
Abstract
Background:
The association between social risk and biomarkers of inflammation remains underexplored in low-resource communities, where social risk and levels of inflammation differ from those in industrialized urban centers. This study aims to assess the association between levels of social risk and biomarkers of inflammation in adults residing in remote rural settings.
Methods:
This population-based, cross-sectional study involved 1392 community-dwellers aged ≥40 years. Social risk was assessed using the social determinants of health (SDH) included in Gijon’s Social Familial Evaluation Scale (SFES). Biomarkers of inflammation were measured through the Systemic Immune-Inflammation Index (SII) and the C-Reactive Protein (CRP)/albumin ratio. Both unadjusted and multivariate models were fitted to determine the independent association between SDH and biomarkers of inflammation, treated as dependent variables.
Results:
The mean (±SD) age of 1392 study participants was 53.8 ± 11.5 years (59% women). The mean Gijon’s SFES score was 10.1 ± 2.6 points, the mean SII was 451.6 ± 240.5 × 109 L, and the mean CRP/albumin ratio was 0.13 ± 0.29. Unadjusted generalized linear regression models demonstrated direct significant associations between SDH scores and both dependent variables, including SII (β: 6.12; 95% CI: 1.35-10.89) and the CRP/albumin ratio (β: 0.03; 95% CI: 0.01-0.05). These associations remained significant after adjusting for demographics, level of education, and cardiovascular risk factors for both, the SII (β: 7.24; 95% CI: 2.08-12.41) and the CRP/albumin ratio (β: 0.03; 95% CI: 0.01-0.05).
Conclusions:
Social risk is directly associated with biomarkers of inflammation in the study population, suggesting that inflammation may be associated with adverse health outcomes in individuals with high social risk. Study results demonstrate that this association is not only evident in high-income regions but in underserved rural communities as well.
Keywords
Introduction
The social determinants of health (SDH) encompass non-medical factors that influence the conditions in which individuals are born, grow, live, work, and age. These factors include living conditions, economic stability, education quality, social relationships, support networks, and access to healthcare. 1 SDH are used to assess the social risk faced by individuals and have been shown to play a significant role on health outcomes, particularly in vulnerable populations, as they can influence the occurrence and progression of chronic conditions and diseases.2 -4
A significant body of evidence suggests that inflammation plays a central role as a key factor mediating the relationship between social risk and negative health consequences.5 -7 However, much of the existing evidence on the association between social risk and levels of inflammation does not fully address potential differences related to the diverse settings in which people live. Evaluating the mediators of the consequences of social risk should be tailored to the distinct circumstances of individuals residing in rural or urban settings. 8 Rural populations often face unique social challenges such as limited access to healthcare, restricted educational opportunities, and smaller support networks. In contrast, urban populations might encounter different stressors, such as higher levels of pollution, greater socioeconomic disparities, and more pronounced gender and racial disparities.
There is a gap in the literature regarding how social risk assessments should be adapted to these different environments. Most studies have focused on urban settings, leaving the experiences and needs of rural populations underexplored. Additionally, it has been suggested that some biomarkers of inflammation may be different in rural settings compared to industrialized urban centers due to distinct environmental conditions. 9 Addressing this gap is crucial for developing more accurate and adapted social risk assessments that can better inform about cost-effective public health interventions and policies aimed at reducing health disparities. It is also important to determine if the inflammatory response ensued through increased social risk differs in distinct settings.
The present study aims to assess the association between SDH and biomarkers of systemic inflammation middle-aged and older adults living in rural settings.
Methods
Results
Of the 1838 individuals aged ≥40 years enrolled in the study villages as of June 2024, 1392 (76%) completed the clinical interviews and laboratory exams required to investigate all the variables of interest. Of the remaining 446 individuals, 13 died or emigrated between enrollment and the invitation to participate in this study, 37 were unable to complete the interviews due to aphasia or severe cognitive impairment, 67 had any of the exclusion criteria detailed in the methods section, and 329 declined consents, mostly because their unwillingness to have blood drawn. Included individuals were younger, less often women, and better educated than those who were excluded (all differences at the P < .001 level).
The mean (±SD) age of 1392 study participants was 53.8 ± 11.5 years (median age: 51 years), 818 (59%) were women, and 747 (54%) had primary school education only. CVH metrics in the poor range included: smoking status: 69 (5%); body mass index: 436 (31%); physical activity: 73 (5%); diet: 265 (19%); blood pressure: 354 (25%); fasting glucose: 301 (22%); and total cholesterol blood levels: 170 (12%).
The mean Gijon’s SFES score was 10.1 ± 2.6 points (median: 10 points), The mean SII was 451.6 ± 240.5 × 109 L (median: 339.4 × 109 L; range: 42.1-1,922.6; interquartile range: 295.6-552.2), and the mean CRP/albumin ratio was 0.13 ± 0.29 (median: 0.06; range: 0.004-3.54; interquartile range: 0.02-0.11).
Table 1 depicts characteristics of study participants, categorized by SDH scores stratified by the median (unadjusted analyses). Participants with lower scores on the Gijon’s SFES were younger, less often women, had lower education levels, better physical activity, and were less likely to have blood pressure readings ≥140/≥90 mmHg, and total cholesterol levels ≥240 mg/dL.
