
Abstract
Introduction:
As males are less engaged with healthcare than females, they often present when a condition is more advanced, reducing the potential for early intervention. Little is known about why men are less engaged and what influences them to be more proactive. This study sought to explore men’s experiences of engagement with general practice.
Methods:
A qualitative descriptive study was nested within a sequential mixed-methods project. Semi-structured interviews were undertaken with 17 male staff and volunteers of the New South Wales Rural Fire Service about their experiences, attitudes, and preferences for general practice engagement. Thematic analysis was used to analyze data.
Results:
Five sub-themes emerged about men’s engagement with general practice. “Reasons for engagement” revealed motivations for seeking healthcare. “Seeking validation” explained how social influences impacted engagement. The “importance of relationships” highlighted the value men place on trust with the healthcare provider/team, and how this impacts engagement. “Interpersonal communication” addressed preferences for direct and authentic communication. Finally, “barriers to engagement” revealed the challenges in accessing care.
Conclusions:
Awareness of the barriers and facilitators to men’s engagement with general practice can inform strategies to improve care. This study suggests that health professionals play a crucial role in building therapeutic relationships with men and partnering with them in their healthcare journey to improve engagement and health outcomes.
Introduction
Life expectancy is a measure of a population’s overall health. There is a disparity between gendered life expectancy worldwide, whereby males continue to lag behind females by some 5.4 years. 1 While life expectancy is impacted by various factors beyond the sex a person was assigned at birth, gender impacts health behaviors, including help-seeking and engagement with healthcare, treatment response, and subsequent health outcomes. 2 Males outnumber females in non-sex-specific deaths, namely cancers of the lung, trachea, colon, and rectum, as well as blood and lymph cancers, ischemic heart disease, and suicide. 3 In addition, more males than females live with hypertension and diabetes, 4 face a higher overall burden of disease and are likely to die prematurely. 5
Gendered trends in healthcare engagement are well-established in Australia and internationally. 6 Literature consistently reports that males are less engaged with the healthcare system than females.7,8 When males do present with a health concern, they often do so at more advanced stages of illness, reducing the potential for early intervention and potentially resulting in worse health outcomes. 7 Several factors contribute to this pattern. Firstly, males may not be fully aware of primary care providers’ services, predominantly viewing general practice as a place for acute healthcare delivery. 8 Additionally, barriers to men’s engagement include difficulties in accessing general practice in a timely manner, as well as psychological factors, including the impact of masculinity and stoicism. 9 Such masculine norms have been identified as factors that impact men’s help-seeking behavior.8,10
General practice is the primary contact for people seeking healthcare in Australia. Australian general practices are often owned by a single or group of general practitioners (GPs) or are part of larger corporate businesses. 11 Practices are increasingly multidisciplinary, with teams comprising GPs, nurses, administrative, and support staff, often with co-located allied health professionals. Consultations in general practice are funded by Medicare, Australia’s universal healthcare scheme that seeks to provide affordable healthcare for all. 12 However, patients increasingly must also pay out-of-pocket co-payments to cover consultation fees. 13 This impacts engagement as people need to consider the financial implications of accessing care, and as such widens the socioeconomic divide in healthcare access.14 -16
Identifying how men in the community engage with general practice provides valuable insights that could improve service delivery, increase patient-centered care and potentially lead to better health outcomes. This understanding is particularly important for men, given their lower engagement with the healthcare system and generally poorer health outcomes. Therefore, this paper seeks to explore men’s experiences of engagement with general practice, to inform strategies that enhance male participation in primary care services across the adult lifespan.
Methods
Study Design
This study used a qualitative descriptive design and was undertaken as the second phase of a mixed methods project about men’s health. A qualitative descriptive study explores the human experience, facilitates a concise overview of the phenomena, and allows a clear description of the experience from the participants’ perspective. 17
Initially, a cross-sectional online survey was undertaken,18,19 and survey respondents were asked to participate in subsequent interviews. This paper reports the interview data focused on men’s engagement with general practice. Survey data18,19 and qualitative data about men’s views about preventive care in general practice are reported in separate papers given the volume and depth of data.
