
Abstract
Objective:
The Community Health Worker Institute (CHWI) addresses health-related social needs (HRSNs) by integrating Community Health Workers (CHWs) into patient care. This study explores the barriers and facilitators to HRSN referrals and the integration of CHWs within clinical teams.
Methods:
Qualitative interviews were conducted with CHWs, CHWI program staff, and clinicians from ambulatory care clinics. Semi-structured interviews, guided by the Consolidated Framework for Implementation Research, were audio-recorded, transcribed, and analyzed using rapid qualitative methods.
Results:
Preliminary findings found that while clinicians support the CHWI and referral program, time constraints during patient visits likely hinder effective screenings and referrals. CHWs are seen as valuable advocates but continue to face challenges due to confusion about their clinical role from patients and clinicians. Hierarchical power dynamics seen between providers and CHWs likely contribute to this confusion. Clinics with strong leadership, clear role delineation, and clinical site preparation appear to have better CHW integration.
Conclusion:
CHWs play a crucial role in addressing HRSNs, but their integration into clinical teams requires overcoming logistical and educational challenges. These findings offer insights for improving the HRSN referral process and integrating CHWs into healthcare systems.
Keywords
Introduction
The critical impact of social determinants of health (SDOH) has gained growing recognition within healthcare. According to the World Health Organization, SDOH are defined as “the conditions in which people are born, grow, live, work, and age,” and are shaped by the distribution of money, power, and resources at various levels, including global, national, and local. 1 Among the SDOH, there are distinct health-related social needs (HRSNs) such as housing instability, food insecurity, and access to care that significantly influence individual and community health outcomes. 2 Healthcare institutions are beginning to acknowledge a role in addressing non-medical needs of patients. 3 Addressing these needs are essential to reducing healthcare disparities. 4
As a result, there has been an emergence of screenings to support clinicians in identifying HRSNs in their patients. HRSN screenings collect crucial social information that can guide the allocation of resources and inform policy decisions aimed at promoting health equity. 5 Increasingly, health systems have adopted the process of gathering data on HRSNs for electronic health records (EHR) to coordinate clinical care.6 -8 Screening data collected from patients allows interventions to be tied to the patient’s specific needs and focuses on shared decision making. 9 Screenings can identify unmet HRSNs and can facilitate connecting patients to community resources. 10 Further research has continued to optimize HRSN screenings through improvements in efficiency, universal implementation, linkage of patients to resources, and integration into EHRs for ease of clinician use. 11
In parallel, Community Health Workers (CHWs) have emerged as a pivotal strategy in addressing HRSNs within healthcare systems and are recognized as vital components of the healthcare workforce. 12 CHWs empower patients to advocate for themselves and work at both the patient and institutional level to pioneer social justice. Clinicians acknowledge the role CHWs play in sharing community resources that they may be unaware of. 13 CHWs share lived experiences with the communities they serve, creating a vital bridge between healthcare systems and patient populations.14,15 A 2021 national survey completed by the National Association of Community Health Workers found that CHWs largely represented the communities they serve: 62.3% were Hispanic/Latino, 31.7% were Black or African American, and 4.8% were American Indian. 16 Evidence suggests that CHWs play a significant role in achieving health goals and improving health outcomes in diverse communities. 17 Previous studies have shown CHWs to be effective in increasing access to preventive care through cancer screenings and management of chronic health conditions such as diabetes, hypertension, and asthma.14,18 CHWs can lessen the cost of healthcare by reducing emergency department visits and hospitalization stays. 19 A study from our health system found CHWs effective in connecting over 78% of patients with social services and of those patients connected, over 93% of patients reported that their HRSN had improved or fully resolved. 20
Based on the growing evidence supporting HRSN screenings and the effectiveness of CHWs, the Community Health Worker Institute (CHWI) was launched. Our health system began screening patients for HRSNs in 2017 and in 2022 launched the referral to CHW component.20 -24 The CHWI identifies and connects patients with HRSNs to CHWs who assist in addressing HRSNs (see Figure 1). When a patient screens positive on the HRSN screening, the clinician asks the patient or family if they are interested in receiving assistance with their HRSN. 25 Upon patient consent, the clinician refers them to a CHW through the EHR for further assistance. CHWs then reach out to the patient or family to conduct an initial evaluation, gathering demographic information, obtaining consent for service navigation, and gaining a comprehensive understanding of their HRSN. CHWs aid patients by connecting them with community-based programs, assisting with benefit applications, navigating complex medical system care coordination, increasing patient education and empowerment, and providing social support among other services. CHWs maintain ongoing communication with patients until their HRSNs are resolved, until the family no longer requires services, or until the family is disconnected after multiple contact attempts.

