
Abstract
Gender-responsive healthcare is critical to advancing men’s health given that masculinities intersect with other social determinants to impact help-seeking, engagement with primary healthcare, and patient outcomes. A scoping review was undertaken with the aim to synthesize gender-responsive approaches used by healthcare providers (HCPs) to engage men with primary healthcare. MEDLINE, PubMed, CINAHL, and PsycINFO databases were searched for articles published between 2000 and February 2024. Titles and abstracts for 15,659 citations were reviewed, and 97 articles met the inclusion criteria. Data were extracted and analyzed thematically. Thirty-three approaches were synthesized from across counseling/psychology, general practice, social work, nursing, psychiatry, pharmacy, and unspecified primary healthcare settings. These were organized into three interrelated themes: (a) tailoring communication to reach men; (b) purposefully structuring treatment to meet men’s health needs, and (c) centering the therapeutic alliance to retain men in care. Strength-based and asset-building approaches focused on reading and responding to a diversity of masculinities was reinforced across the three findings. While these approaches are recommended for the judicious integration into health practitioner education and practice, this review highlighted that the evidence remains underdeveloped, particularly for men who experience health inequities. Critical priorities for further research include intersectional considerations and operationalizing gender-responsive healthcare approaches for men and its outcomes, particularly at first point-of-contact encounters.
Globally, males are twice as likely to die prematurely than females, and those who are socially, economically, and geographically disadvantaged shoulder a disparate health burden (Baker & Shand, 2017; Dobson, 2006; Global Burden of Disease 2017 Disability-Adjusted Life Years & Health-Adjusted Life Expectancy Collaborators, 2018). While there have been health-promotion investments encouraging men to seek help over the past two decades (MacDonald et al., 2022; Robertson et al., 2013; Smith et al., 2018), there has not been an equivalent level of investment to structurally improve the accessibility and responsiveness of primary healthcare services for men. Men continue to fall through the cracks after they engage in healthcare because their interactions do not immediately meet their needs (Lefkowich et al., 2017; Seidler et al., 2020).
Gender is a social determinant of health that affects men, which has implications for health systems and service design (Hawkes & Buse, 2013). While masculinities vary, research consistently connects men’s conformity to traditional masculine norms to their poor engagement with healthcare, even when men seek professional help (Galdas et al., 2005; Mahalik et al., 2012; Seidler, Wilson, Kealy, et al., 2021). Men’s propensity for nondisclosure, rationality, objectivity, and the need for control in healthcare encounters are offered as explanatory notes for men’s reticence to “being” helped (Noone & Stephens, 2008; Seidler et al., 2019; Tremblay & L’Heureux, 2005). However, research has pointed to a need to adapt our primary healthcare services to be more engaging for men, rather than place all the onus on individual men to seek out and connect with “foreign” healthcare services (Seidler, Rice, Oliffe, et al., 2018). Notably, traditional masculine norms can challenge practitioner applications of person-centered care, within primary healthcare settings, that aim to establish connection, trust, and mutual understanding (Malcher, 2009; Novak et al., 2019). Person-centered care represents the core foundation of student and health professional education and practice competency standards (Dielissen et al., 2012; Gerteis et al., 1993; Gillon, 2008), yet this education is rarely delivered with necessary gender considerations.
Gender-responsive healthcare is idealized as purposefully responding to the depth and diversity of people’s gendered health and illness experiences to optimize their outcomes (World Health Organization [WHO], 2016). Gender-responsive healthcare also connects gender with other social determinants to tailor services to address social inequities (Manandhar et al., 2018). Notwithstanding the critical need to invest in gender-responsive healthcare for women (Hay et al., 2019; McGregor et al., 2019), developing a gender lens for men’s health is key to improving boys’ and men’s engagement and retention in and outcomes of health (Bedi & Richards, 2011; de Oliveira et al., 2015; Hawkes et al., 2020; The Lancet, 2019). Mainstreaming gender-responsive healthcare for men through workforce upskilling might usefully reframe what is currently a sub-specialty as a core competency for all healthcare practitioners (HCPs).
These somewhat lofty hopes can be advanced with a review of the current knowledge regarding HCP approaches that lead to effective engagement with men across primary healthcare settings. While such a review has been previously undertaken, this was limited to healthcare settings where men underwent psychological treatment (Seidler, Rice, Ogrodniczuk, et al., 2018). In this previous review, tailoring language, clarifying treatment structure, and building a therapeutic alliance were considered key practices. The aim of this study therefore was to undertake a scoping review to integrate and synthesize the literature on approaches to engaging with men used by HCPs across a range of primary healthcare settings.