Participant Recruitment
Adult male volunteers or employees of the New South Wales Rural Fire Service (NSW RFS) were recruited to participate. While recruiting from a single organization may limit generalizability, this organization was specifically chosen to provide a sample of adult males from diverse educational and socio-economic backgrounds and geographical locations. The NSW RFS is a diverse organization comprising paid employees and on-call volunteers who engage with the service outside their other personal and employment roles. These people undertake a diverse range of roles and responsibilities, including emergency response (eg, firefighting, car accidents, flood response), as well as office-based roles, operational logistics, community support, and education. 20 As such, this organization provided unique access to a diverse group of men to enable the study to capture a cross-section of the community.
Social media advertisements, key informants, and snowballing were used to recruit survey respondents. The survey asked respondents to indicate a willingness to participate in the interviews. As over 200 respondents indicated interest, a purposeful sampling method was used to select participants based on variation of age, geographic location, and use of general practice. Prospective participants were contacted via email and invited to participate. If no response was received to two emails, another person with similar characteristics from the prospective participant list was approached.
Data Collection
Data were collected through individual semi-structured interviews conducted by the first author (RM), a nurse practitioner experienced in primary care. A semi-structured interview guide was developed, consisting of questions arising from the survey data and relevant literature8,18,19 (Figure 1). Due to the wide geographical distribution of participants, interviews were offered via telephone or videoconference, depending on participant preference. Interviews were audio-recorded, and field notes were taken during and after the interviews to assist in interpreting the data. Recruitment and data collection was undertaken between May and July 2023. Data were collected until no new information was forthcoming. 21

Interview Schedule Excerpt.
Data Analysis
Verbatim transcription was undertaken by a professional transcription company. The first author verified accuracy by comparing transcripts with the audio recordings before they were uploaded into NVivo 12, 22 for analysis. An iterative, 6 step process of thematic analysis, informed by Braun and Clarke, 21 was used to analyze the data. Initially, the first author immersed themselves by reading and rereading transcripts and listening to the audio-recordings. In the next step, coding of the transcripts was then undertaken and discussed with the research team, focusing on verifying codes and developing emerging patterns and themes. Member checking was not undertaken, although all research team members reviewed the transcripts, and two researchers (RM and CP) undertook coding independently. Sub-themes were identified within the themes, and then the team reviewed, defined, refined, and verified to ensure that all data had been captured. In the final step, quotes were then extracted to illustrate the data’s story in the research report. The Consolidated Criteria for Reporting Qualitative Research checklist (COREQ) was used as a guide to reporting. 23