Community Health Worker Institute Health-related social need screening to CHW referral process.
While CHWs are effective in addressing the HRSNs of patients, there is still a significant proportion of patients who are not successfully connected with CHW services. 20 There is high variability in referral rates across clinical sites ranging from 6.4 to 72.4% of eligible patients referred to CHWs. 20 Previous research in other health systems has identified the limited understanding of the CHW role by healthcare professionals to be a significant barrier to CHW integration within clinical teams. 26 There are no evidence-based guidelines on how to best integrate CHWs into healthcare settings along with limited research of CHWs’ personal perspectives on their integration into clinical teams. 27 Further research is needed to understand the variability in volume and success of referrals to CHWs across clinical teams in order to further optimize evidence-based screening and referral programs.
To explore perspectives from CHWs, program staff, and clinicians on HRSN screening and referral programs, we conducted a qualitative study in a large urban health system. The objectives were to: (1) identify the barriers and facilitators to HRSNs referrals to CHWs, and (2) assess CHW integration within clinical teams. The findings will inform improvements to and adaptations of the CHWI, with the goal of improving program delivery and CHW integration to more effectively address HRSNs. To our knowledge, this is the first study to explore perspectives from CHWs and clinicians on a CHW HRSN screening and referral program in a large health system.
Methods
Study Sample
We conducted semi-structured interviews at 2 ambulatory care sites within a large health system in the Bronx, NY. Purposeful sampling was used to capture diverse perspectives from program implementors across clinical sites.28 -30 Participants were eligible if they were 18 years or older, English-speaking, and had a current role within the health system that included engagement with the CHWI. Participants provided informed verbal consent.
Interviews
Employing the updated Consolidated Framework for Implementation Research (CFIR), a structured implementation science framework, we collected data on the barriers and facilitators to HRSN referral and CHW integration through qualitative interviews. 31 Semi-structured interview guides were developed based on CFIR constructs, encompassing program complexity and design, resource availability, cultural attitudes toward CHWs, communication practices, recipient needs, and adaptations (see Supplemental Table 1). 31 All interviews were conducted via Zoom between November 2023 and February 2024, with an average duration of 30 min. Trained investigators with advanced degrees and experience with qualitative research conducted the interviews. Audio recordings were transcribed for each interview, using an intelligent verbatim technique. 32
Analysis
Two team members trained in qualitative methods (PG and JH) employed a rapid qualitative approach to analyze data.33 -35 Each transcribed interview was coded and summarized separately by both team members. 32 Transcript summaries were organized by CFIR domains including innovation, inner setting, and implementation process with corresponding constructs within each domain. 31 Debriefing sessions were completed to reconcile any coding discrepancies, resulting in a combined and final transcript summary for each interview. 36 Transcript summaries included both direct quotations and paraphrased content from the interviews. Operational definitions of constructs were established between team members to facilitate the coding process. Matrix analysis was completed by analyzing data from all interviews organized by CFIR domain and constructs. Analytic memos were drafted for each CFIR domain and construct by extrapolating data from the matrix analysis summarizing key findings. Seminal quotes were elicited for key facilitators and barriers (see Supplemental Table 1). Results are organized into facilitators and barriers by CFIR domain.
Results
Participants
Ten participating completed interviews, including CHWs (n = 3), program staff (n = 3), and clinicians (n = 4). Of the 4 clinicians, 2 were pediatricians and 2 were internal medicine physicians. Program staff included 2 CHW supervisors and 1 program manager. There was an equal distribution of participants at each level from the 2 clinical teams. All participants were female with an average work history of 57.1 months. Participants were on average 34 years old with a range of educational levels. Each interview revealed valuable themes, highlighting facilitators and barriers across domains. Seminal quotes from participant interviews (Table 1) further illustrate these findings, offering deeper insight into key themes.
