
Abstract
Introduction:
The Undiagnosed Mass Clinic (UMC) at our institution is a clinical and research program created to address gaps in the early diagnostic phase of the cancer care continuum for patients with potential malignant neoplasms. All patients referred to the UMC are invited to participate in the UMC registry, which tracks operational and clinical metrics while maintaining a repository of blood and tissue specimens for future research.
Methods:
We conducted a retrospective cohort study of the first 100 patients enrolled in the UMC registry. We analyzed patient demographics, final diagnoses, and the time from initial consultation to final diagnosis.
Results:
Most participants were White (86%), non-Hispanic (93%), and married (72%). The mean (SD) age was 64 (13.9) years. The final diagnoses of the masses were categorized as malignant/neoplastic with malignant potential (n = 53), benign (n = 36), or requiring diagnostic surveillance (n = 10). The mean (SD) time from initial consultation to final diagnosis of malignant/neoplastic with malignant potential masses significantly improved from 37.4 (36.6) days for the first 50 participants to 17.3 (19.7) days for the next 50 participants (P = .006).
Conclusions:
These initial insights from the UMC registry will help direct future efforts to improve the care of patients with potential malignant neoplasms.
Introduction
When a patient has a newly discovered mass that may be malignant, the pathway leading to diagnosis is often uncertain. Frequently, patients, health care professionals, and health care systems experience challenges in obtaining a timely and accurate diagnosis in these situations, which may lead to considerable patient distress and potentially affect outcomes.1 -4 According to the National Cancer Institute, the prevalence of cancer in the US is expected to increase by 44% from 18.1 million in 2022 to 26 million in 2040. 5 Efforts to improve inefficiencies in how cancer is diagnosed, specifically with regard to time from presentation to diagnosis, are urgently needed because of this anticipated increase in cancer prevalence.
New clinical or radiologic findings that are concerning for a malignant neoplasm pose a particular challenge for clinicians because the differential diagnosis is often broad and may include a malignant tumor (solid or hematologic); an infectious, inflammatory, or postinflammatory condition; a benign tumor; or other conditions.6 -8 At our institution we observed that specialty practices at Mayo Clinic were often consulted for such undiagnosed conditions that were ultimately discovered to be outside their respective areas of expertise, especially hematology/oncology and surgical specialties.
Most people know of someone who has been affected by a potential cancer diagnosis. The events leading to diagnosis can cause substantial psychosocial distress, with delays affecting access to initial care, specialty referrals, diagnostic imaging, biopsy, and test results. 9 Furthermore, if a biopsy is deemed necessary, challenges around appropriate site selection and adequate tissue collection may further complicate the diagnostic process, increasing stress for both patients and clinicians.
In light of the broad range of potential diagnoses and the cumulative challenges during this early diagnostic phase of the cancer care continuum, we posited that patients would be better served by a dedicated program featuring general internists with expertise in consultative medicine. Consultative medicine is an emerging field in health care in which generalist physicians provide diagnostic care for patients with complex or multiple unexplained symptoms. 10 After conversations with the leadership of both the Mayo Clinic Comprehensive Cancer Center and emergency department, Mayo Clinic Division of General Internal Medicine created a program to address this clinical need. This effort began at the Mayo Clinic campus in Scottsdale, Arizona, and was later expanded to our other US campuses in Jacksonville, Florida, and Rochester, Minnesota. This expansion afforded broader understanding of existing operational and clinical challenges, as well as opportunities for efficiency and improving the patient experience. This combined clinical and research program was formally launched on January 7, 2022, and was named the Mayo Clinic Undiagnosed Mass Clinic (UMC). The mission of the UMC is to bring the strengths of a multidisciplinary health care organization to patients when comprehensive care is needed most (ie, when a new cancer diagnosis is being considered).
The UMC recognized that establishing patient cohorts and registries is an important aspect of enhancing health care through research and innovation. Health care institutions and researchers rely on registry data and biospecimens to develop new research initiatives and facilitate understanding of the pathogenesis of disease, especially for rare diseases and conditions.11,12 Approximately 75 active patient registries are currently maintained by the National Institutes of Health. 13 These registries facilitate research and seminal discoveries for various human diseases, including Alzheimer disease, cardiovascular disease, kidney disease, cancer, infertility, and genetic disorders. The initial insights gleaned from the UMC informed the creation of a research-based registry to prospectively collect data and biospecimens from patients with a newly discovered mass or masses. The UMC registry combines a biospecimen repository, clinical data, and operational data, such as time from initial consultation to final diagnosis, that will facilitate future research efforts to discern how efficient and accurate diagnoses may be obtained.