Ethical Issues
The Human Research Ethics Committee of the University of Wollongong (Approval no 2022/225) and the NSW RFS approved the study. All participants provided informed consent and were advised that they could stop the interview at any time. Pseudonyms are used to protect confidentiality.
Results
Participant Characteristics
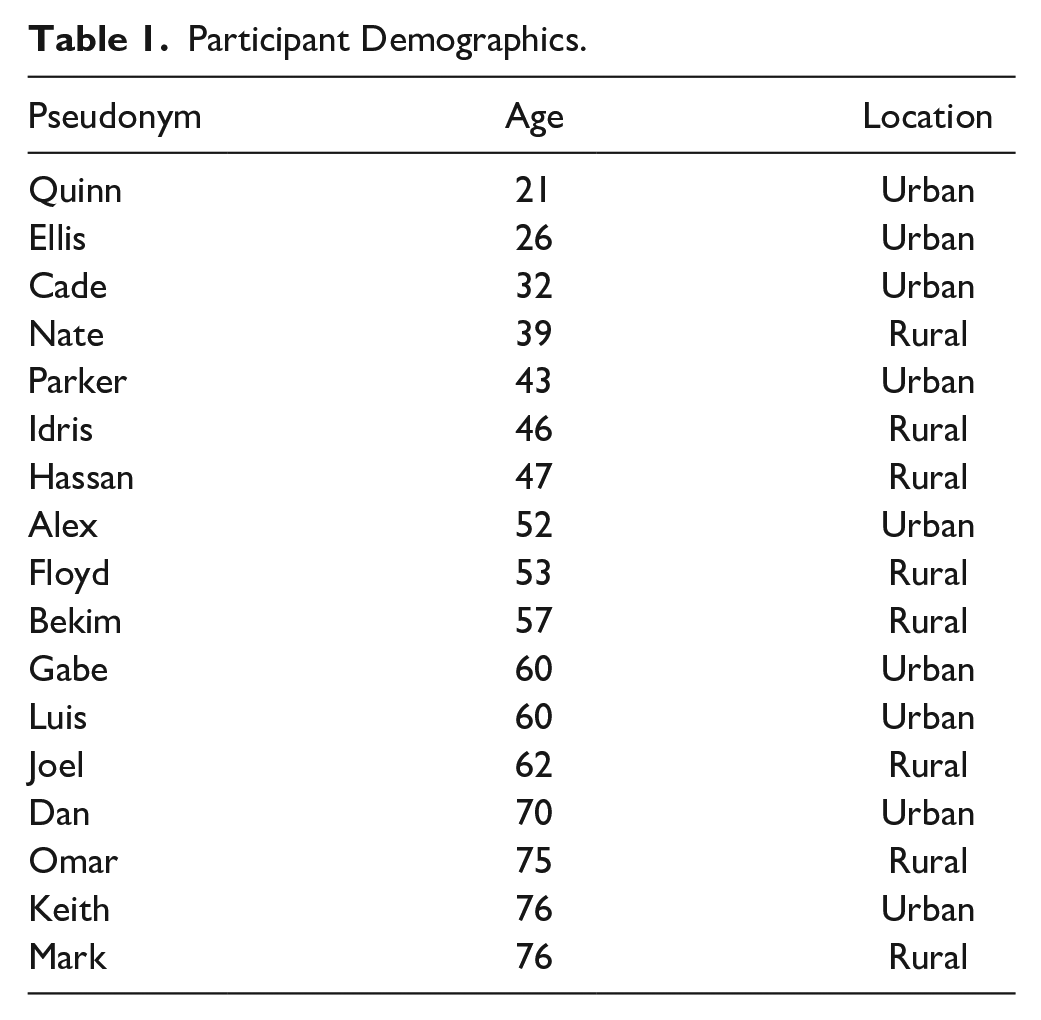
All 17 interviews were conducted via videoconference and lasted between 16 and 62 minutes (mean = 36.3 minutes). Participants’ ages ranged from 21 to 76 years (mean = 52.6 years; Table 1). Nine (53%) participants resided in an urban region.
Participant Demographics.
Themes
Participants described their engagement with general practice in five sub-themes: reasons for engagement, seeking validation, importance of relationships, interpersonal communication, and barriers to engagement.
Reasons for engagement
For most participants, attendance at their general practice was event-focused. In particular, attendances were driven by the need for prescription medication. Keith described how “obviously if one’s prescription’s run out, you need to go and get renewed scripts, but if I’m well, I might not go for a year or so.” Likewise, Luis indicated that “. . .apart from the COVID jab, [visits have] only been for repeat prescriptions.”
However, a few participants spoke of engaging with general practice for preventive care, such as sexual health and skin checks.
I go to the GP twice a year for routine things, and then after that, on an ad hoc basis like a new sexual partner and when I want to get a clear check there, and your typical general practice questions. So yeah, cold, flu, stomach bug and when I need a doctor’s certificate, that kind of thing. (Cade)
Additionally, other participants highlighted incidental care they sought secondary to their initial reason for attending the practice. Dan indicated that “it was time to get sun cancers burnt off again, and I get my bloods and blood pressure checked when I go to get the sun cancers done.” Similarly, although attending for a prescription renewal, Hassan noted that “while I’m here, might as well do my blood pressure and give me a script to get bloods taken.”
Seeking validation
While all participants expressed willingness to engage with general practice, they also discussed the need for validation and a preference for searching for health advice before seeking healthcare. Several participants described a need to justify or legitimize a health concern through discussions with significant others before seeing the GP.
