
Abstract
Introduction:
This study aimed to test the introduction of Community Appointment Days (CADs) for patients on the Musculoskeletal (MSK) Physiotherapy waiting list in Lanarkshire, UK.
Methods:
A multi-professional team developed, implemented, and evaluated the first 2 CADs on 16th and 17th April, 2024. The mixed-methods design involved patients completing a “passport” (which included a survey) on the day and being followed up 4 weeks later by survey or interview. The patient management system was interrogated for waiting times and numbers returning to the service within 6 months. Structured thematic analysis was used to create a conceptual model from the qualitative data.
Results:
More than 3 times as many patients were booked into a CAD appointment (n = 443) compared to routine outpatient clinics (n = 133), and the vast majority reported positive outcomes. A total of 52 attendees (12%) were discharged on the day and a further 202 (46%) with Patient Initiated Review (PIR). Only 126 (28%) were given a follow-up 1:1 Physiotherapy appointment, although 63 (14%) did not attend on the day. Of the 443 booked, 26 (6%) returned for an additional review MSK outpatient appointment within 6 months.
Conclusions:
The CADs had positive outcomes for patients and were successful in reducing waiting times.
Introduction
Health systems in the US, 1 China, 2 and Europe 3 are grappling with the need for reform and calls for new models of care in the United Kingdom are not new. 4 The National Health Service (NHS) in Scotland is unable to meet the growing demand 5 and in response it has been suggested we need to put patients at the centre 6 and focus on prevention. 7
It can be difficult to successfully transform services in the public sector, where the political context influences change 8 and there is a historical reluctance to evaluate reforms. 9 That said, working collaboratively with communities can reduce healthcare resource use and improve health outcomes10,11 and identify when resources need to shift towards prevention and early intervention. 12
Providing services in the community can also be more cost-effective; a systematic review showed that costs were significantly less when adult rehabilitation was done at home rather than inpatient settings 13 and community-based self-management can yield significant savings. 14 The appetite for community healthcare instead of hospital-based appointments under the right circumstances has been demonstrated 15 and reaching out to patients can reduce community health clinic “did not attends.” 16
Reforming most people’s first point of contact with health services (primary care) has been challenging in Scotland, 17 but funding is available to test new models of care. 18 Community Appointment Days (CADs) in Lanarkshire, UK are one such example, based on the approach taken by a Musculoskeletal (MSK) Physiotherapy service in Sussex, UK. The holistic care they provided in a community setting resulted in reduced waiting times and a high percentage of patients able to self-manage afterwards. 19 The purpose of this study was to implement the new CAD model locally and capture the main outcomes.
Methods
A mixed-methods design was used to test the potential of CADs to improve health outcomes and reduce waiting times. The outcomes were more personalised care, increased access to services, and increased self-management. A multi-professional team was formed to develop, implement, and evaluate the 2 days.
Target Population
All patients on the MSK Physiotherapy waiting lists in 2 geographic areas were invited to attend the CADs. They received an appointment letter and information leaflet in advance, which allowed them to opt-out if they did not wish to attend. Those who attended could also request an alternative clinic appointment if they changed their mind on the day.
The CAD Model
The first 2 CADs took place on 16th and 17th April, 2024 in John Wright Sports Centre, East Kilbride, UK. Patients checked-in at Reception, then participated in a “What matters to you” conversation with a MSK Physiotherapist. This allowed them to be directed to interventions tailored to their needs; 1:1 Physiotherapy assessment, advice/guidance, rehabilitation/movement, equipment/adaptations, and engagement with a range of community supports. The CADs were staffed by those who would otherwise have been seeing patients in outpatient clinics on these 2 days, augmented by leadership input, project management, and evaluation staff.
Quantitative Methods
The patient management system was accessed to check how many had attended and whether or not they were subsequently booked for any follow-up appointments. Everyone attending was asked to answer survey questions on a “passport,” using either their mobile phone (with Information Governance approval) or on paper. No personal details were included, but passport data was linked to individual clinical records at check-out. Questions related to reason for attending, what matters to you, advice/plan agreed on the day, community organisations engaged with and feedback on the experience. It also asked for consent to being contacted for follow-up.
