
Abstract
Background:
Effective hypertension management requires long-term lifestyle and medication adherence facilitated by regular physician. Higher continuity of care (CoC) is postulated to lead to better outcomes.
Objectives:
This study compares health outcomes of patients with hypertension receiving CoC from single family physicians over 5-year period with those treated by multiple physicians.
Methods:
Retrospective cohort study was conducted using electronic medical records from multi-ethnic Asian adults with hypertension and other non-communicable diseases. Patients managed in Family Physician Clinic (FPC) across 7 Singapore public primary care polyclinics from 2015 to 2019 were propensity scores matched with those treated by multiple physicians in General Clinic (GC) of the same polyclinics. CoC Index (COCI), health outcomes including blood pressure (BP), LDL-Cholesterol (LDL-C), cardiovascular complications and preventive measures were compared until 2021.
Results:
Analysis of 6520 patients (mean age 64.8 years, 56% female, 76% Chinese) showed FPC cohort had higher COCI (mean = 0.432 vs 0.073; P < .001). This was associated with further reduction in diastolic BP of 0.13 mmHg (P < .001) and LDL-C levels of 0.01 mmol/L (P = .001) per year faster than in GC, with higher proportion of patients meeting LDL-C targets (74.1% vs 68.0%; P < .001) in 2021. FPC cohort also showed greater influenza (OR = 2.88; P < .001) and pneumococcal (OR = 1.34; P < .001) vaccinations uptake. Subgroup analysis of patients with diabetes indicated better diabetic foot screening completion (OR = 1.34; P < .001). No significant improvement was found in systolic BP or cardiovascular complications.
Conclusion:
Higher CoC in FPC led to clinically relevant improvement in LDL-C and vaccination, but not BP or cardiovascular complication rates.
Introduction
The rising global prevalence of non-communicable diseases (NCDs) 1 necessitates an effective healthcare system for managing them. Singapore, a densely populated island state with no natural resources, faces a rapidly ageing population, leading to an increasing healthcare burden associated with NCDs. 2 The current fee-for-service primary healthcare system is episodic, where patients often consult different physicians, which is inadequate for managing NCDs that require long-term continuity of care (CoC) to improve health outcomes and prevent complications. In response, the Singapore Ministry of Health launched the “Healthier SG” programme in July 2023, 3 aimed at promoting preventive health and strengthening CoC by enrolling patients with their preferred primary care physicians.
CoC involves long-term follow-up from a single physician, fostering a stronger physician-patient relationship. Over time, physicians are more familiar with patients’ evolving demographic, clinical and social profiles, understanding their healthcare needs, values, and preferences through the ongoing interactions. It is expected that the greater CoC will lead to better results as health outcomes in primary care are closely linked to 3 crucial elements: contact, comprehension, and coordination. 4 Contact refers to regular interaction between physician and patient, fostering familiarity and trust. Comprehension emphasises physician’s understanding of patient’s medical history and personal circumstances, ensuring that care is tailored to individual’s needs. Coordination involves seamless collaboration among healthcare providers, ensuring cohesive and well-managed patient care. Together, these aspects contribute to better health outcomes by ensuring that care is personalised, timely, and well-coordinated.
Previous studies in different healthcare systems have reported variable effects of CoC on metabolic health outcomes including blood pressure,5,6 low-density lipoprotein cholesterol (LDL-C),7,8 glycaemic control (HbA1c),9,10 and preventive care uptake. 11 However, literature on the effect of CoC on health outcomes of patients with NCD in primary care of a highly urbanised multi-ethnic Asian community like Singapore is sparse. Evaluating the effect of CoC on local health is crucial to support the Healthier SG campaign.
In Singapore, 3 clusters of public primary care clinics (polyclinics) serve the multi-ethnic population. This study involves one of the clusters which operates multiple polyclinics in the southern and eastern regions. Patients are typically seen and managed by different physicians during each consultation at General Clinic (GC) in these polyclinics. For over a decade, the cluster has also implemented the Family Physician Clinic (FPC) where FPs (primary care physicians who have attained additional postgraduate qualification in Family Medicine) provide higher CoC. Patients at FPC, who often have more complex health needs, are scheduled to see the same FP for 15-minutes consultations, compared to the 5 to 10 minutes in GC. Patients can choose between FPC and GC for their chronic follow ups, with all still having access to GC for acute medical issues.