Seminal Quotes of Facilitators and Barriers to CHW Referral and Integration Organized by CFIR Domains and Constructs.
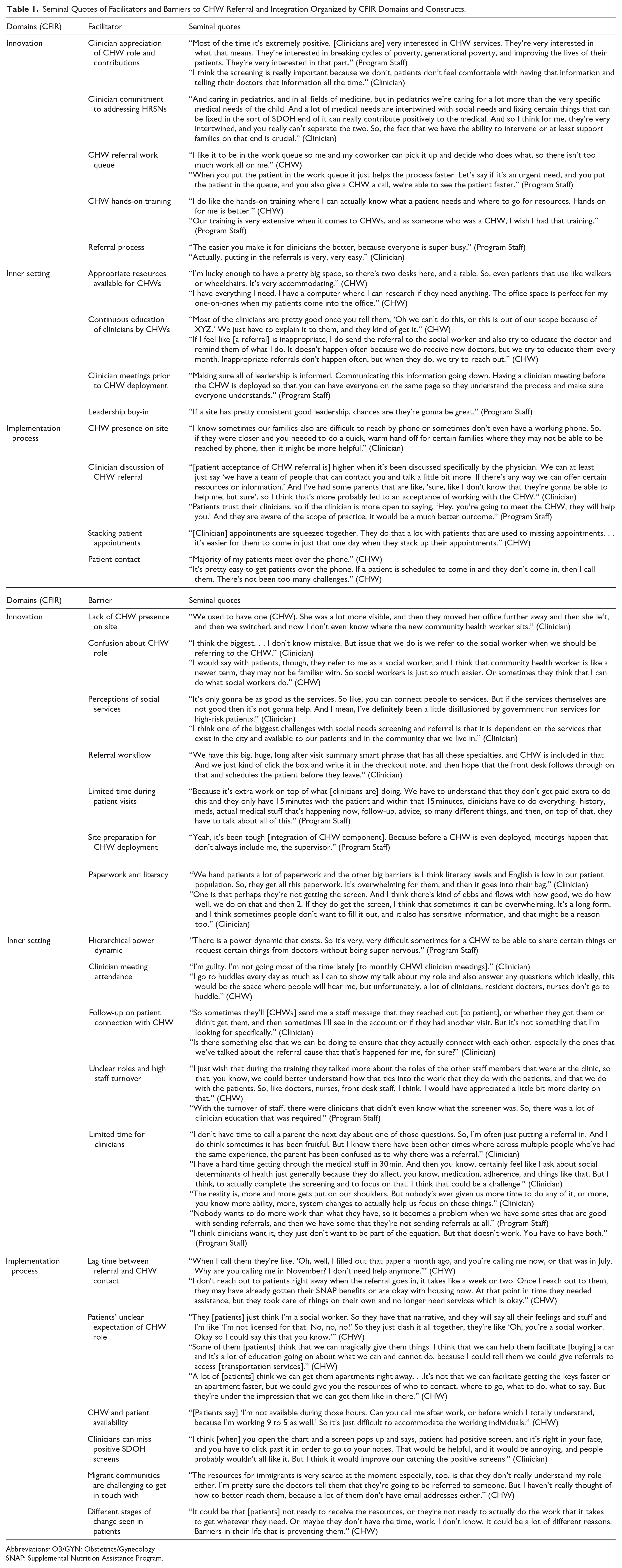
Abbreviations: OB/GYN: Obstetrics/Gynecology
SNAP: Supplemental Nutrition Assistance Program.
Innovation Domain
The innovation domain explores constructs related to the intervention being implemented, in this study the CHW referral and integration within clinical teams. A key innovation facilitator was a strong commitment from clinicians to collaborate with CHWs and integrate them into patient care. Clinicians recognized that information about HRSNs is often more effectively communicated by community members, and they valued the unique perspective CHWs bring to patient interactions. Clinicians demonstrated adequate understanding of the importance of addressing HRSNs, indicating broad support for the CHWI. The current workflow for CHWs to identify patients through EHR referral and the ease for clinicians to make referrals were both effective.