A 4-week follow-up survey was sent to everyone who had received a CAD appointment reminder, asking what had happened on the day, satisfaction with the appointment, and ability to cope with the issue they had been referred for.
Qualitative Methods
As attendees left the venue, verbal consent was requested for a short exit interview. Questions covered thoughts on attending, usefulness of the appointment, and satisfaction with any follow-up arrangements. They could not be recorded due to background noise, so they were used to inform, and obtain consent for, a possible follow-up interview.
Those who consented to a follow-up telephone interview were contacted 4 weeks after the event. Informed consent was obtained and they were asked to reflect on attending the event and whether any advice provided had been followed. Interviews were digitally recorded, transcribed, and stored on a NHS encrypted computer to ensure confidentiality. The data was subjected to structured thematic analysis, 20 which involved extracting keywords from quotes, assigning initial codes across these keywords, grouping codes into themes, and defining the concepts that emerged. Author AS did the initial inductive analysis, author HA independently did so for a sample of the output, and both agreed the final conceptual framework.
Ethical Considerations
While it is always advisable to seek ethical approval when human participants are involved, completion of the UKRI MRC & NHS Health Research Authority “Do I need NHS REC review” tool confirmed that this study did not need NHS Research Ethics Committee review. We have endeavoured to comply with established ethical standards throughout.
Results
The patient management system showed that 443 people were booked for the CADs over the 2 days and 380 attended. About 52 (12%) were discharged following the CAD, and a further 202 (46%) were assigned to Patient Initiated Review (PIR), which is discharge with the option to return within 6 months if required. About 126 (28%) of those booked were given a follow-up Physiotherapy appointment and 63 (14%) did not attend the CAD.
Passports were submitted by 364 people on the day, with slightly more doing so on their mobile (58%) than on paper (42%). In addition to all attendees having the “What matters to you?” conversation, 64% (n = 232) received Physiotherapy advice/guidance and/or rehabilitation/movement input (some had both) and 35% (n = 129) had a 1:1 Physiotherapy assessment on the day. From arrival to departure, people spent an average of 1 hr 8 min at the CAD, and 1 stayed for 4½ hr.
The follow-up survey was completed over 2 weeks by 81 of those booked for the CADs (17%), in an average of 3½ min. A similar number of respondents had attended on 16th (n = 34) as 17th April (n = 35) although 9 were not sure which day. A total of 14 people consented to a follow-up telephone interview.
Person-Centred Care
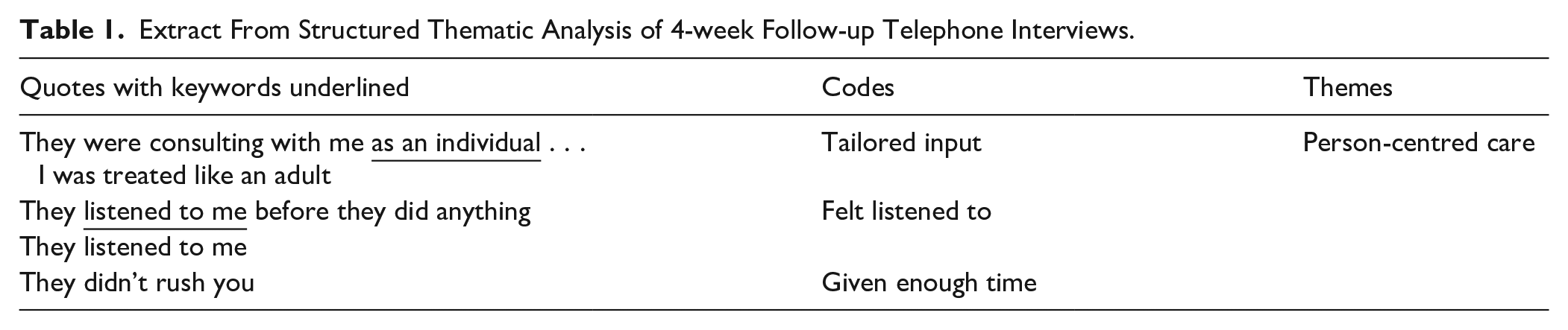
The “What matters to you?” conversations were intended to be an opportunity for staff to personalise the care to individual patients. Accordingly, the passport survey asked how patients felt about the effort that had been made to do so. In response, 354 (98%) said “every” or “a lot of effort” had been made to listen to what matters to them about their health issues and 349 (96%) said the same about including this in what to do next. This was reinforced during the 4-week follow-up telephone interviews where people felt the Physiotherapists had maintained a focus on them (Table 1).