Hypertension is one of the leading NCDs managed in polyclinics. 12 Beyond medication adherence, FPs serve as health coaches encouraging patients to adopt healthier lifestyles and self-care behaviours aligned to clinical practice guidelines, 13 including low-salt diet, regular exercises, and self BP-monitoring. Attaining optimal blood pressure control reduces severe cardiovascular complications such as ischaemic heart disease and stroke. As part of holistic care of patients with hypertension, preventive care including influenza and pneumococcal vaccinations also plays a significant role in improving health outcomes for this population.14,15 Hypertension is a common condition among the elderly, who are particularly vulnerable to complications from influenza and pneumococcal infections. 16 Vaccinations can help reduce the risk of severe respiratory infections, which can exacerbate hypertension and lead to further health complications. 17 Therefore, understanding vaccination uptake rates among patients with hypertension is essential for developing strategies to enhance their overall health and well-being.
Hence, this study aims to compare the various health outcomes of patients with hypertension and other NCD receiving higher CoC by single FPs in FPC over 5-year period, with those who are managed by multiple physicians in GC of the same polyclinics during the same period.
Materials and Methods
Study Design
A retrospective cohort study was conducted on polyclinics patients with hypertension using electronic medical records (EMR) data from 1 January 2015 to 31 December 2019, with final outcomes assessed up to 31 December 2021.
Study Sites
Data for adult patients diagnosed with hypertension (ICD-10) were extracted from 7 polyclinics of the cluster.
Study Population
Inclusion Criteria
Patients aged 21 years and above who attended a designated polyclinic at least once a year during the 5-year observation period.
Exclusion Criteria
Patients who did not have at least 1 annual review for hypertension during the study period.
FPC Cohort
Patients with at least an annual FPC consultation during the study period.
GC Cohort
Patients who had GC consultations but never attended FPC.
Data Extraction
A retrospective review was conducted using de-identified aggregated data from EMR. In each clinic, physicians entered clinical notes and diagnosis, checked and ordered laboratory tests, prescribed medications, and made referrals via the electronic platform Sunrise Clinical Manager. Relevant data of both cohorts were retrieved from 1 January 2015 to 31 December 2021, including demographic variables such as age, gender, and ethnicity, diagnosis codes of other co-morbid conditions, and laboratory results.
Eligible patient data were extracted and transformed into an actionable format through the Extract, Transform, and Load process. The transformed data were loaded into the Electronic Health Intelligence System (eHINTS) for retrieval. A research informatics staff from the research department adhered to the data extraction methodology and retrieved the data via eHINTS. A trusted third party de-identified the data before secure transfer to the study team for analysis.
Matching of Control
Propensity score 18 was used to match patient in the GC cohort with each FPC patient in a 1-to-1 ratio. R software (The R Project for Statistical Computing) with package MatchIt 19 was used in the matching process using age, gender, race, baseline systolic blood pressure (SBP), diastolic blood pressure (DBP), LDL-C and creatinine, presence of co-morbidities of type-2 diabetes mellitus (DM), hyperlipidaemia, and pre-existing cardiovascular disease complications of ischaemic heart disease (IHD), stroke, transient ischaemic attack (TIA), and peripheral vascular disease (PVD) at their first visit of 2015. For subgroup analysis of patients with DM, the matching process was repeated to include baseline HbA1c as an additional parameter.
Continuity of Care Computation
Continuity of Care Index 20 (COCI) is widely used to measure CoC of patients over multiple clinical visits. The formula used was:

Where N = count of clinic visit, n j = count of clinic visits to physician j, s = unique count of physicians sharing clinic visits for the particular patient.
The COCI score was calculated based only on chronic visits to the polyclinics from 2015 to 2019, ignoring their acute visits. The score ranging from 0 (different physician for every chronic visit) to 1 (the same physician for all chronic visits). There is no universally accepted value for high CoC, but a recent systematic review 21 has identified 0.75 as a potential cut-off.
Outcomes
The health outcomes of clinical and laboratory data, and incidence of new cardiovascular complications based on ICD-10 diagnoses of IHD, stroke, TIA, and PVD were assessed until 31 December 2021.
Clinical data included SBP and DBP values recorded at every visit from 2015 to 2021. Laboratory data included LDL-C and HbA1c levels. Target LDL-C was based on the cut-offs that were used during the study period 22 (presence of IHD/stroke/TIA/PVD <2.1 mmol/L, DM <2.6 mmol/L, and hypertension/hyperlipidaemia <4.1 mmol/L).