Methods
Protocol and Registration
The review and reporting methodology followed the recommendations of Peters et al. (2020) and the PRISMA extension for scoping reviews (PRISMA-ScR) reporting framework (Tricco et al., 2018). Each of the five incremental steps in the scoping review framework of Arksey and O’Malley (2005) was also followed. First, the research question for the review was identified, followed by the relevant studies for the review being identified. Next, the eligible studies were selected, with the data from those studies extracted, charted, and tabled. Finally, the results were collated, summarized, and reported.
The research question developed to guide the review was: What are the key approaches for engaging men during primary healthcare encounters? Primary healthcare settings were defined as healthcare settings provided as part of national health systems that are the first level of contact for individuals and families (WHO, 2023). Healthcare delivered through community-based health-promotion programs was excluded. A healthcare encounter was defined as a formal interaction between a man (as a patient/client) and an HCP, be it a dyadic, couple, or group-based encounter, in a healthcare setting.
HCPs included medical doctors, nurses, and allied health practitioners, including social workers, psychologists, and pharmacists, as well as students and trainees working in direct contact with patients/clients. Engagement was defined as the “processes of building the capacity of patients, as well as healthcare providers, to facilitate and support the active involvement of patients in the care process, to enhance safety, quality, and people-centeredness of healthcare service delivery” (WHO, 2016). As per the definition adopted by Seidler, Rice, Ogrodniczuk, et al. (2018), the care process refers to variables clinically relevant to the interactions between the man and the HCP. These include (a) attitudes, behaviors, and experiences of men; (b) attitudes, beliefs, and behaviors of HCP (therapeutic stance); (c) the nature of the dyadic interaction (therapeutic alliance); and (d) the treatment environment and atmosphere. The protocol was registered prospectively with the Open Science Framework on February 8, 2023 (https://doi.org/10.17605/OSF.IO/85WPG).
Eligibility Criteria
Article inclusion criteria were (a) focus predominantly or entirely on adolescent and/or adult men, (b) study sample including men, HCPs, an expert, or an expert panel; (c) encounters or interactions involving men in primary healthcare settings; (d) peer-reviewed published journal articles of primary (original) research, case studies, reviews, commentaries, or opinion pieces or editorials; (e) published in English language; and (f) published from 2000 to February 2024.
Information Sources and Search
The search strategies were initially prepared by the authors and conferred with an experienced university-based librarian and further refined through team discussion. Articles were identified through four electronic databases (OVID Medline, CINAHL, EMCARE, and APA PsychINFO). A search strategy was iteratively devised for use with Medline and the syntax adapted for the other databases. Both MeSH thesaurus terms and free text words were used. Additional articles included were extracted from the reference lists of identified articles or those recommended by expert colleagues. The final search strategy for Medline is provided in Supplemental Tables 1 and 2.
Selection of Sources of Evidence
Search outputs were imported into Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia, available at www.covidence.org), and duplicates were removed. Two researchers independently screened titles and abstracts and selected articles based on study eligibility criteria. Dual screening was performed on 30% of articles initially, and having achieved less than 5% disagreement on screening decisions, single reviewer screening proceeded thereafter. Discordant screens were resolved by consensus with a third reviewer. For the second stage of the review, full texts of the selected articles were assessed for eligibility by two reviewers and checked for accuracy by a third reviewer.
Data Charting and Items
The extracted data for charting included author(s), year, location of study, study design and type of evidence, and primary healthcare setting and primary health discipline (Table 1). The study population characteristics (sample size, average age, sub-population group), theoretical orientation of intervention (where applicable), and recommended engagement strategies/practices were also extracted. To understand nuances in approaches for different settings, articles were further categorized according to whether they described engagement with men in long-format healthcare encounters, typically occurring in dedicated mental health (counseling/psychology, psychiatry) and social work settings, or typically short-format encounters, namely medicine, nursing, pharmacy, and paramedicine settings (e.g., general practice or pharmacy consultations). Seven articles that could not be categorized were excluded from this sub-analysis (Table 1).
Summary of Included Articles

Note. NS = nonspecific.
Synthesis of Results
Given the review scope and objective, an inductive thematic synthesis (Braun & Clarke, 2021) guided the analyses. Inductive derivation of codes was guided by a previous scoping review (Seidler, Rice, Ogrodniczuk, et al., 2018) in distilling and discussing key themes and approaches. Using NVivo (Version 12; 2018) to organize the data, thematic synthesis was undertaken to identify recurrent and unique themes. For this, two researchers read and annotated all articles, coding for common content relating to distinct engagement approaches with male patients (or clients). The coded approaches were then iteratively grouped to themes based on their overall focus (e.g., practitioner insight) or robustness of the results. The coding was reviewed by a third independent researcher, and changes were discussed to reach consensus. The coded results were tabulated, and a conceptual categorization of engagement approaches was then derived and presented with illustrative examples.