The long-term vision of the UMC is to transform how cancer is diagnosed by intentionally studying each step of the diagnostic process with a dedicated registry and biospecimen repository. This approach by the UMC will facilitate scientific discovery and enhance our knowledge and thereby have a transformative effect on this gap in the cancer care continuum. Here, we describe our findings from the first 100 patients enrolled in the UMC registry.
Methods
Ethical Oversight
The UMC registry program was initially reviewed and approved by the Mayo Clinic Radiology Research Committee. The program protocol was then reviewed and subsequently approved by the Mayo Clinic Institutional Review Board (IRB, #45CFR46.111) as a greater than minimal risk study. All requirements for approval of research were met. Any incremental changes to the study design or procedures during the course of the study continue to be appropriately reviewed and approved by the Mayo Clinic IRB, which serves as the central IRB for all 3 Mayo Clinic campuses. Written informed consent is obtained for all study participants before participation. Patients provide consent to collection of operational and clinical data, in addition to blood samples and, when feasible, excess tissue from their clinically indicated biopsy procedures.
Setting
Potential UMC registry participants are identified and recruited from all 3 Mayo Clinic campuses in Arizona, Florida, and Minnesota. Participation at multiple campuses facilitates access to diverse patient populations and improves our study recruitment efforts. All 3 Mayo Clinic campuses use a common electronic health record platform (Epic Systems Corporation), which allows connection among all UMC sites.
Participants
Eligibility criteria for enrollment in the UMC registry includes patients seeking care at the UMC who have new or enlarging lymph nodes identified clinically or with imaging or a new mass evident in imaging of soft tissues, bone, spleen, adrenal gland, retroperitoneum, or an intra-abdominal location without clear organ association. All enrolled patients must provide informed consent and agree to participate in all aspects of the registry. Because the UMC registry began during the COVID-19 pandemic, patients were initially seen either by telemedicine video or in person, depending on their preference and the local practice.
Patients are excluded from enrollment if they are younger than 18 years, unable to provide informed consent, institutionalized, or pregnant at the time of screening. Patients with a known history of any condition or factor determined by the UMC investigator performing triage to preclude participation in the UMC registry or that may hinder adherence to participation are also excluded. In addition, patients with a solitary mass (without evidence of multisystem disease) involving the breast, brain, kidney, lung, ovary/adnexa, liver, pancreas, sinus, throat, or thyroid gland are excluded. During our initial preprotocol efforts, including specialty stakeholder meetings at all 3 Mayo Clinic campuses, we determined that these solitary masses were best addressed by our respective clinical specialty areas, which have established, mature workflows in place to provide care for these patients.
Sample Collection
To lessen the burden on study participants, blood samples for research purposes are collected at the same time as a scheduled clinical draw. The purpose of collecting these blood samples for the UMC registry is to allow future research in areas relevant to cancer diagnosis, such as somatic cell–free DNA testing, germline testing, proteomics, extracellular vesicles, and mononuclear cells for immunologic studies. Tissues for the UMC registry are collected at the time of a standard-of-care diagnostic tumor biopsy procedure, with the site determined clinically. Tumor tissue samples for research are collected only after diagnostic requirements for the standard of care are met. The interventional radiologist or surgeon performing the biopsy must have also determined that the additional tissue for research is safe to collect and will not substantially increase the risk of harm to the participant.
Data Collection
In this retrospective cohort study, we describe the first 100 patients enrolled in the UMC registry from the launch of the UMC (January 7, 2022) through May 1, 2024. Clinical data were abstracted periodically from patient health records during the study period. Study data were collected and maintained in a database created with REDCap research electronic data capture tools hosted at Mayo Clinic.14,15 Examples of abstracted clinical data include dates of initial clinical consultation, tissue diagnosis and initiation of treatment for those with malignant neoplasms, medications, laboratory test results, demographics, social economic status, health history, and any previous or current health conditions. The data abstraction was conducted by the study biostatistician with R programming, v4.3.2. 16 Information gathered from any genetic testing is also stored in the UMC registry database to facilitate future genetic research.