Preventive health outcomes included completion of influenza vaccination, pneumococcal vaccination, diabetic foot screening (DFS), and diabetic retinal photography (DRP) at the study sites within the study period.
Statistical Analysis
Descriptive statistics were used to compare demographics and initial clinical parameters between FPC and matched GC cohorts. Mann-Whitney U test was used to compare differences in COCI scores between cohorts as it did not follow normal distribution as checked by QQ plot and Anderson-Darling test (data not shown).
Comparison of clinical parameters from 2015 to 2021 between FPC and GC groups was done using Linear Mixed-Effects Model (LMM) with package lme4 23 in R. LMM is a statistical model that extends traditional linear regression and allows modelling of time trend using hierarchical data of clinical measurement results per patient over multiple years. This model reports the effect size of patient belonging to a certain group on each clinical parameter measured. Chi-square test was used to compare patients who have achieved their LDL targets, had new cardiovascular complications, vaccinations, and microvascular screenings done, with odds ratio (OR) being presented.
All the statistical data analysis was done in R using 2-tailed test with P < .05 to determine statistical significance.
Results
From 92 691 patients with hypertension managed at the 7 polyclinics in 2015, 64 047 remained on follow up with at least annual visit until 2019. 54 833 of them had complete baseline data for matching and comparison. Among them, 3260 were managed in FPC and 51 573 in GC (Figure 1).

Flow diagram of the number of patients available for analysis.
After propensity score matching adjusting for confounders, 3260 were matched from GC as control. The baseline demographic profiles of the 2 matched cohorts generated from their first visit in 2015 were similar (Table 1). The mean HbA1c value of subgroup patients with DM were derived from a subset of 2092 patients.
Baseline Demographic and Clinical Parameters of the FPC Cohort and the Propensity Score Matched GC Cohort Selected as Control Based on First Visit of 2015.

Abbreviations: DBP, diastolic blood pressure; DM, Diabetes Mellitus; IHD, Ischaemic heart disease; LDL-C, low-density lipoprotein cholesterol; PVD, peripheral vascular disease; SBP, systolic blood pressure; SD, standard deviation; TIA, transient ischaemic attack.
The FPC cohort showed statistically significant higher COCI score compared to GC cohort (mean = 0.432 vs 0.073; P < .001) based on patients’ visits from 2015 to 2019 (Figure 2).

Boxplot of distribution of COCI score in FPC and GC cohorts.
Table 2 showed the effect size of the different cohorts in changes in clinical parameters result over the years. There was no significant difference in SBP values with both cohorts on average increased by similar amount per year (0.66 vs 0.68 mmHg; P = .577) from 2015 to 2021. This trend could be observed in Figure 3(A) which showed the yearly pattern of mean SBP increasing similarly in the 2 cohorts. However, DBP value showed further reduction of 0.13 mmHg per year faster in FPC compared to GC cohort (change per year = −0.12 vs 0.01 mmHg increase; P < .001). Figure 3(B) showed this trend with mean DBP in FPC cohort decreasing more rapidly over the years compared to GC cohort.
Clinical Parameters of Patients in Year 2015 and the Effect Size of Magnitude of Change Per Year in the Different Cohorts.

Abbreviations: CI, confidence interval; DBP, diastolic blood pressure; DM, diabetes mellitus; LDL-C: low-density lipoprotein cholesterol; SBP: systolic blood pressure.
P-value was calculated using Linear Mixed-Effects Model, except for the proportion of patients attaining their LDL-C target which used Chi-square test. Bolded values are those which are statistically significant.

Time series plots of trends of clinical parameters over the years in FPC and GC cohorts. A – mean systolic blood pressure. B – mean diastolic blood pressure. C – mean LDL-C level. D – mean HbA1c level.
For LDL-C, its level also showed greater decrease by 0.01 mmol/L per year in FPC compared to GC (change per year = −0.05 vs −0.04 mmol/L; P = .001) and the proportion of patients achieving their LDL-C target was also higher in the FPC cohort at the end of the observation period (74.1% vs 68.0%; P < .001). This pattern could be seen in Figure 3(C) showing mean LDL in 2021 in FPC cohort was lower than that of the GC cohort.
Subgroup analysis of patients with DM revealed FPC cohort did not achieve better glycaemic control compared to GC cohort. HbA1c in both cohorts on average decreased by 0.03% per year (P = .324) from 2015 to 2021. However, the mean HbA1c values in the FPC cohort was always higher than in GC cohort over the years (Figure 3D), although both groups had similar initial values (Table 1).
