primary care clinics without a structural linkage, primary care clinics with a structural linkage will be associated with greater change preparedness.
Informational linkages are a looser and oftentimes more temporally limited relationship whereby participating organizations exchange information but maintain much of their decision-making autonomy (eg, strategic direction and operational goals). Primary care clinics may use informational linkages to broaden their environmental focus and monitor the behaviors and expectations of other organizations (eg, competitor clinics and hospitals) in their external environment. They may also provide a conduit for primary care clinics to acquire information quicker and help them mimic other organizations in their environment. 25 In the case of primary care clinics, informational linkages may help them monitor professional/industry standards and conform to the prevailing expectations regarding care delivery (eg, quality improvement strategies). Therefore, we hypothesize that:
Hypothesis 2: Relative to primary care clinics without an informational linkage, primary care clinics with an informational linkage will be associated with greater change preparedness.
Consumer/patient linkages refer to relationships an organization maintains with its “customers.” In our study, consumer/patient linkages are measured as the use of a patient advisory board to solicit feedback from customers. Thus, consumer/patient linkages are situated between structural and informational linkages in that they are more formal and enduring than informational linkages but are not as permanent or binding as structural linkages. Like informational linkages, consumer/patient linkages may broaden a primary care clinic’s environmental focus and allow it to gather information about patient-specific needs and expectations. In doing so, consumer/patient linkages may create normative pressures for primary care clinics to undertake efforts to adopt change. 25 Therefore, we hypothesize that:
Hypothesis 3: Relative to primary care clinics without a consumer/patient linkage, primary care clinics with a consumer/patient linkage will be associated with greater change preparedness.
Methods
Study Setting
Our study took place in the context of a statewide, multistakeholder cooperative effort to reduce cardiovascular risk and disparities among individuals across Alabama by supporting primary care providers, especially those in the most underserved areas of the state. The cooperative served as a convener of stakeholders and maintained a repository of ongoing cardiovascular disease (CVD)-related initiatives and resources. One of the cornerstone efforts of the cooperative was the implementation of the Heart Health Improvement Program (HHIP) in 51 clinics with suboptimal rates of BP control. The HHIP used a multi-pronged approach to quality improvement (QI), including practice facilitation (PF) and technical assistance, onsite and eLearning, and data transparency/reporting (ie, audit and feedback). Funded as part of the Agency for Healthcare Research and Quality’s EvidenceNOW: Building State Capacity program, 26 the overarching HHIP was designed to build internal QI capacity and increase the implementation of evidence-based guideline recommendations for screening and treatment for cardiovascular risk factors. The analysis reported in this manuscript is more narrowly focused on assessing the change readiness climate and change process capacity of the clinics involved in the HHIP. The overall study was approved by the [institution blinded for review purposes] Institution Review Board (Protocol #: 300002272), with the need for written informed consent waived. More details about the overall study can be found in the study protocol paper. 27
Data Sources
The analysis reported in this paper relied primarily on 2 surveys. One survey, the Organizational Readiness to Implement Change (ORIC), was administered to as many clinic staff as possible. A second survey, the Change Process Capacity Questionnaire (CPCQ), was administered to 1 member per clinic (eg, clinic manager and physician). Both surveys are described in more detail below. Paper-based surveys were left in the clinic by the practice facilitators during an initial on-site visit. Study participants scanned and emailed completed surveys to a study program manager. The overall clinic response rate was 92% (n = 47 clinics).
Measures
Our analysis included 2 summated scales related to change readiness, 1 summated scale related to change process capacity, 5 clinic characteristics, and 7 community characteristics. A summary of the key study concepts and definitions is provided in Table 1.
Key Variables and Definitions.

Readiness to Implement Change
Two dimensions of change readiness were assessed in the study using the Organizational Readiness to Implement Change (ORIC) survey, an instrument developed and validated by Shea et al. 28 Change commitment was operationalized as the average of 5 survey items, all of which were measured on a 5-point scale ranging from 1 = Disagree to 5 = Agree. Similarly, change efficacy was operationalized as the average of 7 survey items measured on the same 5-point scale.