. . .probably talk to (partner), and she’s like, ‘well maybe go see the GP’, and then I’d make an appointment with the doctor. (Floyd) I’d probably chat to my mum about it because she’s pretty good about that kind of stuff and knows what’s going on. (Quinn) “Kids will say, ‘Go and see the doctor dad”, And when I’ve been to the doctor, I’ll say, “By the way, I got my bloods back, it’s all good.” (Dan)
Beyond speaking with others, some participants discussed strategies they implemented to understand their own health concerns before talking with a health professional. The Internet was commonly referred to as a source of health advice, Dan explained “I googled it and diagnosed it myself, and then googled what exercises to do to repair that particular muscle.” Similarly, Joel described how “I do my own research on certain things first. I did my Dr Google research, and she (GP) used her years at university.”
Other participants referred to seeking advice from a family member and trialing advice found on the Internet to see if it works before making an appointment at the general practice for professional health advice.
I Google. . . I can’t remember the specific names of any websites, but medical websites not like Facebook or anything like that. . . . probably give it about three days and if it’s not starting to feel better that’s when I’ll go and see a GP. (Quinn)
Importance of relationships
All participants described their engagement with general practice in terms of the importance of relationships. While most participants identified a preferred GP, they also expressed a connection to the broader practice. A trusting relationship was described as an important consideration that impacted engagement.
I have a connection with my standard GP. But I know if he’s not available there are others in that practice that I could go to that I trust. (Alex) . . .we lived there for about 26 years, and I had the same practice. . . I chose the GP there, well initially. . . . you’re assigned to a particular GP, but then there were a couple there with whom I developed a pretty good relationship. . . I guess I went to them because I had respect and trust for their diagnostic abilities. (Keith)
However, some participants highlighted the importance of a personal connection with a specific GP.
I do have a regular GP. Reason I go to see her is she’s always done right by me and knows my history and she’s very approachable and yes, she’s certainly an asset for my life. (Idris) you’d be more comfortable with someone you’ve seen multiple times before; you have a feel for them and stuff like that; you’ve got that sort of developing interpersonal relationship. (Ellis) I know they’ve got all your records in front of them but the doctor actually knowing you as a person rather than just looking at whatever sort of symptoms you’ve presented with, makes a big difference! (Luis)
Interpersonal communication
Participants discussed communication from 2 perspectives: that of the participants, and GPs. Most participants described themselves as being proactive in raising health concerns and asking questions of their GP. Gabe explained: “I don’t leave until I’ve voiced my concerns.”
Several participants spoke of how they recognized from experience that they needed to be active in driving conversations rather than being passive recipients of care.
my past experiences have been a huge factor in recognising that I need to be the one that has to initiate a lot of the conversation. Sometimes you have to be the one to initiate the conversation, and to be able to say what is on your mind. I mean previously and historically, I never would have done that, but I’ve now learned from mistakes of the past. So I do that differently now. (Cade) I sort of drive the conversation. I guess when I’ve been there, I’ve been very forthright and asked questions and I’ve got suitable answers. (Parker)
This level of engagement extended to how participants felt about raising a sensitive or personal health concern with a GP.
As you get a bit older, you realise that doctors have sort of seen it and heard it all before, so there’s no point in the grand scheme of things, there’s no point in shying away from it, if it’s concerning you, it’s better to get it out and sort of talk about it than let it fester. (Luis) I’m easy and a little bit of embarrassment is nothing compared to the other alternatives. (Hassan)
When participants discussed communication from the GP, it was evident that many valued a sincere and direct approach from their GP in communicating health advice.
. . .we speak plainly to one another. I work for an emergency organisation. So I would rather that he said, ‘you’re, pardon the language; you’re a fat fxxk and you need to move’. His directness works for me. (Alex)
Poor communication skills or a disingenuous attitude from the GP negatively impacted the relationship between participants and their GP. Dan often felt his GP, “ wasn’t really interested,” and when Ellis requested a “general blood test,” the GP was “. . .angry at the idea of sending me for one, his demeanour changed, tone of voice, words used.” Bekim described how this kind of attitude made him feel;
. . .when you think about it, you’re actually sharing some pretty private stuff with somebody, and if you are just not heard, that makes a big difference doesn’t it, bedside manner is huge.