Regarding new cardiovascular complications, Table 3 showed no significant differences in the incidence of new TIA (OR = 1.53; P = .057), stroke (OR = 1.27; P = .142), or PVD (OR = 1.25; P = .314) between the cohorts. However, significantly more patients in FPC cohort developed new IHD (OR = 1.32; P = .016).
Number of New Cardiovascular Complications That Happened in Patients of the Different Cohorts by the End of 2021.

Abbreviations: CI, confidence interval; IHD, ischaemic heart diseasel; OR, odds ratio; PVD, Peripheral Vascular Disease; TIA, transient ischaemic attack.
P-value was calculated using Chi-square test. Bolded value is the one which is statistically significant.
Table 4 showed statistically significant increase in OR of patients in FPC receiving influenza (OR = 2.88, P < .001) and pneumococcal (OR = 1.34, P < .001) vaccinations to GC in year 2021. In the DM subgroup, more patients completed DFS (OR = 1.34, P < .001) in the FPC cohort but fewer had DRP done (OR = 0.84, P = .009) in 2021. This same pattern was consistently observed from 2015 to 2021, as shown in Figure 4 where FPC cohort always showed significantly higher OR for influenza vaccination (Figure 4(A)), pneumococcal vaccination (Figure 4(B)), and DFS completion (Figure 4(C)) but lower OR for DRP done in polyclinics (Figure 4(D)) when compared to GC cohort.
Number of Vaccinations Performed in All Patients and Microvascular Complication Screenings in the DM Subgroup of Patients in 2021.
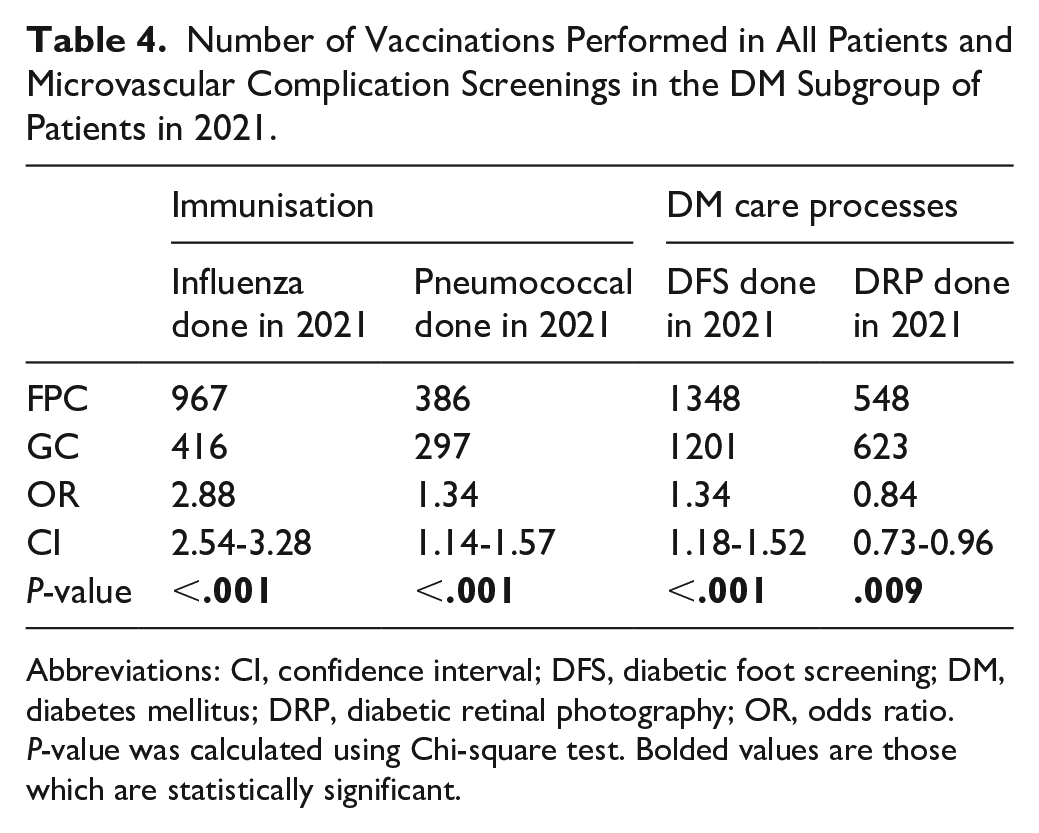
Abbreviations: CI, confidence interval; DFS, diabetic foot screening; DM, diabetes mellitus; DRP, diabetic retinal photography; OR, odds ratio.