Data Analysis
We categorized the final diagnoses of the initially undiagnosed masses into 3 groups: benign, malignant or neoplastic with malignant potential, and planned diagnostic surveillance. These categories were selected after a thorough discussion with Mayo Clinic Comprehensive Cancer Center leadership to most accurately reflect the novel cases encountered in the UMC (ie, distinguishing patients requiring specialty cancer care from those who may be adequately treated by generalist physicians). The malignant or neoplastic with malignant potential category was created to capture diagnoses, such as well-differentiated neuroendocrine tumors of the pancreas and gastrointestinal stromal tumors of the stomach, in which cancer care specialty surveillance is generally recommended. The planned diagnostic surveillance category was created to capture diagnoses in which the index of suspicion for a malignant neoplasm is low, but surveillance (ie, serial imaging) is deemed necessary. Lastly, the benign category was reserved for confirmed nonmalignant conditions.
Descriptive statistics were used to summarize patient demographic data and initial and final diagnoses. Continuous variables were summarized as mean (SD), and categorical variables were summarized as frequency (%). Differences between patients with masses categorized as benign and those with masses categorized as malignant or neoplastic with malignant potential were analyzed. For patients with masses categorized as malignant or neoplastic with malignant potential, an initial cohort of the first total 50 patients enrolled in the UMC registry (January 4, 2022, through April 18, 2024) was compared with a subsequent cohort of the next 50 enrolled patients (April 19, 2023, through May 1, 2024). Differences in categorical data were determined with χ2 tests, and continuous data were compared with t tests. All statistical tests were 2-sided, and P values < .05 were considered statistically significant. Analyses were performed with R software, v4.2.2. 16
Results
Of 175 participants who were initially assessed for eligibility during the study period, 49 were excluded from enrollment in the UMC registry: not meeting inclusion criteria (n = 34), referral to a more appropriate clinical specialty (n = 9), unable to contact (n = 1), other (n = 4), and lost to follow-up (n = 1; Figure 1). The other 126 patients were invited for a prescreening interview, and if they were deemed eligible for enrollment were scheduled for a visit to obtain informed consent. Of these 126 patients, 24 were not scheduled for a visit because of the following reasons: uninterest (n = 12), no show/scheduling difficulties (n = 4), unwilling to provide samples (n = 1), and other (n = 7). Of the 102 who consented to participate in the UMC registry, 2 changed their mind and withdrew their consent, and a total of 100 patients were included in our initial analysis of the UMC registry. Of these 100 patients, 86 provided blood and/or tissue samples (blood only, n = 37; tissue only, n = 8; and blood and tissue, n = 41), and 14 patients did not provide either blood or tissue samples. Forty-three participants were enrolled in the UMC registry in 2022, 34 were enrolled in 2023, and 23 were enrolled from January 1, 2024, through May 1, 2024.

Flow diagram of patient enrollment in the Mayo Clinic undiagnosed mass registry.
Most participants were women (54.0%), White (86.0%), non-Hispanic (93.0%), and married (72.0%; Table 1). The mean (SD) patient age was 64.7 (13.9) years, and 44% had at least a 4-year college degree. Most patients had masses that were ultimately categorized as malignant or neoplastic with malignant potential (n = 53), with fewer patients having masses categorized as benign (n = 36) or requiring diagnostic surveillance (n = 10; Table 2). One patient was lost to follow-up.
Participant Demographics. a

Continuous variables (age and time from consultation to final diagnosis) summarized as mean (SD); all other variables summarized as No. (%) of patients.
P values determined with χ2 (categorical) or t (continuous) tests comparing benign versus malignant or neoplastic with malignant potential groups.
Initial and Final Diagnoses of Masses From Patients Enrolled in the UMC.