Results
The search strategy generated 15,639 references (Figure 1), and 20 references from other sources (reference lists of selected articles and colleague recommendations) were selected. Following removal of duplicates and abstract screening, 171 articles underwent assessment of the full text, resulting in 97 eligible articles for review (Figure 1 and Table 2).

PRISMA Flowchart
Key Characteristics of Included Articles (N = 97)
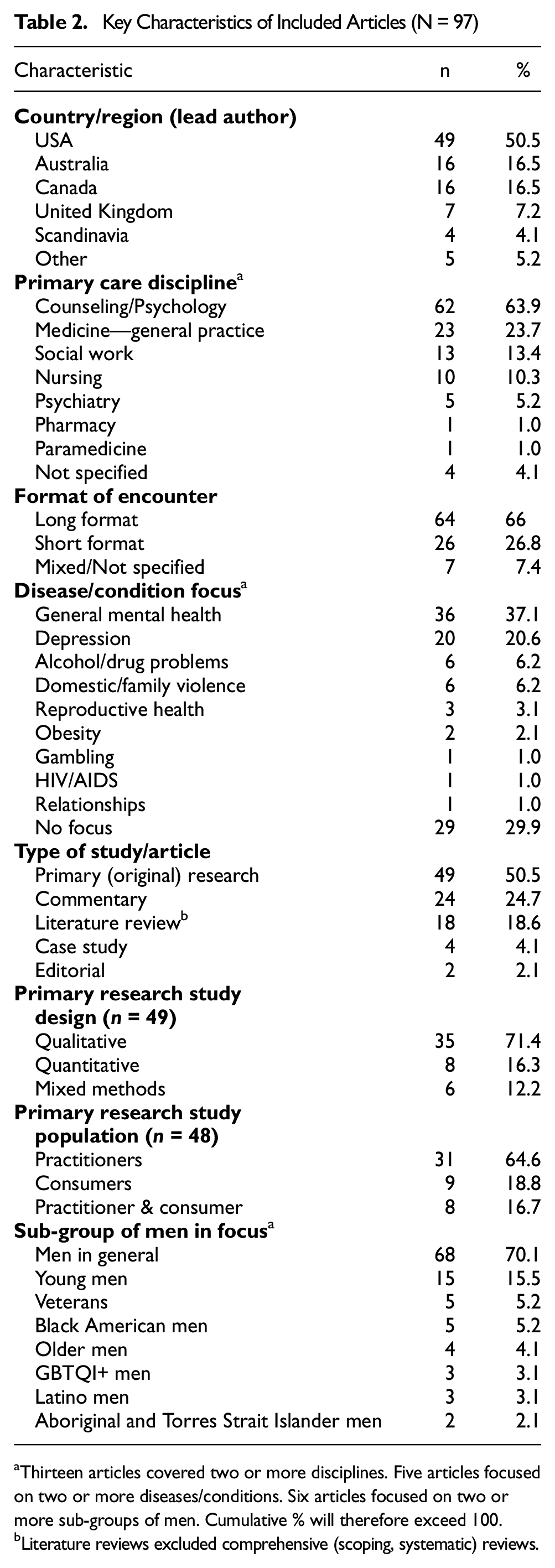
aThirteen articles covered two or more disciplines. Five articles focused on two or more diseases/conditions. Six articles focused on two or more sub-groups of men. Cumulative % will therefore exceed 100.
Literature reviews excluded comprehensive (scoping, systematic) reviews.
Article Characteristics
Year, Author, and Origin of Studies
The included articles (n = 97) were published between 2000 and 2024 and included 88 unique first authors. Half of the studies (n = 49; 50.5%) were from the United States of America (Table 2).
Article and Study Type
Forty-eight articles (49.5%) were categorized as a commentary, review, case study, or editorial. Of the 49 studies reporting primary data, 35 (71.4%) used qualitative methods, and eight (16.3%) used quantitative methods.
Sample and Participant Characteristics
Empirical studies reported data from 1,559 boys and men (patients/clients) and 1,276 HCPs. Sample sizes ranged from 1 to 475. Sixty-two articles (63.9%) were from counseling/psychology settings. Sixty-four (66%) articles focused on healthcare settings with typically long-format (namely counseling/psychology, psychiatry and social work) encounters. Thirty-seven (38.1%) studies were focused on a specific male sub-group, the largest cohort being young men (15.5%).
