
Abstract
Aim:
To investigate the detection and initial management of first psychotic episodes, as well as established schizophrenia, within the primary care of the Andalusian Health System.
Background:
Delay in detecting and treating psychosis is associated with slower recovery, higher relapse risk, and poorer long-term outcomes. Often, psychotic episodes go unnoticed for years before a diagnosis is established. Primary care physicians are crucial for early recognition of psychosis and schizophrenia, especially in Spain, where primary care is the main entry point to healthcare services.
Methods:
Cross-sectional exploratory study. All active primary care physicians in the Malaga Guadalhorce Health District were invited to participate. Due to the COVID-19 pandemic, the survey was conducted online. The survey, adapted and validated for the local context, included 22 items and 5 sociodemographic questions covering early detection, treatment options, physical health monitoring, and management challenges. Descriptive and bivariate analyses summarized the data and explored correlations between key variables.
Findings:
The study included 142 primary care physicians (response rate 35.5%), with 28.9% men and 71.1% women, primarily from urban areas (83.1%). Most had completed residency training (86.6%), with 79.6% receiving psychiatric training. However, only 5.6% had participated in training sessions in the last 5 years, with all such sessions lasting less than 30 h. Physicians typically managed 0-10 patients with diagnosed schizophrenia and saw these patients 2 to 3 times annually. They often felt capable of managing these patients, especially with mental health consultancy support. Physical health monitoring was common, though some relied on mental health services to do this. Collaboration with mental health services was moderate, with high utility perceived for having a list of patients with severe mental disorders in their care panel.
Conclusions:
Family physicians are generally confident in managing psychosis and schizophrenia but lack recent specialized training. Mental health consultancy services are valued, but collaboration with these services needs improvement. Clear guidelines and enhanced training are essential to ensure comprehensive care, addressing both mental and physical health needs of these patients.
Introduction
Delay in detecting and treating psychosis is associated with slower and/or less complete recovery, higher risk of relapse, and poorer outcomes in subsequent years.1 –3 Sometimes, individuals experience psychotic episodes for many years that go unnoticed before a diagnosis is established. 4 In this context, Primary Care Practitioners (PCPs) play a crucial role as they can achieve higher rates of early recognition of psychosis and schizophrenia,5,6 particularly in countries like Spain where the healthcare system places primary care as the gateway to receiving healthcare services. 7
In Spain, the prevalence of schizophrenia spectrum disorders (SD) is approximately 6.2 per 1000 individuals, with a higher prevalence observed in men compared to women. The incidence rate (IR) for individuals aged 15 to 34 years is 50.25 per 100 000 person-years, also higher in men. These findings highlight the significant burden of schizophrenia on the Spanish healthcare system, necessitating comprehensive strategies for early detection and management in primary care settings. 8
Early intervention extends beyond the need to reduce complications related to the disorder itself, but also addresses the additional need to mitigate other physical and psychological complications. 9 Both psychosis and schizophrenia are strongly linked to poor physical health, 10 resulting in a reduced life expectancy over 15 years, regarding the general population (worse for men). 11 While approximately one-fifth of premature deaths among individuals with schizophrenia are due to suicides and accidents, the majority stem from physical illnesses,11,12 notably cardiovascular disorders, metabolic conditions like diabetes mellitus, chronic obstructive pulmonary disease, and certain cancers and infectious diseases such as HIV, hepatitis C (HCV), and tuberculosis.12,13
In part, the physical deterioration observed can indeed be explained by the nature of the disorder and the side effects of pharmacologic treatment. 14 However, there is evidence suggesting that inadequate healthcare organization, physician attitudes, and the social stigma associated with schizophrenia patients also contribute significantly to this decline.15,16 A clear example is the low detection rate of diabetes mellitus in this population, despite its high prevalence17,18 as well as the underdiagnosis of cardiovascular diseases 12 , cancer, 19 and HCV. 20
In this context, the role of primary care in monitoring the physical health of individuals with psychosis and schizophrenia becomes crucial for improving their quality of life and life expectancy. Therefore, national and international clinical practice guidelines urge greater efforts in detecting and treating physical illnesses associated with psychosis and schizophrenia.21 –23