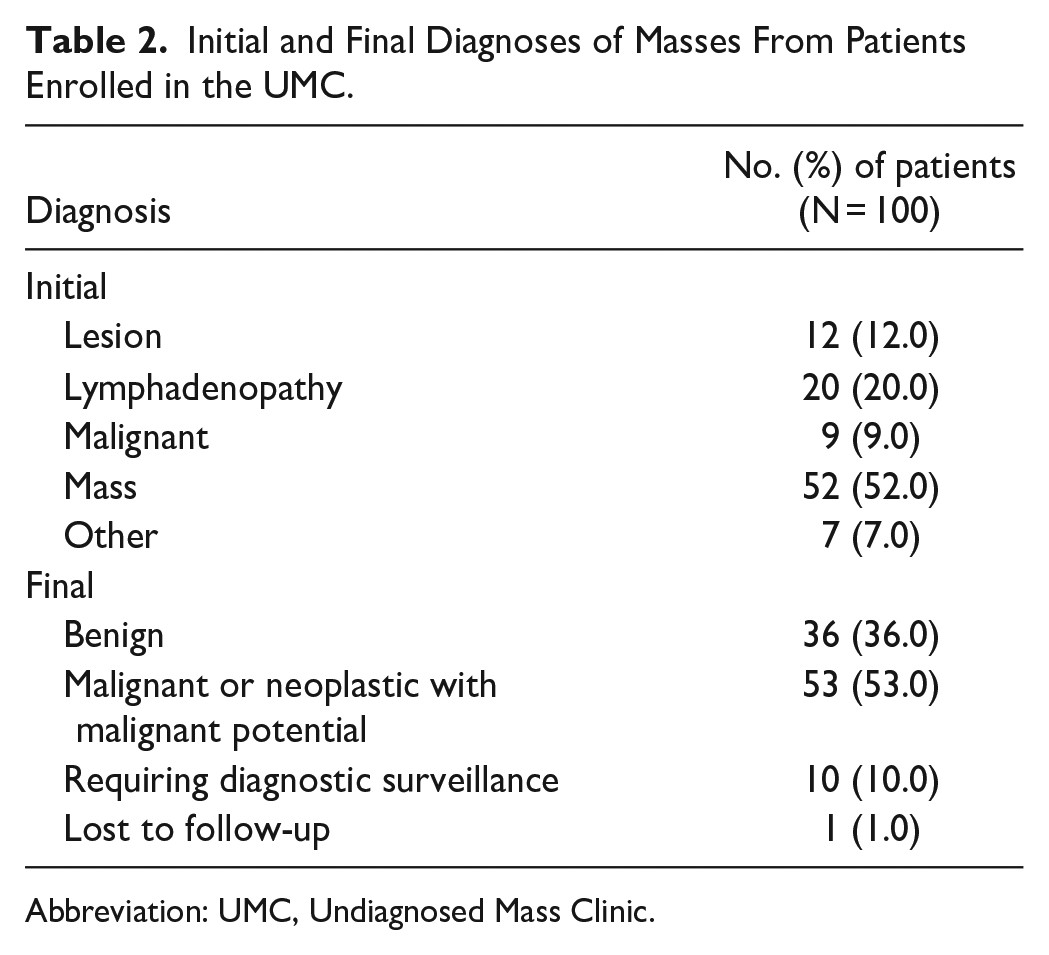
Abbreviation: UMC, Undiagnosed Mass Clinic.
Masses categorized as malignant or neoplastic with malignant potential included solid tumors and some hematologic cancers, including lymphoma and multiple myeloma. Patients with benign masses had diagnoses such as schwannoma, fibrous tissue, reactive lymph nodes, and some infectious diseases. Masses categorized as requiring diagnostic surveillance were defined as those without convincing evidence of a malignant neoplasm, either after tissue collection or clinical assessment without tissue collection, but warranting specific and prescribed surveillance, which typically involved repeated imaging studies at 6- to 12-month intervals.
Participants whose masses were categorized as benign were significantly younger than those whose masses were categorized as malignant or neoplastic with malignant potential (58.5 [15.3] years vs 68.9 [11.1] years, P < .001; Table 1). No other demographic data significantly differed between patients with benign masses and those with masses categorized as malignant or neoplastic with malignant potential, including sex (61% vs 45% women, P=.14), race (89% vs 81% White, P = .22), and the mean (SD) time from initial consultation to final diagnosis (27.6 [34.3] days vs 27.5 [31.0] days, P = .76).
For the 27 patients enrolled in the initial cohort (of the first total of 50 patients) whose masses were categorized as malignant or neoplastic with malignant potential, the mean (SD) time from initial consultation to final diagnosis was 37.4 (36.6) days (Table 3). In contrast, the 26 patients enrolled in the subsequent cohort (of the second total of 50 patients) with masses categorized as malignant or neoplastic with malignant potential had a significantly decreased mean (SD) time from initial consultation to final diagnosis (17.3 [19.7] days, P = .006).
Time to Final Diagnosis of Malignant or Neoplastic With Malignant Potential Masses for the First 50 versus Second 50 Patients Enrolled in the UMC.

Abbreviation: UMC, Undiagnosed Mass Clinic.
P value determined with a 2-sided t test comparing the initial vs subsequent cohorts.