Characteristics of 1392 Study Participants According to Scores in the Gijon’s Social Familial Evaluation Scale (Gijon’s SFES), Measuring Social Determinants of Health, Dichotomized by the Media (Unadjusted Analyses).

Statistically significant results.
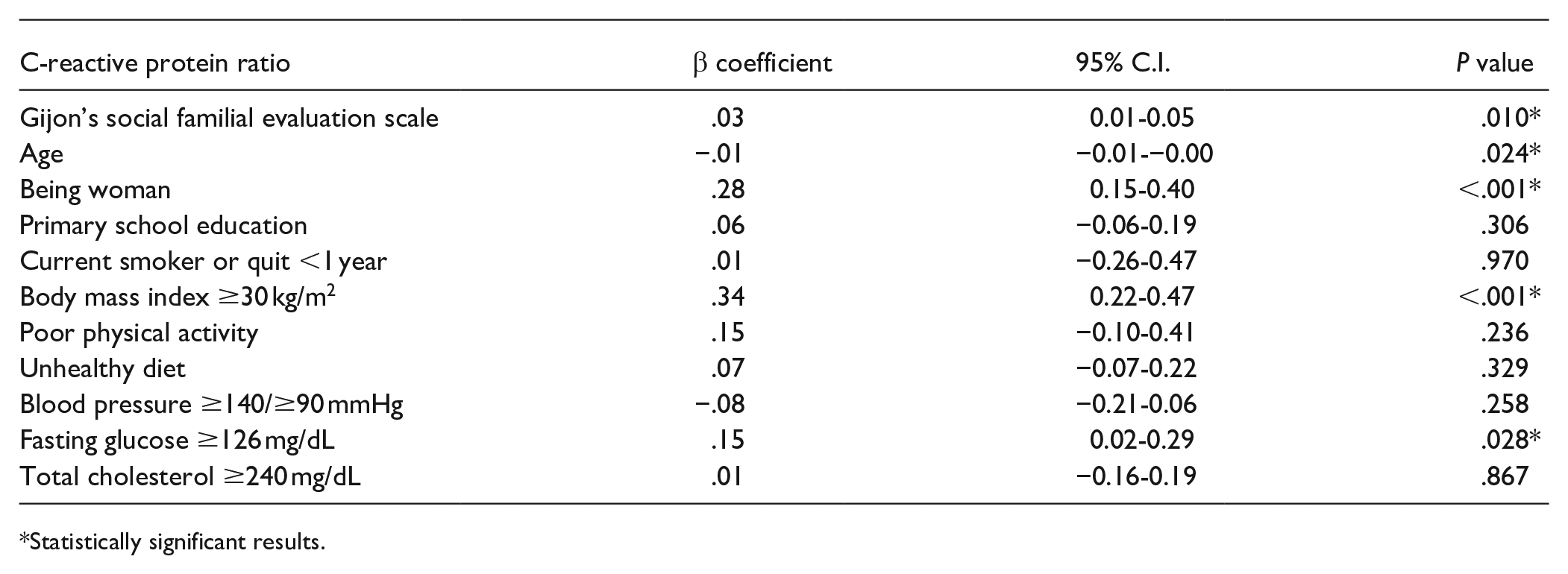
Unadjusted generalized linear regression models showed significant direct associations between Gijon’s SFES scores and the SII (β: 6.12; 95% CI: 1.35-10.89), as well as between the Gijon’s SFES and the CRP/albumin ratio (β: 0.03; 95% CI: 0.01-0.05). When these models were adjusted for age, sex, and education, Gijon’s SFES scores were still associated with both biomarkers of inflammation (β: 7.81; 95% CI: 2.69-12.94, for the SII, and β: 0.03; 95% CI: 0.01-0.05, for the CRP/albumin ratio). Likewise, Gijon’s SFES scores and both biomarkers of inflammation remained significantly associated in multivariate models that included all the covariates of interest (Table 2). Age and increased body mass index were significant covariates in both models, while sex and high glucose levels were significant only in the model assessing the association between Gijon’s SEFS score and CRP/albumin ratio.
Multivariate Generalized Linear Regression Models Showing Associations Between Scores in Gijon’s Social Familial Evaluation Scale and the Systemic Immune-inflammation Index (Upper Panel) and the C-reactive Protein/Albumin Ratio (Lower Panel), After Adjustment for All Covariates of Interest.

Statistically significant results.
Statistically significant results.