Extract From Structured Thematic Analysis of 4-week Follow-up Telephone Interviews.
Increased Access to Services
A total of 443 people were appointed to the CADs, while only 133 would have been booked over 2 traditional outpatient clinic days. This means that an additional 310 had access to the MSK Physiotherapy service and a tailored suite of other inputs on the same day. Attendees were asked to rate the service on their passport survey; the average was 4.78 out of 5, with 85% giving it 5 stars.
In the follow-up survey, the vast majority were satisfied with all aspects of the CAD, including location, layout, advice provided, outcome, and community supports. About 32 of the 81 added positive comments, saying it was “a great set-up” or “well-organised and professional” and the “staff were very helpful.” One “thought this was a fantastic way to get a lot of people seen at once” and “didn’t feel awkward about discussing [their] issues, as the areas were separated enough to be private.” In the 4-week follow-up interviews those who had been given an individual clinic appointment were highly satisfied with the speed at which it had been arranged, and had found it useful.
14 survey respondents were not happy about the CAD arrangements. Four expressed dissatisfaction with the layout; this related to lack of privacy in an open hall, for example being treated in a group environment meant “more privacy was much-needed” or it was “too noisy and . . . I did not want persons around me listening to my health and personal details.” The others had not felt any benefit yet: “it’s too early to tell” or they hadn’t had as much time with a Physiotherapist as they’d wanted.
About 252 people (69%) noted on their passport that they had talked with 1 or more of the community support organisations present. Figure 1 shows that the most popular was Active Health/Leisure (n = 96), followed by Versus Arthritis (n = 87), Pharmacy (n = 72), Podiatry (n = 64), then Weight Management (n = 57). The benefit of having community supports present on the day was mentioned by several attendees in their 4-week follow-up interviews: “it was good to have people from different agencies” and “I was in awe at the amount of resources that were there.” For some patients this played a vital role, with 1 follow-up survey respondent saying: “if I’m honest if I was just given a leaflet or email address I would not have followed up.”

Percentage of all passports (n = 364) recording engagement with community supports.
Increased Awareness and Implementation of Self-Management
Supported self-management is defined here as “educating people about their condition and care, and motivating them to care for themselves better.” 21 The 4-week follow-up telephone interviews showed that there had been an increase in both awareness and implementation of self-management after the CADs. Some people had gained a better understanding of what had been causing their issues and had “got the answers [they’d] been looking for.” The advice provided had helped people understand that their issue was to be managed rather than cured: “it gave me peace of mind.” In terms of implementation, people assigned to Patient Initiated Review (where they could come back to the service within six months if their issue had not resolved) were happy to continue with the advice/exercises given and see if an appointment was needed at that time. A number of interviewees said they had used the information/advice given on the day and “it has helped.”
In the follow-up survey, reflections on coping with the issue their appointment had been about showed that 31 felt their ability to cope had improved since the CAD. Additional comments reinforced how attendees had “learned more about how to improve” and “came away understanding more about [their] illness and how [they] can improve [their] wellbeing.” Another described how they had put the advice provided and booklet given into practice, saying the “exercises are starting to help.”
Impact on Waiting Times
In one of the 2 areas involved, the waiting time was 33 weeks before the CADs and was on an upward trajectory. This dropped to 25 weeks after the CADs. The other area’s waiting time was also on an upward trend and reduced from 39 to 38 weeks after the CADs. Other areas’ MSK Physiotherapy waiting lists that were not targeted continued to rise during this time.