Synthesis of Evidence
In the 97 articles, 33 approaches were offered for engaging men in primary healthcare encounters (Table 3). The approaches were coded and are detailed in three themes: (a) the tailoring of communication to reach men, (b) purposefully structuring treatment to respond to men, and (c) the centering of the therapeutic alliance to retain men in care. The key approaches for each theme are described in the following part. Concordance or differences in the approaches extracted for typically long-format encounters and short-format encounters are also summarized.
Synthesized Engagement Approaches by Theme and (Typical) Format of Encounter

Long-format articles were classified as articles from disciplines of counseling/psychology, psychiatry, and social work. Short-format articles were classified as articles from disciplines of medicine, nursing, pharmacy, and paramedicine. This classification excludes seven articles that could not be definitively categorized.
Theme 1: Tailoring of Communication to Reach Men
Nine engagement approaches themed under the tailoring of communication to reach men, centered on the communication style used by the HCP during the primary healthcare encounter. Communication approaches were offered in 37 (57.8%) articles describing long-format encounters and 20 (76.9%) articles describing short-format encounters (Table 3). The use of informal language and encouraging and enabling men to tell their story and raising issues directly were the most common for both formats. Other language adaptations such as the use of metaphors and male-relevant language were more often approaches offered in the articles describing long-format encounters, whereas the use of informal language was more commonly referenced in articles describing short-format encounters.
The Use of Informal Language
The use of informal language, described in 26 articles (26.8%), served to enhance health messages and helped facilitate a perception of HCPs as “down to earth” (Madsen, 2015), with a “laidback and respectful manner” (Malcher, 2009). This builds trust and mutual respect and establishes a relaxed environment for interactions with men who may enter primary healthcare environments with uncertainty and/or discomfort. This also helps to alleviate men’s anxieties and reduce paternalistic healthcare dynamics or historical reticence around help-seeking.
Encourage and Enable Men to Tell Their Story
Approaches that encourage and enable men to tell their story (19 articles, 19.6%) included the use of explorative, open-ended questioning and avoiding checklist-style discussions. This aims to develop “a shared understanding by asking questions rather than dictating answers” (Marotti et al., 2020). It helps to convey a HCP’s genuine interest for the men’s life, to foster connection. Practitioners who “allow more opportunity to talk more about what else is happening in the man’s life” (Morgan, 2001) provide space for the whole man in the room and thus create more holistic healthcare encounters. This approach was also offered by Rosu et al. (2017) with the caveat of time permitting HCPs to do so.
Raise Issues Directly
Approaches that favored a “direct and matter of fact style communication” (Smith et al., 2008) style were typically mentioned when working with other men (18 articles, 18.6%). A focus on nonverbal communication was also mentioned as an approach for specific sub-groups of men (2, 2.1%). Malcher (2009) suggested this is important for HCPs working with men from First Nations in general practice, where a “less confronting, side-by-side communication with opportunities for silence and reflection” is favored over a direct approach to raising issues.
Additional Key Communication Approaches
Other approaches included the use of male-relevant language (14, 14.4%), including alternative labels for treatment or symptoms (12, 12.4%), culturally appropriate language (7, 7.2%), and metaphors (7, 7.2%). Metaphors may help bridge men’s everyday language to help them describe their symptoms and express their feelings (Dvorkin, 2015). The use of jargon may distance men, especially those who have limited health literacy. It is also important to “ensure information is understood” so as not to reinforce power dynamics (Farnbach et al., 2021). This is especially the case for men who may be living in marginalizing conditions. The integration of male-relevant language, “which respects, and in-part conforms, to masculine norms” (Seidler et al., 2019) was detailed as needing to ensure cultural responsiveness, recognizing the futility of an essentialist, one-size-fits-all approach to communicating with men.
Insights gained through storytelling and history taking can afford opportunities for gateway conversations (5, 5.2%) to elaborate other health or social welfare issues that might otherwise exist as peripheral and therefore redacted health concerns (e.g., violence, obesity, work-related matters). These conversations provide “a useful tool for interviewing men as it moves from areas of greater to lesser comfort” (Malcher, 2009).
Theme 2: Purposefully Structuring Treatment to Respond to Men
Eleven approaches that were grouped under purposely structuring treatment to respond to men centered on the key elements of healthcare optimally responding to men’s healthcare needs. Fifty-three (86.9%) articles from the literature describing long-format encounters offered one or more approaches in this theme. Approaches that were responsive to gender socialization, need for collaboration in care, and tapping into healthy masculinities were each offered in over 30% of these articles (Table 2). Eleven (47.8%) articles describing typically short-format encounters offered approaches in this theme.