Barriers to engagement
Participants described various barriers to engaging with general practice, including difficulties with making appointments and issues with cost. Obtaining a timely appointment promptly was a key challenge.
It’s very difficult to access a GP locally if sick. You’ve got to know that you’re going to be sick about two or three months in advance. (Joel) If I needed to see (GP) today, I wouldn’t get in to see him for 2 weeks. (Alex)
Others highlighted the inconvenience of waiting for long periods in the practice to see the GP.
I hate to wait –it’s a barrier. I’ll ring to make an appointment, I’ll say, ‘can I have the first one after lunch,’ because I know there won’t be a backlog in front of me then. So I manage the annoyance myself. (Dan)
For some participants, the cost of attending general practice negatively impacted their engagement. Cade explained that “cost is an issue. I think medical care is a right for everybody. . .I definitely think cost is a big access barrier for me.” Similarly, Ellis referred to saving up his health concerns to ensure the visit was value for money. “I can’t go in and see him whenever I want or for a check-up or stuff like that. Unless I can rack up—like make the visit worthwhile.” Despite recognizing the potential importance of consulting a GP, to avoid the costs of general practice, some participants looked for other health services;
I don’t see why I’d go see a GP for 10 minutes just to look at a couple of moles. Sure, I understand that’s a life-saving appointment potentially. But at the same time, I’d probably find a Skin Cancer clinic or something like that, that is cheaper or free. (Ellis)
Whilst acknowledging that cost was a barrier to accessing healthcare, other participants, such as Luis, expressed that, “I’m not rich but if something’s got to get done, we will find the money to get it done.” Similarly, Omar felt that healthcare costs were justifiable because “I’m getting older, and I value my health.”
Discussion
This study explored men’s experiences of engagement with general practice and identified the reasons men engage and the facilitators and barriers to engagement. Participants identified that attendance at their general practice was generally event-focused. Furthermore, participants described seeking validation before engaging with general practice, seeking advice from family, and via the Internet. Participants identified the importance of having an established relationship with a GP/general practice. A relationship built on trust positively impacts healthcare engagement, which is a key finding of this study. Most participants were proactive in addressing health concerns with their GP, and many valued a sincere and direct approach by their GP when communicating health advice. Lastly, timely access, protracted waiting periods within the practice and cost were identified as barriers to engagement.
Participants spoke highly of having a regular GP or general practice and how continuity, familiarity, and trust in the person/team positively impacted their engagement. The relational continuity within general practice supports the delivery of person-centered care. 24 Relational continuity is a tenet of a well-balanced healthcare system and is highly valued by both patients, 25 and healthcare professionals. 26 Continuity of care with a regular healthcare provider has been shown to improve health outcomes, 27 increase preventive care delivery, 26 and trust in the healthcare provider, 28 and is associated with reduced healthcare expenditure. 29
This study demonstrated that participants favoured a GP who adopted a direct approach to communication and highlighted how a GPs’ interpersonal communication skills significantly impacted the therapeutic relationship. This is supported by literature that highlights men highly value healthcare professionals who communicate in an authentic and direct manner.30,31 The impact of masculinity on men’s interactions with general practice has been previously identified.8,32 Men’s masculine identities are adaptable to the environments in which they find themselves, including healthcare. 30 Skilled healthcare providers competent in adapting to the communication nuances of gender, including addressing their own gender bias, reduce communication barriers and help to forge a deeper therapeutic relationship with the men for whom they provide care. 30 When GPs exhibit ineffective communication and patients do not feel heard or validated, the ability of the patient to convey pertinent health information is impacted, and trust in the GP is lost.28,33 Supporting GPs with ongoing education and building on communication skills through a gender-focused lens will assist in upholding and strengthening patient-centered healthcare.
Participants sought advice from loved ones or the Internet before seeking general practice care. Social influences play a significant role in help-seeking. 34 Men, in particular, often opt for a period of self-monitoring and delay seeking professional healthcare advice. 35 Sources of social influences impacting help-seeking and engagement include family and friends but also increasingly include the Internet and social media. 34 Help-seeking and subsequent healthcare access of males is facilitated by advice, support, and the encouragement of family and friends. 36 Additionally, accessing the Internet for health advice assists in decision-making and can lead to an enhanced interactional role with the healthcare provider, enhancing communication, and shared decision-making. 37 Social networks could be better used to disseminate quality health information to enhance self-management and positive engagement with the healthcare system.