Change Process Capacity
Change process capacity was assessed using 14 survey items from the Change Process Capacity Questionnaire.19,20 The Change Process Capacity Questionnaire was developed and validated by Solberg et al 20 as a measure of quality improvement infrastructure in primary care clinics. All items were measured on a 5-point scale, ranging from 2 (strongly positive) to −2 (strongly negative). Consistent with the approach adopted by Solberg et al, 20 these scores were summed across the 14 items to yield a variable that could take on values between −28 and +28 (more positive scores indicating greater quality improvement capacity/infrastructure).
External Linkages
Our analysis included 3 dichotomous variables to reflect the different types of linkages a clinic could maintain with external stakeholders. One variable indicated whether a clinic was part of a multi-organizational network or maintained multiple physical locations where it delivered patient care (1 = Yes, 0 = No). A second variable indicated whether a clinic shared information with other organizations (1 = Yes, 0 = No). Finally, a third variable reflected whether the clinic had a patient advisory board (1 = Yes, 0 = No).
Organizational and Community Context
The quantitative analysis included 3 clinic characteristics that reflected the general structure and staffing of the clinic. Ownership was a dichotomous variable that indicated whether a clinic was a Federally Qualified Health Center (FQHC) or not (1 = FQHC, 0 = not a FQHC). A second dichotomous variable reflected whether the clinic had been designated as a patient-centered medical home (1 = PCMH, 0 = not a PCMH). Finally, organizational maturity was accounted for with a variable reflecting the number of years the clinic had been operating (<5 years (referent); ≥5 years and <20 years; ≥20 years). Two variables were included to reflect the patient characteristics of the clinic (percentage of patients that were Black or Hispanic, percentage of patients that were uninsured or insured by Medicaid). Finally, urbanicity was included to reflect potential differences in the communities that the clinics operated in (metropolitan [referent], micropolitan; small town, or rural).
Statistical Analysis