Understanding the Influence of Gender Socialization
The most common approach offered (31 articles, 31.9%) in this theme was that HCPs understand the influence of gender socialization (i.e., adherence to masculine norms) on males’ health service access, symptom presentation, and interactions with HCPs. This includes understanding “the ways by which the traditional male gender role both inhibits and complicates” (Rabinowitz & Cochran, 2007) the expression of common conditions in men. With this, HCPs will in turn be better able to assess, diagnose, and tailor treatment. Rosu et al. (2017) described this as adopting a “masculinities” perspective that acknowledges the many and varied ways of being a man and responding to, and reducing, biases toward stereotyped masculinity. Practitioners should be sensitive to diversity including men “whose principles and expectations relating to masculinity and gender are less pronounced” as well as those who “strongly ascribe to hegemonic masculine principles” (Doherty et al., 2017).
Collaboratively Set Goals
In 25 (25.8%) articles, approaches recommended including men in the decision-making processes and collaboratively setting goals and expectations by “asking what the man wants to have accomplished in terms of success with respect to the challenges he identifies” (Blundo, 2010). This included establishing a shared understanding of roles and responsibilities with men so they “understand their role and are affirmed in their engagement, knowledge, and confidence to have and express opinions” (Rosu et al., 2017) regarding their care. Agreement in expectations can ensure men are across all key aspects of the healthcare process. This approach responds to men’s “need to have tailored and holistic plans” (Guilcher et al., 2016) facilitating autonomy and empowerment over what can be experienced as a passive treatment process.
Action-Oriented, Solution-Focused Treatment
Related to this, several articles (25, 25.8%) suggested being responsive to men’s preference to take control, act, and problem-solve. Action-oriented solution-focused treatment care can resonate more with men, with this framing of treatment “more likely to make clinically significant and reliable change” (Richards & Bedi, 2015). These approaches should also be accompanied by “periodically checking in with men about their preferences, goals, needs” (Kealy et al., 2021).
Allow for Flexibility, Timing, and Pace of Treatment
Orienting treatment around men’s needs includes allowing for flexibility of space, timing, and pace of treatment (18, 18.6%) around. “the content and focus of the contact.” This included more psychotherapy-specific approaches of allowing men the “choice of meeting places, duration or intensity” which can increase comfort and engagement (Kivari et al., 2018).
Additional Key Structural Approaches
By seeking opportunities to improve men’s health literacy throughout encounters (19, 19.6%) and transparently breaking down treatment options, structure, and direction (16, 16.5%), HCPs can “temper men’s expectations accordingly, thus engaging and empowering their client as an equal partner in treatment” (Seidler et al., 2020). Exploring roles and responsibilities in care (14, 14.4%) and helping men access and describe internal experiences (13, 13.4%) may assist in tapping into their needs, motivators, and preferences for “structure and a clear context” (Tremblay & L’Heureux, 2005) in healthcare. Finally, building a male-friendly space (9, 9.3%), a treatment feedback process (6, 6.2%), and employing masculine-sensitive assessment strategies were also noted as key factors in adapting treatment to respond to men (4, 4.1%).
Theme 3: Centering the Therapeutic Alliance to Retain Men in Care
The third theme “centering the therapeutic alliance to retain men in care” comprised 13 approaches. The majority of articles (98.4%) describing healthcare typically delivered through long-format encounters included one or more approaches synthesized to this theme (Table 3). This compared to 76.9% of articles describing settings with typically short-format encounters. Approaches that explored strengths and positives of men’s masculinities, promoted men’s autonomy, and validated their personal experience were regularly offered in the longer-format encounter articles. Listening with empathy, creating a nonjudgmental environment, conveying confidence, professional competencies, and confidentiality were more often focused on shorter-format encounter articles.
Explore Strength-Based Masculinities
Adopting a strength-based approach and leveraging masculinities when engaging with men in care were recommended in 43 (44.3%) articles. Juxtaposing men’s defeat, awkwardness, or “fear of femininity” (Kealy et al., 2021) during healthcare encounters with strength-based approaches lobbied HCPs to reinforce men’s masculine self-worth by “using solution-focused skills to pose constructive questions that elicit the man’s taking responsibility to make things better for himself and others” (Blundo, 2010). Transforming men’s vulnerabilities by affirming their help-seeking can be positioned as an “expansion of positive masculine qualities” (Kealy et al., 2021). Patel and Barnett (2011; pharmacy) also highlighted the importance of dispelling men’s concerns for burdening their HCP and/or taking up finite resources by reframing “complaining” as merely describing one’s experience. Normalizing universal statements such as “Many of my patients forget to . . .” were suggested as approaches to “remove the embarrassment often associated with certain feelings and experiences.” Indeed, normalizing certain experiences as common for men was noted in 31 (32%) articles as validating help-seeking as manly, particularly in mental health settings. Key strengths included promoting men’s autonomy over their health and establishing them as experts in their health and behavior change, described in 37 (38.1% articles). This affords men control during healthcare interactions and indeed the therapeutic alliance, to reinforce their “inner strength and ability to take ownership of their situations as an important driver of their journey to recovery” (Guilcher et al., 2016).