Discussion
In this cross-sectional, population-based study of community-dwellers aged ≥40 years living in rural settings, we observed a significant direct association between higher levels of social risk and biomarkers of inflammation, namely, the SII and the CRP/albumin ratio, in both unadjusted and multivariate models. These findings corroborate the results of previous studies conducted in industrialized urban centers, thereby expanding the applicability of the above-mentioned associations to resource-limited communities, where measurements of social risk and levels of inflammation differ.8,9
Research conducted in urban centers most often focused on a single component of social risk, such as social relationships or economic status. To mention some of these studies, hostile Scottish individuals with low socio-economic status exhibited higher levels of inflammatory biomarkers compared to their non-hostile counterparts. 19 The authors speculated that hostility may have adverse effect on the endothelium and elaborate on this effect as a potential cause of increased expression of inflammatory biomarkers. In another study conducted in Denmark, New Zealand and the UK, a strong association was found between social isolation with increased inflammation, and it was suggested that this social stressor precedes inflammation and hypothesized that dysregulation of the hypothalamic-pituitary-adrenal axis (related to social isolation) mediated the association between social isolation and inflammation. 6 In addition, another study using NHANES data demonstrated a significant association between social disadvantage and inflammation, which was more evident among middle-aged Hispanic men and women than in people from other ethnic and age groups. 20
A comprehensive evaluation of the association between a construct that includes various components of social risk—like those included in the Gijon’s SFES—and inflammation has not yet been conducted.6,19,20 Moreover, there remains uncertainty regarding whether the inflammatory biomarkers used in previous studies conducted in developed urban centers are applicable for assessing the association between social risk and biomarkers of inflammation in resource-limited rural communities. In the present study, we relied on a structured and validated field instrument that includes different determinants of social risk, that was specifically designed for individuals living in low- and middle-income countries. 10 Furthermore, the 2 biomarkers of inflammation determined in this study have previously demonstrated reliability in resource-limited rural communities.21,22
The few available studies in rural areas of low- and middle-income countries suggest that high social risk is a significant issue in these regions. Those studies demonstrated direct associations between social risk and poor cognitive performance, 23 as well as inadequate nutritional status. 14 Additionally, social risk has been linked to detrimental effects on cardiovascular risk factors and the progression of cerebral small vessel disease biomarkers.15,21 Furthermore, this condition has been found to be associated with increased premature mortality. 24
Understanding the link between social risk and inflammation has significant implications for public health interventions. By identifying specific social risk factors that contribute to increased inflammation, targeted interventions can be designed to improve health outcomes. For example, community-based programs that strengthen social networks, provide economic support, or enhance access to healthcare could potentially reduce inflammation and its associated health risks in vulnerable populations.
This study has several strengths. The use of a holistic approach to estimate levels of social risk together with the use of a field instrument (the Gijon’s SFES) specifically designed to be applicable in limited-resource populations, underscore the validity of our findings. This is relevant because social risk factors and their impact on biomarkers of inflammation may differ between high-income and low-income settings due to variations in resources, healthcare access, and social support systems. Likewise, the use of 2 different biomarkers of systemic inflammation enhanced the credibility of our findings since both were independently associated with higher levels of social risk. In addition, the selection of participants taken from the community and the systematic assessment of the different variables of interest ensure that the observed associations are robust and scientifically sound.
Limitations of our study extend beyond its cross-sectional design precluding the evaluation of the direction of the relationship between the main variables investigated. While biological plausibility suggests social risk acts as exposure and inflammation as the outcome, we cannot definitively conclude that higher levels of social risk cause increased expression of inflammatory biomarkers, especially in the light of some studies indicating that this relationship may be bidirectional. 7 While the selected biomarkers of inflammation are reliable, they only capture a part of the complex inflammatory response, and determinations of other biomarkers could provide a more comprehensive understanding of the relationship between social risk and inflammation. A sizable proportion of eligible candidates (about 15%) refused to participate because “fear of the needle,” a reason commonly observed in rural populations 25 ; this may have resulted in selection bias, although individuals who refused blood drawn had similar characteristics regarding age, sex, and level of education as those included in the study. Additionally, our results might not be generalizable to other rural populations. Subsequent studies should consider diverse populations to validate these findings across various rural settings.
In conclusion, the results of this study demonstrate that high social risk is associated with an increased expression of inflammatory biomarkers. These may, in turn, drive complex biological responses leading to clinical complications related to social risk. Departing from the population enrolled in this cross-sectional study, an ongoing prospective longitudinal study has been designed to demonstrate if inflammation serves as the link between social risk with adverse outcomes. Understanding this connection is critical for a better comprehension of the role of social risk in human health.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319251344427 – Supplemental material for High Social Risk and Biomarkers of Systemic Inflammation: A Population-Based Study in Middle-Aged and Older Adults Living in Rural Communities
Supplemental material, sj-docx-1-jpc-10.1177_21501319251344427 for High Social Risk and Biomarkers of Systemic Inflammation: A Population-Based Study in Middle-Aged and Older Adults Living in Rural Communities by Oscar H. Del Brutto, Denisse A. Rumbea, Emilio E. Arias, Kleber Arriaga and Robertino M. Mera in Journal of Primary Care & Community Health
Footnotes
Author Contributions
OHD: study design, manuscript drafting; DAR: study coordinator, data collection and analysis; EEA: data collection; KA: interpretation of laboratory exams; RMM: statistical analysis, significant intellectual contribution to manuscript content.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Universidad Espíritu Santo—Ecuador. The sponsor had no role in the design of the study, in the collection, analysis and interpretation of data, or in the decision to submit the manuscript for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.