P-value was calculated using Chi-square test. Bolded values are those which are statistically significant.

Plot of yearly Odds Ratio of vaccinations and microvascular complication screenings done in FPC cohort to GC cohort from 2015 to 2021. Error bars are 95% Confidence Interval. A – Influenza vaccination. B – Pneumococcal vaccination. C – Diabetic Foot Screening. D – Diabetic Retinal Photography.
Discussion
The study aim has been addressed by the various analysis performed. This study has first shown that FPC cohort received a significantly higher COCI score compared to GC indicating that FPC patients received greater continuity of care from their dedicated FPs over the 5-year period from 2015 to 2019. Although the mean score of the FPC cohort of 0.432 could be considered low, it was comparable to other published data where the cut-off values ranged from 0.236 to 0.44.24-26 The lower-than-expected score may be attributed to FPC patients occasionally being managed at GC for their chronic illnesses during the 5-year period, as well as the possibility of seeing different physicians in FPC due to absences. While having the same team or clinic can contribute to continuity, it is the ongoing relationship with the same physician that plays a more critical role. 27 Continuity through the same physician enables the development of trust, 28 which is essential for encouraging self-management.
Regarding individual clinical parameters, our study showed that FPC cohort did not necessarily demonstrate better BP results compared to GC cohort. The SBP did not show any statistically significant difference, while despite statistically significant improvement in DBP per year compared to GC, it was unlikely to have any clinical significance given the small magnitude. These findings aligned with previous studies indicating that blood pressure levels may not always improve in patients receiving higher CoC.6-8,29 The heterogeneity of real-world measurements and white coat hypertension may further distort BP documentation in EMR. Home BP monitoring was advocated but such remote data has yet to be fully integrated into the EMR.
The improvement in LDL-C levels per year also showed statistically significant difference, although its magnitude was small. However, when stratifying patients by whether they attained their LDL-C targets, a clearer pattern emerged, with more patients in FPC achieving their targets (74.1% vs 68%). This was understandable as usually all physicians would aim for patients to reach their LDL targets and once it was achieved they would not try to lower it further. This improvement in LDL-C has also been observed in other CoC studies. 7 The higher proportion of FPC patients who reached their LDL-C target is clinically relevant at the population level as it is hoped to give them the long-term benefit of better cardiovascular risk factor control.
In the subgroup analysis of patients with DM, the FPC cohort exhibited no significant improvement in HbA1c per year compared to CG. This finding is consistent with previous research indicating that higher CoC does not always translate to improved HbA1c level. 10 However, patients in FPC consistently had higher mean HbA1c value every year despite the successful initial matching using the first visit data. Patients in FPC were generally more complex, often presenting with higher prevalence of co-morbidities such as cognitive and psychiatric disorders, as well as significant social and economic factors which could affect their chronic condition management. Unfortunately, such factors may not always be captured in EMR. Furthermore, in lieu of focussing on deliberating on cardiovascular health issues such as lowering HbA1c level, FPs often prioritised and addressed immediate or more urgent issues emerging from these patients. Future research using natural language processing to analyse consultation notes can elucidate the impact of FPs in counselling and modifying the health-seeking and lifestyle behaviour of their patients while considering these various other factors.
While the results showed no difference in incidence of new stroke, TIA, or PVD, patients in FPC cohort had a higher incidence of being diagnosed with IHD (OR = 1.32), which contrasted with existing literature.30-32 This outcome was based on diagnoses coded by physicians during follow-up visits and should be interpreted in context. Firstly, if patient actually had been diagnosed to have IHD in a different location other than the polyclinics, and the polyclinic physicians did not add the new diagnosis code to patient’s EMR, the diagnosis would be missed by this study, leading to lower incidence of IHD than the true rate. Secondly, the rigorous training and certification that qualified FPs underwent had sharpened their clinical skills. Facilitated by the longer consultation in FPC, this may enable them to identify early features of IHD in patients resulting in early referral to the specialist. This allowed earlier confirmation of the diagnosis before an actual acute coronary syndrome could happen, which would still be reported as new IHD cases in the EMR by the FPs when patient returned for their follow up in the polyclinic. The potentially lower morbidity and mortality associated with earlier diagnosis and intervention cannot be determined in this study, which has yet to be linked to national disease and death registries.