Previous studies in other European countries have addressed early detection of psychosis and physical health monitoring in primary care settings (eg, Gavin et al 24 ; Le Galudec et al 25 ; Simon et al26,27; Stip et al 28 ; Verdoux et al 29 ). The findings indicate that, among psychotic symptoms, PCPs more easily identify prominent symptoms such as hallucinations, delusions, and bizarre behavior.26,29 These studies also reveal considerable variability in how primary care professionals approach individuals with psychosis and schizophrenia.24,26
In Southern Spain, specifically in Andalusia, the healthcare system is organized to address the most prevalent and severe diseases and disorders through Integrated Care Processes (PAI). These processes offer treatment pathways supported by the best available scientific evidence at any given time, aiming to ensure continuity of care and reduce variability in clinical practice. 30 However, the implementation of PAIs has been uneven, 31 and given the seriousness and prevalence of severe mental disorders, updating these processes is necessary. In this regard, several studies have been conducted to incorporate user demands, values, and preferences32,33 into the public healthcare system, as well as to analyze barriers and facilitators for implementing evidence-based recommendations.34 -36
Guidelines recommend distinct approaches for managing psychosis and established schizophrenia in primary care. For psychosis, the role of the PCP is to detect the condition and refer the patient urgently to mental health services, especially in acute situations such as agitation. Medication is not required at this stage; prompt referral is the key intervention.21,22
For established schizophrenia, if clinical stabilization is achieved, the monitoring of the patient’s physical health transitions to the PCP after the first year. During the initial year, all healthcare responsibilities lie with mental health services, primarily due to safety protocols for medications, which necessitate frequent (sometimes weekly) blood tests during the first few months. During psychopathological exacerbations, the responsibility for physical health monitoring reverts to mental health services until clinical stabilization is regained.21,22,37
Additionally, there are cases where long-stabilized patients prefer to discontinue visits to mental health services and opt for follow-up care by their PCP, akin to other stabilized chronic medical conditions. Guidelines support this approach if it aligns with the patient’s preference.
The current project aims to contribute to this comprehensive analysis by exploring the current approach to psychosis and schizophrenia in primary care, focusing on early detection of cases and monitoring physical health. Since in Spain, there is a lack of current data on these issues, the objective of this study is to investigate the detection and initial management of first psychotic episodes, as well as established schizophrenia, within the primary care of the Andalusian Health System. To achieve this, the study explored the healthcare burden related to patients with psychotic disorders or schizophrenia, the approach, attitudes, and needs of family doctors, how assessments are conducted, and the type of management offered for handling these conditions.
Methods
Design
This is a cross-sectional exploratory study designed to answer the following research question: How are psychosis and schizophrenia managed in primary care services?
Participants
All PCPs from health centers under the Malaga Guadalhorce Health District were invited to participate in the study. This amounts to a total of 33 health centers and 400 family doctors (varying depending on affiliation/employment).
As an inclusion criterion, family doctors had to be actively practicing at the moment of the survey. Those physicians who were on sick leave or any other cause for leave or were not formally enrolled in the staff were excluded.
Instruments
A modified version of the IGPS questionnaire 26 was used for data collection. This questionnaire includes 22 items and 5 sociodemographic questions, covering the number of patients in the early stages of schizophrenia attended by the physician (whether already diagnosed or diagnosed by the GP); treatment options; detection and treatment of early psychosis; treatment and prognosis of schizophrenia; and the value of treatment.
The instrument was subject to a translation process by 2 independent translators. Next, to obtain a culturally valid version in Spanish language, the translated version was reviewed by a panel of experts, including a family doctor, a psychiatrist, a clinical psychologist, a mental health nurse, and a research methodology expert, to refine the translation and adjust cultural aspects to fit the Andalusian health system. Some questions were removed for being irrelevant, and others were rephrased to be more understandable in our context. This revised draft was further reviewed by another group of 5 psychologists to identify and amend any potentially stigmatizing or offensive language. This resulted in changes such as removing problematic behaviors and substituting “psychiatric care” with the more neutral “healthcare.”