The clinic was the unit of analysis (n = 47). Univariate and bivariate analyses were used to describe and assess the relationship between the different clinic characteristics and their change readiness and capacity. Initial exploration of the data indicated that the change readiness and capacity variables were not normally distributed (ie, left-skewed). Therefore, bivariate analyses used Mann-Whitney U tests for 2-level categorical clinic characteristics, and Kruskal-Wallis 1-way analysis of variance (ANOVA) was used for 3-level clinic characteristics. Ordinary least square regression models adjusted for heteroscedasticity were used to estimate the relationships between a clinic’s external linkages and change readiness and capacity while controlling for other clinic characteristics. All analyses were conducted with Stata 18. All relationships were considered to be statistically significant at P < .05.
Results
Clinic Characteristics
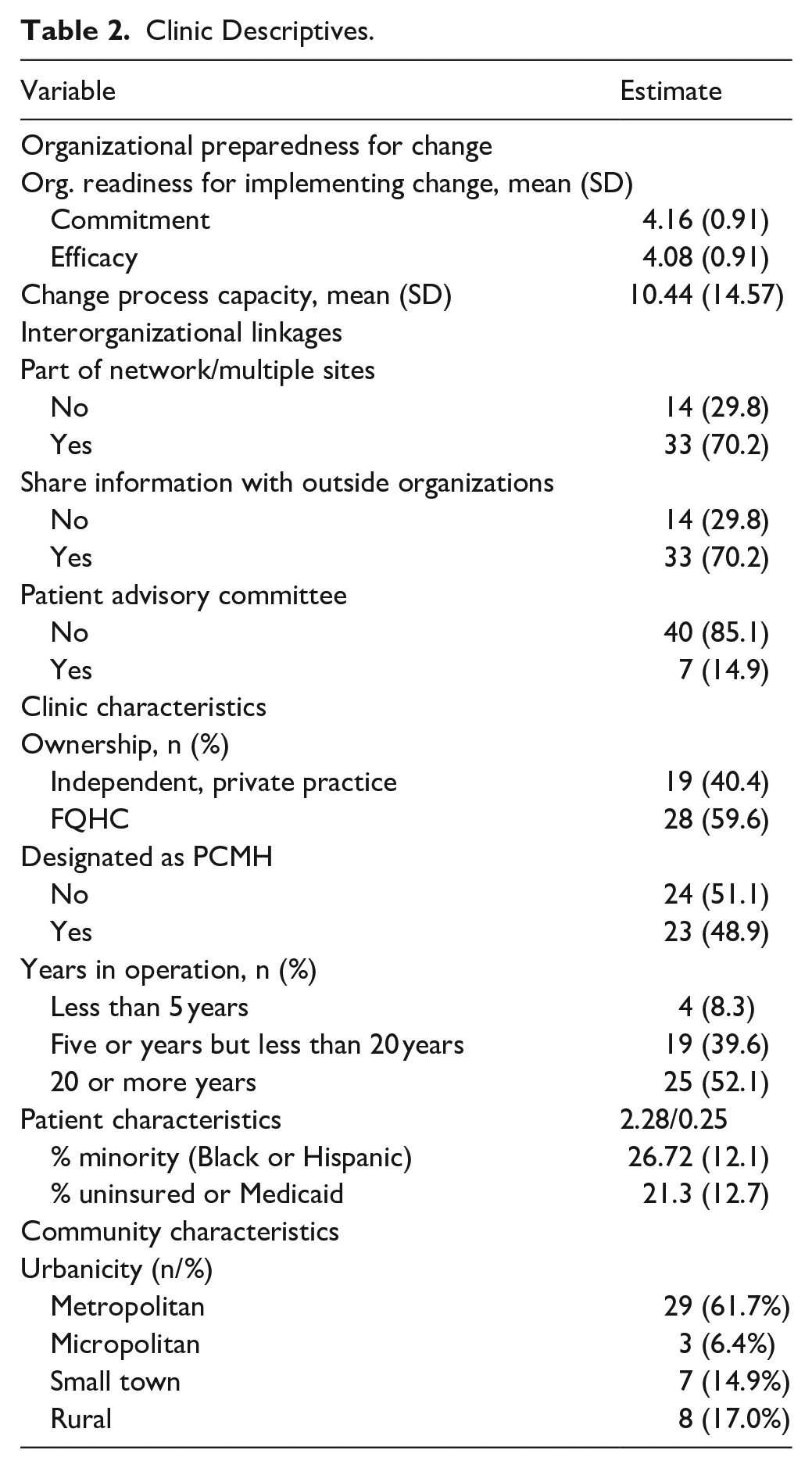
Nearly 60% (59.6%) of the clinics in our study were FQHCs (Table 2). The remaining clinics were independent primary care physician clinics (n = 19, 40.4%). Practices were nearly evenly split between being designated as a patient-centered medical home (n = 23, 48.9%) or not (n = 24, 51.1%). Over1-half (52.1%) of the participating clinics had been in operation for 20 or more years, followed by clinics that had been in operation between 5 and 20 years (n = 19, 39.6%). On average, participating clinics served 26.7% minority patients and 21.3% uninsured or Medicaid patients. Over three-fifths (n = 29, 61.7%) of the study clinics were in metropolitan areas, while 17% (n = 8) and 14.9% (n = 7) were in rural or small-town areas, respectively. Regarding external linkages, over 70% (n = 33, 70.2%) of the clinics were part of a network and/or had multiple physical locations. Likewise, 70.2% (n = 33) reported sharing information with outside organizations. In contrast, only 7 clinics (14.9%) reported having a formal patient advisory committee.
Clinic Descriptives.
Organizational Readiness for Implementing Change
On average, respondents reported a high level of change commitment and change efficacy. The mean level of change commitment across the 47 sites was 4.16 (SD = 0.91, range = 1-5) and the mean level of change efficacy was 4.08 (SD = 0.91, range = 1-5).
The bivariate analysis showed that clinics that were part of a network reported a lower median level of change commitment (Md = 4.14) than clinics that were not part of a network (Md = 4.79), a difference that was statistically significant (Mann-Whitney U = 9.98, P = .002; Table 3). Similarly, clinics that were part of a network reported a lower median level of change efficacy (Md = 4.00) than clinics that were not part of a network (Md = 4.80), a difference that was also statistically significant (Mann-Whitney U = 4.55, P = .03).
Comparison of ORIC: Change Process Capacity by Clinic and Community Characteristics.