It has been so amazing. I am so grateful to have community health workers on our team. They provide such an integral role. There was . . .almost a year during the time I was faculty where we didn’t have a community health worker, and it was a lot more difficult for us to screen for social needs and to address social needs in our patients. So having that hands-on, on-site community health worker assistance has been so valuable. (Clinician)
There were significant barriers to innovation implementation. Clinicians reported confusion on the role of a social worker versus CHW. This same confusion was observed among patients, program staff, and CHWs. Participants reported that patients believed CHWs could offer the same services as social workers and clinicians sent inappropriate referrals to CHWs.
Sometimes patients will think I’m the social worker, so I must remind them that I’m the community health worker. Sometimes they think we do the same type of thing, but I just try to educate them on our role. (CHW)
A lack of visibility and integration of CHWs within the clinical environment limited meaningful interactions between clinicians and CHWs to ensure a closed loop process.
I don’t even know where the new community health worker sits. I know who she is, but I don’t know where she is, so I think it feels a little bit distant so it’s a little bit harder to connect. So, when you put the referral in, you just hope that something happens. And then I just see the notes come in and see they got connected, because I forget about it at that point, so you hope it works but you don’t really know. (Clinician)
Despite strong support for the CHW program, clinicians expressed skepticism on the social services offered. Clinicians described time constraints during patient visits resulting in CHW referrals being made without the clinician having discussed the CHW’s role with the patient. This led to confusion on the patient’s end about the purpose of the CHW referral. Clinicians expressed concern about literacy level and limited language options for the HRSN screening tool. CHW program staff reported not being included in meetings with site leadership prior to CHW deployment, resulting in CHWs being sent to sites where HRSN screening had not yet started. Clinician knowledge about the CHWI varied, creating disruptions in referral workflows.
Inner Setting Domain
In this study, the inner setting includes factors related to the health system and ambulatory care sites, including communication, available resources, and culture. Several facilitators and barriers were identified within the inner setting. A major facilitator was the empowerment of CHWs who reported feeling equipped with the necessary tools to perform their roles effectively.
I have everything I need. I have a computer where I can research if they need anything. The office space is perfect for my one-on-ones when my patients come into the office. (CHW)
CHWs who took the initiative to build relationships with clinicians reported receiving more referrals, underscoring the importance of ongoing interaction between clinicians and CHWs. Successful teams demonstrated that well-established workflows were crucial for integrating CHWs into clinical practice. Clinical teams with prior experience in CHW integration were better able to adapt and maintain effective workflows. Integration was especially effective when CHWI program staff met with clinicians, leadership, and administrative staff prior to deploying CHWs to the site. Leadership and clinician buy-in was crucial for information to be shared across clinical teams. Regular reinforcement of incorporating CHWs into patient plans through teaching sessions between attending physicians and residents was also important.
Although CHWs could effectively address incorrect clinician referrals through ongoing clinician education, a power dynamic inhibited CHWs from speaking up when errors in referrals occurred. In some cases, lack of a relationship between CHWs and clinicians further impacted the ability to communicate.
An outgoing CHW that is very willing to communicate with providers on a one-on-one level, and facilitate actual meetings, really results in breaking down a lot of barriers. And the reason that I say that is because there is a power dynamic that exists. So, it’s very, very difficult sometimes for a CHW to be able to share certain things or request certain things from doctors without being super nervous. (Program Staff)
Clinicians reported not having time to follow up on CHW referrals. High staff turnover disrupted communication and referral workflows, with clinicians admitting that they often skipped monthly CHWI clinician meetings where updates were shared resulting in poor communication on role delineation. Program staff noted that initiating change was challenging, especially in environments with established protocols and clinicians who perceive the screening as additional work with an already full schedule. Clinicians expressed feeling overwhelmed and lacked the capacity to ensure that HRSN screenings were completed before patient visits.