Accommodating Diversity and Debility
The intricate intersections between men’s masculine identities and other social determinants of health including “social class, race, sexual orientation, ability status, religion, and other salient identities and roles” (Englar-Carlson and Kiselica, 2013) diversely influence men’s health and illness behaviors. In 29 (29.9%) articles, the necessity to respond to the diversity within and between men, and accepting men’s socialized identities, was reinforced. The value of listening with empathy (25, 25.8%) and creating a nonjudgmental environment (18, 18.6%) was linked as an approach to affirm “the dignity of the client” (Guilcher et al., 2016) and de-stigmatize antisocial or risk-taking behaviors to aid men’s self-disclosures. González-Prendes (2007) highlighted the need to focus on “building the therapeutic alliance by demonstrating empathy through the acknowledgment of the difficulties that the clients had experienced,” and in doing so avoid hastening to “challenge clients’ cognitions.” Related to this, a philosophical bend for HCPs meeting men where they are at in their health needs was discussed in 26 (26.8%) articles. Such an approach allows “carefully monitoring the client’s cues regarding his comfort level with certain topics” (Kiselica, 2003).
Self-Reflect on Gender Socialization
In 25 (25.8%) articles, it was recommended HCPs self-reflect on their own gender socialization and resultant biases, “how masculinity and gender affect their conceptualisations of clients” (Marasco, 2018), and how that translates to their practices for engaging with men. Indeed, taking the first step by calling this out could break down barriers between practitioners and men, fostering deeper connections through shared experiences and understanding as “some male clients may look to see if the counselor will take the first risk and break the silence about socialisation” (Englar-Carlson & Shepard, 2005)
Build Collaborative Relationship
Twenty-two (22.7%) articles noted the value of purposefully establishing a collaborative relationship with men. As a specific example, Dvorkin (2015) described “mirroring” to provide men opportunity and space to reflect on their needs in the exchange: “Starting with the phrase ‘So, what I’m hearing you say is . . .’ and ending with ‘Did I get that right?’ allows men to step into a leadership position within the relationship.” This helps to equalize power dynamics between the HCP and client, overcoming any sense of defeat (and associated shame) men might experience in healthcare settings, and instead encourage active collaboration.
Additional Key Therapeutic Alliance Approaches
To further strengthen the therapeutic relationship with men particularly during initial encounters, conveying confidence and competency (11, 11.3%) with appropriate self-disclosure (13, 13.4%) to build trust and help “reduce the shame-based intensity of the encounter” (Rabinowitz & Cochran, 2007) was discussed. Approaches that reinforce confidentiality (13, 13.4%) especially if ailments are imbued with feelings of shame and vulnerability are important. Eight articles specifically called out the avoidance of HCPs challenging masculine norms. For example, by actively “avoiding language that is negative about masculinity” (Johnston et al., 2008), HCPs become “more likely to be able to form a successful working alliance with male clients” (Good et al., 2005).
Discussion
There has, to date, been an absence of a clear summation about the approaches used for engaging men in healthcare encounters across primary healthcare settings. This review provides a synthesis of the literature to describe 33 engagement approaches, informed by HCPs and male patients, the parts and sum of which may usefully guide HCPs to better reach, respond, and retain men in primary care. The approaches were grouped across three interrelated and coalescing themes (Figure 2). First, themed under tailoring of communication, was a range of suggested language adaptations to initially engage men and keep them connected throughout healthcare encounters. These included the use of accessible language and constructs to make space for men’s contextual stories and health practices. Second, approaches for purposefully structuring treatment detailed the necessity to integrate approaches that are strategically flexible, collaborative, action-oriented, and solution-focused to alleviate potential power imbalances in healthcare settings. Finally, the importance of centering the therapeutic alliance combined communicative and structural approaches, suggesting HCPs be receptive, affirming, and responsive to men’s patterned and diverse gendered help-seeking practices within primary healthcare contexts.