Discussion
The UMC was created to meet a pressing clinical need with a new model of care and to serve as a source of discovery for patients with common but not well-understood masses that are concerning for cancer. This novel clinical program and registry allows for expedited diagnosis and subsequent care for patients while compiling data about these undiagnosed masses for future research purposes. One notable finding of the current study was that the majority (53.0%) of our first 100 enrolled patients had masses that were malignant or neoplastic with malignant potential. Approximately one-third of patients had confirmed benign conditions, and 1 in 10 required planned diagnostic surveillance. In addition, a comparison of participants according to final diagnosis showed that patients with malignant or neoplastic with malignant potential masses were significantly older than those with benign masses. These results support the relevance of this registry in the diagnostic phase of the cancer care continuum.
The UMC is housed in the consultative medicine sections of general internal medicine at the 3 Mayo Clinic campuses. UMC internists have a developed skill set for understanding broad differential diagnoses and the diagnostic skills to narrow such differential diagnoses to a definitive diagnosis, whether malignant, infectious, inflammatory, or other conditions. Indeed, definitive diagnoses were determined for 90% of the first 100 patients enrolled in the UMC registry.
The cancerous masses collected in our biospecimen repository include various solid tumors and hematologic malignant neoplasms. Only 17 of the 53 (32%) masses are of hematologic origin, primarily lymphomas. The solid tumors, which comprise most of the malignant masses collected in this study, range from localized tumors, such as a sarcoma of the pelvis or lower extremity, to metastatic disease of the lung, colon, breast, kidney, or pancreas.
The underlying causes of the benign masses in this study were wide-ranging, including several infectious and inflammatory conditions. Many of these conditions posed little to no risk of morbidity or death for patients and included reactive lymphadenopathy, fibro adipose tissue, and hemangiomas. Other conditions were potentially more serious, including sarcoidosis, lymphogranuloma venereum, and osteomyelitis, and required a high index of suspicion to provide a timely and accurate diagnosis. The masses requiring diagnostic surveillance included unique findings, such as probable reactive lymphadenopathy with some degree of uncertainty, sclerosing mesenteritis, and 1 case of neck and shoulder pain with worrisome cervical spine lesions evident on magnetic resonance imaging performed outside of Mayo Clinic. For this case, positron emission tomography and clinical examination led to a diagnosis of polymyalgia rheumatica. The patient was treated by the UMC clinician with prednisone (15 mg, daily) and had a complete response, with imaging surveillance prescribed for the spine lesions that were lacking 18F-fludeoxyglucose avidity.
Because of the known psychosocial effects of delays in diagnosis on patients with potential malignant neoplasms,1,3 studying the factors that may mitigate such psychosocial adverse effects during the time of diagnostic uncertainty is a priority of the UMC registry. To begin to understand this important area of concern, the registry records the dates of initial contact, initial clinical consultation, biopsy (or biopsies if more than 1), definitive diagnosis, and initiation of treatment. Because of the iterative refinement of workflows, the time from initial consultation to diagnosis for malignant or neoplastic with malignant potential masses was 20 days shorter for the second cohort of 50 patients than for the initial cohort.
A guiding principle built into the UMC program is the commitment to simultaneous rather than sequential efforts. For example, administrative staff prioritize overnight or electronic acquisition of imaging studies performed outside of the UMC before the first clinical encounter. By investing in this resource-intensive effort, the UMC frequently receives and reviews images before the first clinical encounter, allowing tentative biopsy or additional diagnostic imaging to be ordered. Another example of this commitment includes consulting with our genetics department on the same day that a diagnosis is confirmed for solid tumors, which affords screening for germline gene variations before a cancer care specialty consultation. Because germline gene variations often affect treatment decisions, this proactive approach was instituted so that patients do not have to wait weeks for results from genetic testing before starting treatment. 17 Early contact with appropriate cancer care specialists also allows additional molecular testing to be ordered on the abundant clinical biopsy specimens, making the first clinical encounter with the cancer care specialist more efficient. In addition, others have highlighted the necessity of achieving timely diagnoses to facilitate enrollment of patients with severe disease in clinical trials before they become more acutely ill and must resort to the standard-of-care treatment.18,19 Therefore, monitoring efficiency metrics will be a priority of the UMC going forward.