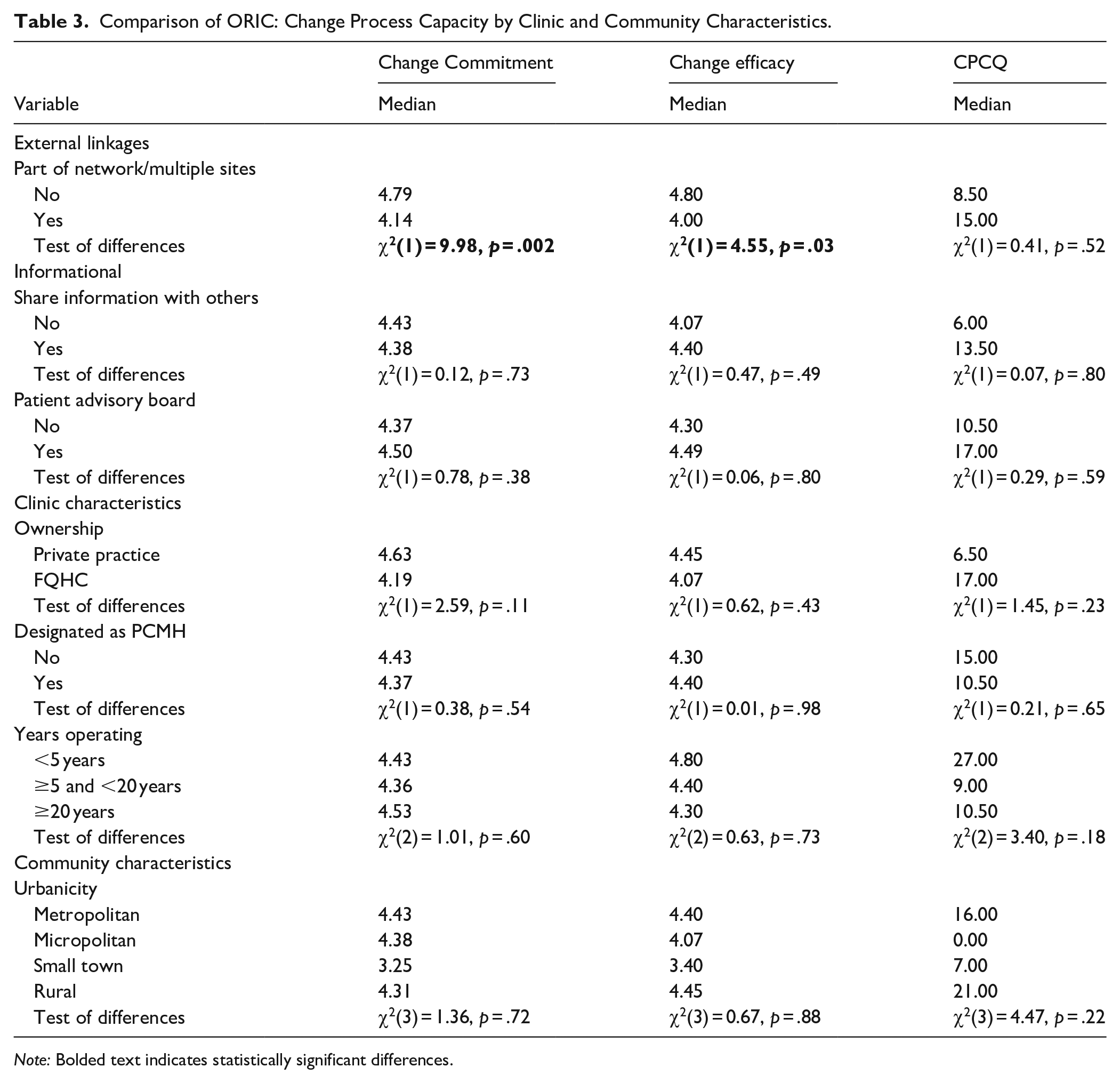
Note: Bolded text indicates statistically significant differences.
Consistent with the bivariate analysis, our multivariable analysis found that, relative to respondents from independent clinics, survey respondents from clinics that were part of a network were associated with lower reported levels of change commitment (b = −1.36, P = .006) and change efficacy (b = −1.16, P = .021), controlling for other clinic characteristics (Table 4). The other 2 types of external linkages, sharing information with other organizations and having a patient advisory board, were not significantly associated with either change commitment or change efficacy.