The reality is, more and more gets put on our shoulders. But nobody’s ever given us more time to do any of it, or more, you know more ability, more, system changes to actually help us focus on these things. (Clinician)
Implementation Process Domain
The implementation process domain captures the strategies and activities used to implement the innovation. Increased CHW visibility at clinical sites was identified as a key facilitator, enabling quick “warm handoffs” between clinicians and CHWs. The role of clinicians during patient visits was crucial in facilitating CHW referrals. When clinicians thoroughly explained the CHW’s role, patients were more likely to accept referrals. Setting appropriate expectations during these discussions was critical for patient buy-in.
Patients trust their providers, so if the provider is more open to saying, ’Hey, you’re going to meet the CHW, they will help you.’ And they are aware of the scope of practice, it would be a much better outcome. (Program Staff)
Program staff observed that CHW referrals improved when CHWs actively advocated for themselves when receiving recurrent inappropriate referrals and communicating with clinicians to clarify their role. Having a flexible process for patients to meet with CHWs was crucial. For example, being able to stack clinician and CHW appointments together was viewed favorably to allow patients to meet with CHWs in person.
Significant barriers were identified in the implementation process domain. A common issue reported was the lag time between when a CHW referral was placed in the EHR and when the CHW followed up with the patient. Participants reported that unclear expectations about what CHWs could provide led to patient discouragement and frustration, likely contributing to declined referrals. CHWs worried that some patients believed that their need could be resolved immediately, but many HRSNs require multiple steps and time to resolve.
They’re hoping that I’m the person that’s gonna help them solve all their problems. (CHW)
CHWs expressed frustration with their rigid work schedules, which often mirrored those of their patients, limiting their ability to meet patients outside of standard working hours. Certain patient populations, such as migrant communities, were more difficult to reach due to lack of phone or email addresses. The overwhelming amount of paperwork patients receive during clinical visits led to lack of screening or missing documentation for completed screenings, resulting in missed opportunities for patients with HRSNs to be referred to CHWs.
Discussion
This study sought to identify the facilitators and barriers to implementing a HRSN screening and referral to CHW program within a large urban health system. Understanding these factors is crucial for developing a replicable framework that other health systems can adopt to effectively screen for and address HRSNs. Our findings identified several critical barriers, including confusion around CHW roles, hierarchical power dynamics in healthcare, gaps in clinician communication, and disillusionment with social services. Key facilitators included strong leadership buy-in and adequate preparation of clinical sites. Addressing these barriers and leveraging facilitators can significantly enhance CHW integration and program success.
Clarifying CHW Roles
Our findings, consistent with previous literature, revealed confusion surrounding the roles of CHWs and their value in the healthcare system.13,26,37 A common misunderstanding among both patients and clinicians relates to the role of a CHW versus a social worker. A program in Michigan that paired CHWs with nurses and social workers reported similar challenges. 38 In response, the team developed a CHW role document that improved team integration and collaboration. 39 Establishing role clarity ensures CHWs can effectively complement the work of other team members.
Hierarchical Power Dynamics in Healthcare
Hierarchical power dynamics in healthcare settings can negatively impact CHWs’ integration within clinical teams and interactions with clinicians. 40 CHWs often excel in “soft skills”—such as empathy, communication, and adaptability—while healthcare systems tend to value and prioritize “hard skills” such as technical expertise and higher education credentials. 41 This imbalance may undervalue the unique contributions of CHWs, creating challenges for effective teamwork and collaboration. The strength of CHWs lies within their shared life experiences with the community members they serve, which fosters trust with patients. 15 Health systems can empower CHWs to further cultivate these skills rather than comparing them with the same metrics used to value clinical providers. This may require developing different objective methods in measuring the efficacy and success of CHWs. Addressing these power dynamics and recognizing the critical role of interpersonal skills is crucial for fostering a more inclusive and effective healthcare environment.