This study confirmed that access and cost impacted men’s engagement with general practice. Barriers such as cost and access issues may result in men either forgoing medical care, 14 or accessing alternate healthcare providers (eg, pharmacies, free clinics). Men’s challenges in accessing an appointment with a healthcare provider have been previously identified.8,38 For men, timely access is impacted by the service’s limited availability of appointments and inflexible scheduling of appointments within “traditional” working hours.39,40 Additionally, having to pay an out-of-pocket cost impacts healthcare engagement.40 -42 Indeed, the cost of accessing general practice was a reason for some to attend alternative free services and access the healthcare they needed. 42 This highlights the role of policy in equitable access to care. Delays in accessibility have an immediate impact and may also deter attendance for future healthcare consultations. 38 When men have to seek out an alternate healthcare provider due to access and/or cost implications, continuity of care may be negatively impacted, resulting in fragmented care. 43 While it may be argued that fragmented care is better than no care, the loss of continuity with general practice has broader implications. These include less coordinated preventive care and loss of oversight of the person’s healthcare as care is undertaken in various settings. 43 Increasing Medicare coverage may, in some part, reduce affordability barriers and support equitable access to primary care. 15 Strengthening general practice to effectively serve the community, support timely access to holistic healthcare, facilitate continuity, and reduce the impact of fragmented care is urgently needed.
Implications for Research and/or Practice
The findings from this study highlight that more can be done to improve men’s engagement with general practice. There is a need for practices and GPs to consider how they approach men’s healthcare. This should include consideration of communication strategies, continuity of care, and access to practice services that can be tailored to specifically meet men’s needs. Reducing the barriers and promoting the facilitators identified in this study can improve the quality of care. Closer connections between men and general practice have the potential to enhance preventive screening, promote early intervention, and improve health outcomes. Supporting significant others and community initiatives to provide positive health messaging to men is also a key strategy to ensure that men receive good health advice when they seek this outside the health system. Further research into the impact of gender on help-seeking and engagement is required. The need to adopt gender-sensitive approaches to providing care is paramount. This is particularly important to ensure that healthcare professionals are gender responsive and deliver truly patient-centered care.
Strengths and Limitations
While this study explored the views of men drawn from a single organization, participants were both employees and volunteers working in a range of capacities. The inclusion of men from diverse socio-economic and educational backgrounds from both urban and rural areas meant that the sample was broadly representative of the Australian population. Conducting interviews via videoconference ensured that visual cues could be observed and facilitated participation regardless of participant location. It was also easier to fit into busy schedules than face-to-face interviews.
Conclusion
Men value having continuity of care with a GP/practice team that they trust and have a relationship with. By supporting general practice to provide continuity of care, men’s therapeutic relationship with GPs/practice teams may be strengthened, and this will support and enhance health and well-being through timely intervention and truly patient-centered healthcare.
Footnotes
Acknowledgements
We would like to sincerely thank the NSW RFS for their support and encouragement in undertaking this project. We are sincerely grateful to the men who agreed to be interviewed and were generous in their time and their significant contribution to this project.
Author Contributions
RM: Conceptualization, Formal analysis, Methodology, Writing—original draft, and Writing—review & editing. CP, GM, and EH: Supervision, Conceptualization, Methodology, and Writing—review & editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received no specific grant. Ruth Mursa was supported by an Australian Postgraduate Award from the University of Wollongong.
Ethical Approval
The Human Research Ethics Committee of the University of the University of Wollongong (Approval no 2022/225) and the NSW RFS approved the study. All participants provided informed consent and were advised that they could stop the interview at any time. Pseudonyms are used to protect confidentiality.
Patient and Public Involvement
Members of the RFS contributed to the design and pilot testing of both the survey tool and interview questions.
Data Availability Statement
No data are available. No data are publicly available.