Several insights were elucidated during the pre-protocol phase of the UMC (before 2022), which were confirmed after the launch of the UMC registry. These insights included the role of dedicated radiology champions at each site and our approach to optimal tissue collection for biopsies performed by the radiology department. This approach includes a target of 5 core biopsies for clinical diagnosis because of the increased tissue demands of molecular testing for most cancers, thereby providing a precision oncology approach to diagnosis. 20
Several limitations of the UMC registry should be noted. Collecting both blood and tissue samples from each patient is challenging for various reasons, including patient preference, timing the research blood draws with the patient’s itinerary, and inability to safely collect additional tissue specimens. In addition, some patients do not require tissue biopsy for diagnosis, such as the patient with polymyalgia rheumatica noted above. However, this may also reflect a strength of the program because skilled diagnosticians may be able to make a definitive diagnosis without subjecting patients to biopsy. Thus, the biospecimen repository is incomplete for some patients, which may limit future research. Key metrics, such as time from presentation to definitive diagnosis and then to initiation of treatment, require further understanding of patient-specific factors and establishing benchmark standards for assessing the outcomes of discrete interventions. Although women were well represented in our patient cohort, overall racial and ethnic diversity was lacking, which may limit the broader applicability of our findings.
Future endeavors for the UMC are determined collaboratively through regular team meetings and facilitated retreats. In these meetings, we have begun to assess patient-reported quality-of-life outcomes with various integrative interventions, including validated questionnaires and biofeedback interventions. This should provide a better understanding of the overall patient experience, with the potential to address psychosocial stressors in this context. We will include additional metrics, such as the time to a cancer care specialty consultation and the time to treatment or clinical trial enrollment, in the future because both of these metrics may serve as benchmarks to improve clinical access. We anticipate the use of the biospecimens in the UMC repository for targeted retrospective studies. Such studies may include the emerging role of cell-free DNA for diagnosis in population-based screening and for symptomatic patients. Other types of molecular testing of blood and tissue samples in our repository will be considered, as well, to assess whether improvements in definitive diagnoses are afforded by such precision tools. We also anticipate collaboration with other healthcare centers to enhance learning and innovation in this relatively unstudied field.
Conclusion
To our knowledge, this is the first published registry of initially undiagnosed masses in which operational and clinical factors are measured, biospecimens are collected from blood and tissue, and multidisciplinary care is managed by a dedicated group of internists. The aim of the UMC team of physicians, nurses, operational experts, project managers, biostatisticians, data scientists, and clinical research coordinators is to bring the strengths of coordinated care and a dedicated registry to address the uncertainty and distress felt by patients who have a potential cancer diagnosis and to ultimately improve outcomes. It has been said: “When one door closes, another one opens, but it can be hell in the hallway.” 21 Our mission is to get patients out of the hallway and into a place of certainty and, in doing so, fulfill our vision to transform how cancer is diagnosed.
Footnotes
Acknowledgements
The study team thanks Richard J. Gray, MD, for helping identify the gap and for his challenge to us to find a creative solution. We are grateful to Minetta C. Liu, MD, for advising on optimal biospecimen collection and to Fiona E. Craig, MD, for helping refine the blood and tissue collection protocol. Scott Kriegshauser, MD, was central to establishing the Radiology champion model. We also thank Regina L. Martin, MSN, RN, for helping to establish nursing protocols and triage and clinical research coordinator Bianca K. Montelongo for her support and patience during this study and assistance with registry review. We thank Lisa A. Marks, MLS, AHIP, for her support during the literature search for this study and Jewel J. Samadder, MD, for being a sage-sounding board as we began to scale this program. Most importantly, we thank all of the study participants, who, without their participation, this study would not have been possible. The authors have authorized Scientific Publications to submit the manuscript on their behalf, and the authors have approved all statements and declarations. Nisha Badders, PhD, ELS, Mayo Clinic, provided editorial suggestions on an earlier draft of the manuscript. The Scientific Publications staff at Mayo Clinic provided proofreading and administrative and clerical support.
Author Contributions
All authors participated in the study concept and design, analysis and interpretation of data, and drafting and revising of the manuscript. All authors have seen and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Mayo Clinic Helen and Paul Baszucki Fund. The REDCap research electronic data capture application used in this study is supported in part by the Center for Clinical and Translational Science Award (UL1 TR000135) from the National Center for Advancing Translational Sciences. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The funding source had no role in study design, collection, analysis, and interpretation of data, writing of the report, or decision to submit the article for publication.
Availability of Data and Materials
Deidentified study data that support the results may be shared beginning 9 to 36 months after publication of this article. Such data will be provided if the investigator who proposes to use the data has approval from an IRB, independent ethics committee, or research ethics board, as applicable, and executes a data use/sharing agreement with Mayo Clinic and the first author/corresponding author.