Key Elements of Gender-Responsive Approaches to Optimally Engaging Men During Healthcare Encounters
The approaches to engaging with men are offered for consideration with the caveat that the evidence is emergent, particularly in the noncounseling literature, which represented less than a quarter of the articles in the current review. This may account, in part, for their lack of translation into healthcare workforce education. A review of health and medical curricula of Australian Universities in 2022–2023 indicated that while men’s health was deemed important, communicating and engaging with men in practice was one of the least likely topics to be covered in curricula (Seidler et al., 2024). For practising HCPs, there is also little training about gender-responsive approaches (e.g., Osborne et al., 2018; Seidler et al., 2022).
The current review findings regarding communicative, structural, and relational (alliance) elements for primary HCPs align with three of the eight dimensions of person-centered care described by Gerteis et al. (1993): (a) respect for patient values, preferences, and expressed needs; (b) information and education; and (c) emotional support to relieve fear and anxiety. Moreover, offered here are gender-responsive specificities for those elements of person-centered care—making available key content and strategy for incorporating these results to inform education curricula and established practices, when providing primary care to men. Understanding men’s motivations and preferences for healthcare engagement in essence affords a much-needed tailoring for person-centered care. Highlighted herein is the fundamental need and ease for incorporating gender competencies as person-centered care for all HCPs (Dielissen et al., 2012).
The most striking difference between the approaches offered from the literature describing typically long-format versus short-format encounters was the greater focus in the long-format encounters on sensitivity and responsiveness to the gendered needs of men. Gender competencies of HCPs aims to strengthen the therapeutic alliance that is recognized as a pivotal predictor of engagement and treatment outcome in mental health contexts (D. J. Martin et al., 2000; Seidler et al., 2020). The importance of the therapeutic alliance extends to any HCP working with men. In contrast to long-form encounters, it could be suggested that time-restricted short-form encounters, such as during general practice or pharmacy consultations, may encumber the integration of what is being fast established as gender-responsive care. Yet these primary care settings are the first entry point to healthcare and preventive health for most men (Simons et al., 2023), and the implications of men’s poor engagement during primary healthcare encounters are stark. Gender-competent HCPs have heighted receptivity for discrete and nuanced gendered cues and symptoms in men’s presentations that may reside outside routine screens (Fisher et al., 2021; Rice et al., 2020). This will support gateway conversation approaches and male-sensitive assessment strategies, both noted in this review as important in first-line encounters with men. This is pertinent when considering men frequently present with physiological ailments in general practice that can obscure underlying chronic disease risk (Serefoglu et al., 2014), psychological distress, or suicide risk (Zajac et al., 2022). Up to 95.7% of men who die by suicide have contact with primary care in the year prior to their death (Laanani et al., 2020), highlighting the risk of missed diagnosis of depression in men (S. Martin et al., 2021). Legitimizing the therapeutic alliance with men at the healthcare entry point, through gender responsivity, aims to ensure value for men and confidently and successfully participate in healthcare (Lefkowich et al., 2017). Finding ways to practically embed gender competency into HCP training and practice should therefore be prioritized.
Many of the gender-responsive engagement approaches and “male-friendly” examples offered in the articles extracted within this review were typically emblematic of traditional masculinity as the singular lens to view and respond to men during their engagement with healthcare rather than it being a consideration. This was also identified by Zielke et al. (2023) in their review of the operationalisation of “masculinity” across gender-transformative health interventions. Gender is dynamic and modifiable, and this includes men’s masculine identities which will adapt to the different social environments including healthcare settings. By prioritizing engagement catered to diversity in and across men (Doherty et al., 2017), HCPs can help men with transformative masculinities to “legitimise help-seeking as the rational, courageous, and ‘manly’ course of action” (Carroll et al., 2020; Seidler et al., 2022). Such strength-based approach in health programming is increasingly being recognized as an essential ingredient in advancing men’s health equity (Galdas et al., 2023; Smith et al., 2020). In their efforts to promote men’s health, and by extension advance the wellbeing of their family and friends, students and HCPs should also be encouraged to address their own gender biases to ensure that these do not translate into practice and influence how they engage with men. Indeed, knowing one’s gender biases, anticipating male diversity, and where applicable, aiding transformative masculinity changes could all break down barriers between HCPs and men, fostering a deeper connection through shared experience and understanding.