Subsequently, the survey was subject to content validation by 2 procedures: 20 PCPs from the Malaga Guadalhorce District evaluated each question on a 4-point Likert scale for clarity and relevance. No changes were necessary as the questions were deemed clear and appropriate by the majority. Subsequently, a content validity analysis was conducted with a panel of 6 experts (3 active family doctors and 3 doctors with dual specialties in family medicine and psychiatry). They assessed the relevance of each item on a 4-point Likert scale, and the Content Validity Index (CVI) was calculated for each item. One item with a CVI below 0.78 was removed following cognitive interviews with the experts to understand their disagreement. After the removal, the survey achieved a high CVI of 0.96.
For the questions specifically evaluating the degree of collaboration with mental health services, satisfaction with this collaboration, and the usefulness of having a list of patients within their primary care panel diagnosed with severe mental disorders (including psychosis and schizophrenia), a 5-point Likert scale was used. This scale ranged from 1 (very dissatisfied/very low) to 5 (very satisfied/very high).
Procedure
The survey was initially planned to be performed in a face-to-face format, although due to the onset of the COVID-19 pandemic and subsequent lockdowns, it was conducted online via an electronic form.
Analysis
Descriptive statistics were employed to summarize the survey data. Measures of central tendency (mean, median) or frequencies were used, depending on the nature of the data. This provided an overview of key metrics, including the number of patients with diagnosed schizophrenia, the frequency of annual consultations, consultation times, and the difficulties faced in patient management. Additionally, the analysis examined the physical health monitoring practices for patients with psychosis, the willingness of physicians to assume treatment responsibilities upon patient request, and the existence and satisfaction with mental health consultancy services within their centers.
Bivariate analyses were conducted to identify correlations between variables. For instance, the relationship between consultation frequency and management difficulties, and the influence of mental health consultancy availability on the physicians’ willingness to manage psychosis treatment, were examined.
Ethical Aspects