Heteroskedastic-adjusted Ordinary Least Squares Regressions, Relationship Between External Linkages and Organizational Preparedness to Change.

P < .05. **P < .01.
The multivariable analysis also revealed several notable significant relationships with clinic characteristics included as model covariates. Survey respondents working in more mature clinics reported lower levels of change commitment and change efficacy. Specifically, relative to survey respondents from clinics operating less than 5 years, respondents from clinics with 20 or more years of experience were associated with 1.20 (P = .038) lower levels of change commitment. Similarly, relative to survey respondents from clinics operating less than 5 years, respondents from clinics with 5 to 20 years of operating experience and 20 or more years of experience were associated 1.10 (P = .038) and 1.54 (P = .009) lower levels of change efficacy, respectively. Respondents working in clinics located in a small-town geographic area were associated with lower levels of change commitment (b = −0.70, P < .037) and change efficacy (b = −0.72, P = .034).
Change Process Capacity
On average, respondents reported a relatively high level of change process capacity (ie, quality improvement infrastructure), with a mean reported change process capacity score of 10.44 (SD = 14.57, range = −28 to 28).
The bivariate analysis found no statistically significant differences in the level of change process capacity for any of the 3 types of external linkages (Table 2). With respect to other clinic characteristics, respondents from FQHCs, relative to respondents from private practice, reported higher change process capacity (b = 26.73, P = .020).
Discussion
The purpose of this paper was to present an analysis examining whether different types of external linkages were associated with greater change preparedness among 47 primary care practices participating in a statewide, community-academic partnership/cooperative. Overall, participants reported relatively high levels of organizational readiness to implement change and chance process capabilities that are in line with those reported in the literature.29,30 These findings are promising and indicate that, despite well-known resource limitations in primary care settings,31,32 they still seem poised to undertake the change needed to adopt evidence-based practices that can support high-quality care. It is also conceivable, however, that the clinics that opted to participate in the study differed systematically in their change preparedness from other clinics.
Our analysis suggests that external linkages may be one factor that influences primary care clinics’ efforts to prepare for change, although not in the ways expected. Specifically, our analysis found that clinics with structural linkages in the form of network membership/multiple locations were associated with lower levels of change preparedness, which was contrary to what was predicted in hypothesis 1. One potential explanation for this counterintuitive relationship is that, despite acting as resource conduits for organizations (eg, managerial expertise, financial capital, and technology support), external linkages can also constrain behaviors and stifle innovation if an organization is over-embedded (ie, too many linkages and/or overdependence on linkages with the same partners). 33 Too many linkages may result in redundant or even conflicting relationships and resources. 34 Because external linkages come with costs (eg, time and money to build and maintain relationships), over-embeddedness may close off opportunities for innovation (eg, linkages with new partners with new ideas and investment in infrastructure). Unfortunately, our data did not allow us to examine the extent to which clinics may have been over-embedded in their relationships with external stakeholders but is something that should be considered in future research.
It is also notable that no other linkage types were associated with our measures of change preparedness, thus we did not find support for hypotheses 2 (information linkage) and 3 (consumer linkage). One potential reason why information linkages were not associated with change readiness is that our measure reflected the outward exchange of information – that is, whether a clinic shared information (eg, clinical information) with other organizations. While it is plausible and even likely that clinics that reported sending information to other organizations also receive information from these other organizations, it is also possible that the types of information exchanged in these linkages are not directly relevant for cultivating change and building QI capacity. For example, the exchange of clinical information in support of a referral to a specialist (or in return) may be less pertinent to establishing a foundation for organizational change than the exchange of strategic or operational information (eg, quality performance relative to goal/network benchmark). Finally, it is also conceivable that both informational and patient/customer linkages, compared to structural linkages, do not have sufficient formalization to influence clinic members’ attitudes toward or approach to preparing for change. Structural linkages, by definition, entail a formal relationship (eg, membership and ownership) and are designed to be strategic and enduring and thus, require greater commitment from organizations. By contrast, informational and patient/customer linkages tend to be more transactional, and a clinic could ostensibly terminate these linkages more quickly and with fewer organizational consequences.