In addition, the patient management system showed that only 17 of those who left the CADs with Patient Initiated Review (PIR) had a return MSK Physiotherapy outpatient appointment within 3 months and a total of 26 had this within six months.
Discussion
A new model of MSK Physiotherapy Community Appointment Days has been successfully tested, having achieved the desired outcomes and, in common with other areas, 19 reduced waiting times. Almost the same number of staff as would have worked in the outpatient clinics saw and treated 3 times as many patients under the new model, and 12% of attendees were discharged on the day. Only 28% of attendees required a follow-up 1:1 Physiotherapy appointment and 176 of the 202 assigned to Patient Initiated Review (PIR) did not return within the six months. Although the “Did Not Attend” rate (14%) was slightly higher than outpatient clinics (10%), some of this difference may have been related to unfamiliarity with the new model being tested. If we had been able to work more collaboratively with communities,10,11 for example offering the option of self-booking, this may have reduced non-attendance.
Those who attended thought considerable effort had been made to listen to (98%) and include (96%) what mattered to them, which is positive. Although the vast majority were happy with the service provided, a few did not like the open arrangements or noise levels. Everyone had received information in advance telling them about the group setting, but some patients still said they were surprised when they came into the hall. This indicates that they may not have fully appreciated what would happen at their appointment, which is to be expected with new models of care.
The “What matters to you?” conversation at the start of each appointment was used by the MSK Physiotherapists as the basis for agreeing which of the available interventions were needed. For 69% this involved engaging with some form of community support such as leisure services, third sector partners, or another health-related intervention. People appreciated being able to speak to so many in the same place and on the same day and there was some evidence in the follow-up interviews that just being given a leaflet or email contact was unlikely to encourage the patient to follow-up. This is an important finding, suggesting signposting alone may be insufficient to achieve the kind of links to non-statutory provision that can lead to long-term engagement and life-changing input. However, it does rely on third sector partners having the capacity to engage, and continuing to do so for any future CADs.
Interestingly there was some evidence of both an increase in awareness and implementation of self-management following the CADs. Some people gained a better understanding of what was causing their issue, while others said the exercises were starting to help. This may have been reinforced for those assigned to Patient Initiated Review (PIR), since responsibility for any future appointment was transferred to the patient. It bodes well for reducing health service costs, as other services have found.13,14
Waiting times for both of the MSK Physiotherapy lists targeted in this study improved after the CADs, one by 8 weeks and the other by 1 week. The greater impact was seen for the smaller of the 2 waiting lists, an effect of the relative magnitude of the numbers involved. The second waiting list was double the size of the first and was also affected by staff vacancies, which reduced overall clinical capacity. Continuing to run CADs with greater appointment capacity than usual outpatient clinics appears to be an effective way of reducing waiting times, as long as referral numbers remain fairly stable.
Strengths and Limitations
A strength of this study is that it describes the implementation of a new model of care in a real-world setting, and captures a range of feedback to augment the system data available. While not conceptualised as original research, good practice processes were adhered to, for example informed consent for patient interviews.
This study is limited by being conducted on a single site and being reliant on self-reported recall for some of the data. However, the response rate for the passport survey was 96% and full details were available on recommended next steps for all CAD attendees from the patient management system. There may have been self-selection bias in the sample of patients who agreed to be interviewed and who completed the follow-up survey. For these reasons, the study results may not be generalisable to other areas.
Conclusion
The CADs had positive outcomes for patients, were successful in enabling some patients to self-manage and reduced routine waiting times. Further CADs are being run to test if the initial benefits are realised in the longer-term, including ongoing engagement with community supports. Utilising the networking skills of community groups 22 in future could improve things further, and it would be useful to undertake economic evaluation, given the current fiscal climate.
Footnotes
Acknowledgements
Many people contributed to this study, including staff at the John Wright Sports Centre in East Kilbride, the Physiotherapists and third sector partners who delivered the interventions, and the patients who provided feedback on their experience. We are grateful to the MSK Physiotherapy teams in Sussex, York, and Scarborough who shared their model and early learning.