Leadership Buy-In and Preparation of Clinical Sites as a Catalyst for Success
Strong leadership buy-in emerged as a crucial facilitator for CHW program success. Effective leadership fosters an environment where care team members clearly understand the role of CHWs and how to collaborate with them. 40 Success in achieving shared objectives requires strong leadership. 42 Another study highlighted the significant role that supportive leadership plays in ensuring the successful implementation of CHW programs. 26
One way for leadership to support CHW integration is through adequate preparation of both clinical teams and patients. Clinical teams can initiate screenings and lay the groundwork before CHWs are deployed, ensuring a smoother integration process. Patients also require preparation for CHWs. CHWs express greater readiness for integration into clinical settings than patients do in utilizing CHWs. 43 CHW-led outreach programs have proven effective in enhancing patient-CHW relationships, fostering trust, and promoting a better understanding of CHW services.44,45 Building these relationships is key to improving patient engagement and program success.
Although many program staff and CHWs stated that a clinician champion is integral to a functioning team, previous research within this health system found little difference in referral rates at sites with or without clinician champions, however engagement levels of clinical champions was not examined. 20 More research is needed to understand the role and level of engagement required by clinician champions to improve implementation.
Gaps in Clinician Communication and Attendance
Low clinician attendance at team huddles, where CHW program updates are discussed, further exacerbated communication breakdowns. CHWs expressed frustration about attending team meetings to share program updates, but no clinician was present. Studies have demonstrated that teams with higher engagement, including consistent clinician attendance at meetings, have more successful program implementation. 46
Disillusionment With Social Services
Participants expressed disillusionment with the social services available to address HRSNs. This sentiment is consistent with studies that found that community members feel hopeless about the lack of resources to adequately address their HRSNs. 47 The process of seeking social services can feel dehumanizing when resource-limited programs prioritize cost savings over the holistic needs of vulnerable populations. 48 Importantly, CHWs—who often share similar backgrounds and life experiences with the communities they serve—are uniquely positioned to build rapport and foster a sense of camaraderie, offering a more humanizing approach to addressing HRSNs. 48
Study Limitations and Future Research
Our study is the first study to explore clinician and CHW perspectives on a CHW HRSNs screening and referral program in a large health system. This study had some limitations. First, the small sample size and inclusion of only 2 clinical teams limit the generalizability of our findings. However, these interviews provide valuable and broad preliminary insights on barriers and facilitators to CHW referrals and screenings that are applicable to most health systems and can guide improvements. Another limitation was potential selection bias, as the clinicians, program staff, and CHWs who participated may have been more actively engaged with the program, leading to an overrepresentation of certain perspectives. Additionally, as with most qualitative research, the absence of objective, quantitative data may limit the breadth and confidence of conclusions that can be drawn.
Future research should test targeted interventions addressing the barriers identified in this study. Testing implementation strategies to reduce referral lag times, enhance clinician engagement, and leverage technology could improve the efficiency and effectiveness of CHW referrals, thereby connecting more patients with unmet HRSNs to CHWs and social services. Moreover, further research should explore specific interventions aimed at strengthening relationships between CHWs and clinical teams. Overall, this qualitative study contributes to the growing body of research focused on integrating CHWs into health systems to better address HRSNs in historically underserved communities.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319251334210 – Supplemental material for Barriers and Facilitators to the Implementation of a Health-Related Social Needs Screening and Referral Intervention in the Bronx
Supplemental material, sj-docx-1-jpc-10.1177_21501319251334210 for Barriers and Facilitators to the Implementation of a Health-Related Social Needs Screening and Referral Intervention in the Bronx by Priya Elizabeth George, Jessica Haughton, Renee Whiskey, Samantha Levano, Hemen Muleta and Kevin P. Fiori in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We thank the Community Health Workers and program staff of the Community Health Worker Institute at Montefiore Einstein and healthcare providers from Montefiore Medical Group who participated in this study.
Ethical Considerations
The Albert Einstein College of Medicine and Montefiore Medical Center’s Office of Human Research Affairs institutional review board approved the study protocol (IRB 2017-8434; reference 107930; date: November 2, 2023).
Consent to Participate
All participants provided informed consent before participating.
Consent for Publication
Not applicable.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this work was provided by the New York Health Foundation.
Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Data consisted of qualitative interviews which will not be shared online due to anonymity.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.