It is notable that our analysis revealed relatively small correlations between the ORIC and CPCQ scores (~0.21-0.23, full results available from authors upon request). While we chose to include both terms under the label “organizational preparedness,” our findings suggest that they are distinct constructs. Notably, we also conducted a factor analysis that supported the conclusion that these are distinct constructs (results available from authors upon request). A close analysis of the survey items reveals 1 distinction. Consistent with its original formulation by Shea et al, the ORIC survey questions asked specifically about the program being implemented in this study (ie, the Heart Health Improvement Program), while the CPCQ reflects more general QI capabilities/infrastructure of the clinic. This difference is similar to the distinction made between organizational readiness for change and the implementation climate. 35 Given these distinctions, researchers may want to consider including the CPCQ as a part of their measurement strategy. To date, the ORIC has been included in more studies than the CPCQ, particularly in the implementation science literature. However, future research is also needed to assess whether the CPCQ is distinct from other organizational climate variables that researchers frequently consider (eg, organizational culture, implementation climate, and patient safety culture). Future research could also build on our work by examining whether different dimensions of organizational preparedness to change are associated with actual changes occurring within these settings, some of which is underway as part of the larger project.
Our analysis also revealed several notable findings with respect to our control variables. First, clinics that were in operation longer were associated with lower levels of organizational readiness to implement change. This finding is consistent with research that argues that organizations face a “liability of aging.” 36 According to this perspective, organizations “ossify” with experience because they increasingly rely on overlearned organizational routines that prioritize productivity and efficiency but reduce the search for novelty and opportunities for learning and change. It is also notable that clinics that were designated as PCMHs were not significantly associated with greater organizational change preparedness. The PCMH is ostensibly designed to support a clinic’s ability to engage in quality improvement, which inherently requires organizations to be receptive to and prepared to undergo change. One potential reason for the lack of a statistically significant relationship is the relatively high level of change preparedness to begin with (ie, a ceiling effect). It is also possible that our binary measure of PCMH was not sensitive enough to capture the different levels and dimensions of PCMH that might be expected to contribute to change preparedness.
Limitations
The results of our analysis should be interpreted with the following limitations in mind. First, one of the surveys (CPCQ) was completed by a single respondent at each clinic. Although we recommended that the survey be completed by the person(s) most knowledgeable of the clinic’s activities, it is plausible that respondents were not knowledgeable in all areas. Likewise, because our interest was in clinic-level phenomena (eg, readiness climate), best practice would suggest having multiple respondents from each clinic to ensure reliable and accurate responses. 37 Second, our analysis focused on the clinic as the unit of analysis, with only 47 clinics included in the study, which imposed some constraints on our statistical power and ability to control for confounding factors in our multivariable analysis. Finally, we adopted a cross-sectional approach to our analysis, which not only limited our ability to make causal inferences but also prevented us from assessing the possibility that change preparedness changed over time. 10
Conclusion
We examined whether different types of external linkages among primary care practices participating in a statewide, community-academic partnership/cooperative were associated with greater levels of change preparedness. Overall, the clinics in our study exhibited high levels of change preparedness, which provides a solid foundation for efforts to reduce CVD risks in critical primary care settings. Our study also suggests, however, that despite their many advantages, structural linkages are associated with lower levels of change preparedness among primary care clinics. Thus, primary care leaders and policymakers should consider the relationships between primary care clinics and other entities in their environment when developing and implementing programs to reduce CVD risks and improve quality in these settings. Making this opportunity a reality will require expanding beyond the traditional relational network of primary care, which has prioritized coordination and integration with other health care delivery organizations such as hospitals or health care specialists,38,39 and placed far less emphasis on relationships with community organizations.40 -42 The limited research that has considered formalized relationships between primary care clinics and community organizations suggests these linkages are beneficial, including improvements in diet, physical activity, and hypertension. Yet, too often, the opportunities afforded by these relationships are thwarted by primary care clinics’ lack of awareness of community organizations and their services 43 or a lack of resources to initiate and sustain these relationships. 44 Given the resource and workforce challenges currently faced by primary care clinics,45 -47 more support is needed to help them systematically identify, connect, and coordinate with community organizations.
Footnotes
Ethical Considerations
The study was approved by the University of Alabama at Birmingham’s Institutional Review Board (Protocol #: 300002272), with the need for written informed consent waived.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Agency for Healthcare Research and Quality (Grant number U18HS027946).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.