Critically, this review reveals a dearth of studies focussed on engaging with men from diverse ethnic and racial backgrounds, who may have unique health beliefs and practices and social norms that influence their gender identities. This included a lack of global indigenous scholarship. This means research funders need to seek proposals that explicitly call for an examination of social determinants of health and health inequities, and researchers need to be explicit about examining intersectional factors when framing research questions. At the practitioner level, an increased uptake of evidence-based intersectional practices such as trauma-informed care, tailored to sub-populations of men, would be an example of translating this intersectional research into practice. This responds to the notion that men from minority cultures are typically socially conditioned to deny injury and/or isolate themselves to conceal their trauma (Affleck et al., 2022). Furthermore, intersectional practices such as this could be accompanied by a formal evaluation of outcomes, assessing whether these methods adequately fit or robustly fail. Resulting insights into the specificities for what works may offer some potential for transferability and translation to other local settings where primary healthcare systems have struggled to engage men. The sensitivities and nuances in approaches to engagement then need translation into HCP education, if we are to reduce health inequities (Baker & Shand, 2017; Zielke et al., 2023) experienced by the most marginalized and vulnerable groups of men globally.
For future translation of these review findings into practice, service delivery interventions could look similar to the “Men in Mind” gender competency-based training curricula, which was developed, in part, from the scoping review of approaches by Seidler, Rice, Ogrodniczuk, et al. (2018) for optimally engaging men in psychological treatment. This review informed the design of a world-first randomized controlled trial that validated the training for mental health professionals (Seidler et al., 2023). While developed for mental health service contexts, the core tenets of “Men in Mind” are likely relevant to all healthcare settings serving men and reflect many of the core findings of this review.
Given the small sample, analysis of the nuances in approaches used by non-counseling disciplines and health setting could not be undertaken. A further limitation of the review was that nearly one third of the articles were a commentary, case study, or editorial. While clinician insights and recommendations from the practice interface are important, this may introduce opinion bias or limited viewpoints. A further caveat is that there remains a lack of rigorous research that has formally validated the efficacy of gender-responsive healthcare engagement approaches for men (Phillips et al., 2023; Smith et al., 2018).
This review excluded articles where healthcare was delivered as part of community-based health-promotion programs. Gender-responsive and transformative frameworks for engaging men within these public health settings have however been previously synthesized (Galdas et al., 2023; Robertson et al., 2016). There is considerable alignment of approaches to those offered herein. These include framing delivery to tap into and inspects masculine ideals (e.g., self-reliance), reinforcing healthy diverse masculinities, being direct and using informal communication styles (e.g., avoiding jargon, use of colloquial language). These are all caveated with the need to apply approaches judiciously so as not to reinforce potentially harmful gender stereotypes. This creates efficiencies for the creation of education curricula that has interdisciplinary reach across the healthcare professions included in this review and beyond. This includes in specialist care settings where similar approaches have been called for to optimize the healthcare provision and outcomes for men. Examples include when communicating with men about active surveillance (Mróz et al., 2013) and when supporting men in care after a diagnosis of male-factor infertility (Obst et al., 2023).
Conclusion
The findings of this review, while warranting further applied research, offer practice considerations for HCPs that may improve men’s engagement during primary healthcare encounters. Moreover, they continue an important lobby for the tailoring of person-centered primary healthcare tenets to advance men’s health. Building and translating evidence-based approaches into student and HCP education is critical, and these andragogical investments need to be concurrent with adjusting broader primary healthcare structures to ensure a sustained focus on addressing men’s health inequities.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883241241090 – Supplemental material for Approaches to Engaging Men During Primary Healthcare Encounters: A scoping review
Supplemental material, sj-docx-1-jmh-10.1177_15579883241241090 for Approaches to Engaging Men During Primary Healthcare Encounters: A scoping review by Zac E. Seidler, Ruben Benakovic, Michael J. Wilson, Margaret A. McGee, Krista Fisher, James A. Smith, John L. Oliffe and Michelle Sheldrake in American Journal of Men's Health
Footnotes
Acknowledgements
The authors acknowledge the significant expertise and support of Professor Jacqui Macdonald in providing input on the design of the literature search strategy used for this study. The authors also acknowledge the members of the Movember Men’s Health Education Project Working Group, who provided clinical and sector expertise and insights to inform the direction of the review, and University Librarian, Vikki Langton, for the technical support for the development of the databases search strategies.
Authors’ Contributions
All authors contributed to the conceptualization and study design, with ZES responsible for funding acquisition, and ZES, JLO, and JAS providing supervision. Articles were reviewed, extracted, and coded by MS, MAM, and ZES and thematically analyzed by RB, MJW, KF, and ZES. The original draft manuscript was prepared by MAM, RB, KF, and MJW, with ZES, MS, JLO, and JAS involved in the reviewing and editing process. ZES, JLO, and MJW provided clinical and public health practice insights. All authors read and approved the final manuscript and met ICJME criteria for authorship.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Australian Government Department of Health (ID: HEALTH/ 21-22/D21-5427311) and Movember (Australia)
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.