In some healthcare systems, patients may be more inclined to follow medical advice immediately. However, in cases where patients are less responsive, the ongoing relationship with the same physician can help build rapport and gradually shift behaviour. 33 Most local FPs were trained to apply the Stott and Davis consultation model, 34 integrating preventive health as a key pillar of family medicine. This was reflected in the higher influenza and pneumococcal vaccinations uptake in the FPC cohort, potentially reducing morbidity and mortality associated with severe respiratory infections. Additionally, patients in the DM subgroup had more diabetic foot screenings completed in the FPC cohort. FPs were skilled in motivational interviewing and counselling techniques 35 encouraging DM patients to screen for potential microvascular complications that could be detected earlier and intervened. The CoC enabled FPs to identify care gaps and implement actions to mitigate deficiencies, similar to reports of enhanced preventive health outcomes in earlier studies.11,36 Although fewer patients in the FPC cohort underwent diabetic retinal screening, this was likely due to the data extraction focussing on screenings completed in polyclinics. Patients with prior diabetic retinopathy were typically managed by ophthalmologists, and this information was not available for analysis.
The strength of this Asian-centric study was the collation of data from a large pool of patients with diverse demographic characteristics across multiple study sites with data analysed over multiple years. Existing literature on CoC was primarily based on different healthcare systems, with studies examining as few as 100 patients from single clinic 10 to as high as 3 460 700 in nationwide study. 32 This study’s participant number ranked within the top half of the largest study populations in a recent systematic review that included 42 studies. 21 Another strength was the propensity score matching, which minimised biases in patient selection based on the data available in EMR.
However, this study was also limited by the data extracted from the database. Relevant confounding factors such as smoking status and body mass index were incomplete, and socioeconomic status or education level of patients were not recorded in the EMR. Additionally, confounders such as missed, delayed, or incorrect diagnosis coding were inherent limitations of retrospective database study such as this. Future research linking CoC to national disease and death registries, including relevant data such as referral and hospitalisation rates, is currently in progress. The results will provide more comparative health and process outcomes between patients managed in FPC and GC.
Another limitation that was not able to be analysed in this study was the longer consultation time that was inherent to FPC when compared to GC. The extra 5 minutes available in each FPC visit allowed for more thorough patient evaluations and discussions, which in addition to the CoC factor could lead to observed benefits observed such as advocating for vaccinations. It could be expected that they would work synergistically, as the higher CoC in FPC facilitated smoother conversations by the same FP from one consultation to the next, even if these consultations occurred months apart. This effectively created a continuous long consultation, as opposed to the episodic nature of visits in GC, where patients may be seen by different physicians who were not fully aware of what happened in the previous visits. This continuity of care was a key factor in achieving better health outcomes and encouraging preventive care, as it ensured consistent and comprehensive management of the patient’s health.
The long-term physician-patient relationship is key in promoting better self-management, particularly in chronic disease management. However, CoC in primary care clinics can still be considered somewhat “episodic” as FPs typically manage patients during scheduled visits every few months. To address this limitation, telemonitoring systems with feedback loops can enhance chronic disease management. These systems enable more frequent interactions between healthcare providers and patients, reinforcing health-seeking behaviour in a timely manner. This has been shown in previous OPTIMUM Study 37 where improved health outcomes were present at 6th month, and persisted even after telemonitoring stopped, at 12th and 24th months. This approach can complement the work of FPs by providing ongoing support between visits, and such model of healthcare can be explored as a possible method of further increasing CoC and ultimately improving the health outcomes of patients with NCD.
Conclusion
Overall, this study has revealed that higher CoC in the FPC cohort of patients with hypertension and other NCDs resulted in clinically relevant improvements in LDL-C control. FPC cohort also had higher uptake of preventive care, such as influenza and pneumococcal vaccinations, and higher odds of completing DFS for subgroup of patients with DM. Models of care that enhance CoC should be adopted to improve the long-term health outcomes of patients with NCDs.
Footnotes
Acknowledgements
The research team acknowledged the contribution of Mr. Aau Wai Keong for his help in data extraction and de-identification process, and Mr. Ng Ding Xuan and Ms. Eileen Koh for discussion about the statistical and analysis process.
Ethical Considerations
The study was reviewed by SingHealth Centralised Institution Review Board (CIRB 2022/2070) and granted exemption due to the de-identification of data in this retrospective cohort study.
Consent to Participate
Not Applicable.
Consent for Publication
Not Applicable.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by SingHealth Polyclinics Centre Grant.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Original data for this study is not possible to be shared as it contains de-identified data from SingHealth Polyclinics.