Informed consent was obtained from the participants before administering the mentioned survey. Participants were previously informed in writing about the study’s objectives and characteristics. The study was conducted according to national and international guidelines (Declaration of Helsinki and Tokyo). The study protocol was evaluated by the Provincial Ethics Committee of Malaga. The general database was stored with a password and kept on a secured, locked device. Once the data were extracted, they were processed anonymously and used solely for the study’s objectives. The confidentiality of the subjects included in the study was ensured in accordance with the Spanish legislation.
Results
Sociodemographic Characteristics of Participants
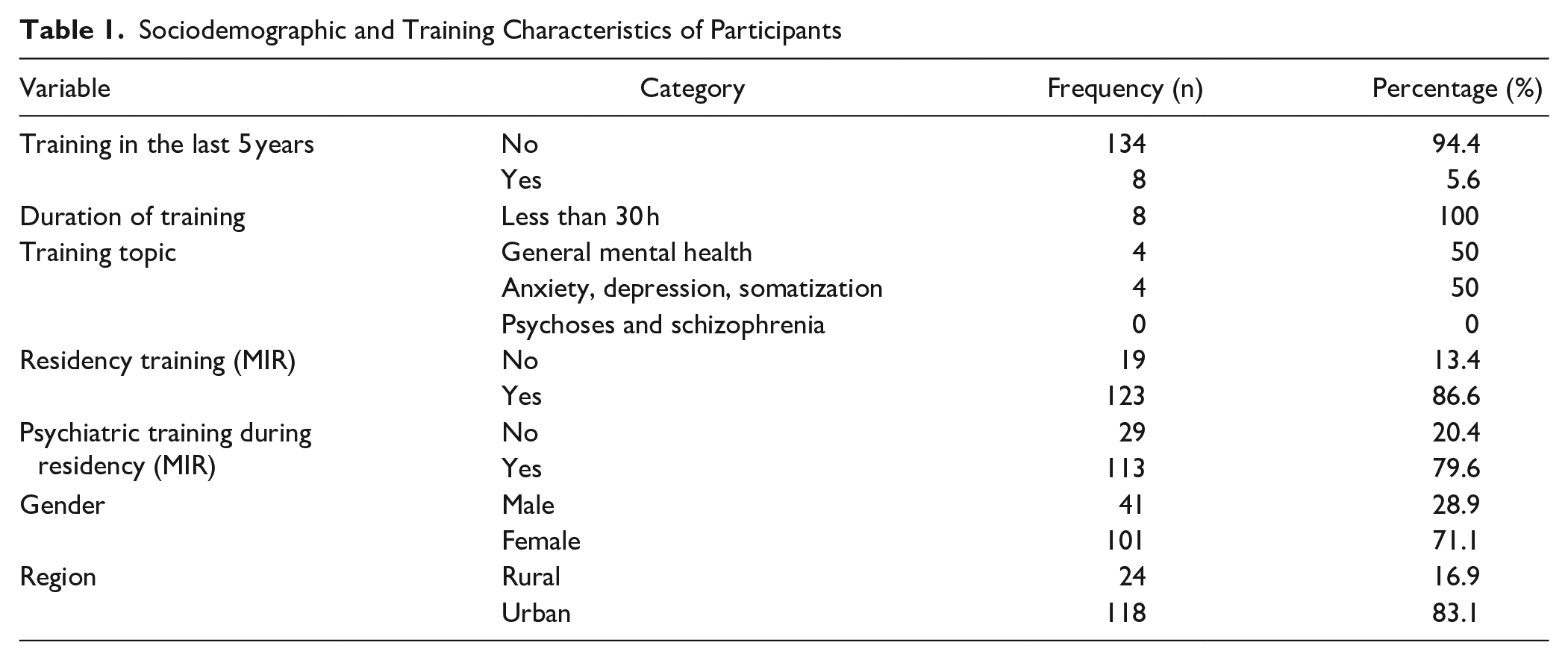
The study included 142 PCPs (response rate 35.5%), with a gender distribution of 28.9% men and 71.1% women. The participants were from various areas, with 16.9% practicing in rural areas and 83.1% in urban areas. Regarding professional training, 86.6% had completed their 4-year residency training (MIR), and 79.6% reported having received psychiatric training during their residency. However, only 5.6% had participated in training sessions in the last 5 years, with all such sessions lasting less than 30 h. The main topics of these trainings were general mental health (50%) and anxiety, depression, and somatization (50%; see Table 1).
Sociodemographic and Training Characteristics of Participants
Clinical and Management Practices
General information on the treatment of schizophrenia
The number of patients with schizophrenia managed by each family doctor and the frequency and intensity of the visits was very variable. So, most PCPs reported managing between 0 and 10 patients diagnosed with schizophrenia, and they typically saw these patients between 2 and 3 times per year. Regarding consultation time, 66.9% of PCPs spent the same amount of time on consultations with schizophrenia patients as with other patients, while 33.1% reported spending more time.
On average, PCPs were responsible for the psychiatric treatment of 2.64 stable patients with an initial diagnosis of psychosis. The main reason for taking charge of treatment included patients being stable and not requiring intensive follow-up. Moreover, most PCPs (81.7%) expressed a willingness to assume treatment responsibilities at the patient’s request, particularly with mental health consultancy support (65.5%), while others preferred to refer patients to a community mental health center (18.3%). Specifically physical health monitoring of psychosis patients was a common practice, with 59.9% of PCPs monitoring physical health of 0-10 patients. Nevertheless, 19.0% of PCPs did not perform physical health monitoring because mental health services were responsible.
Regarding difficulties in patient management, 16.2% of PCPs reported no difficulties. However, among those who felt capable of managing these patients (85.2%), almost half of the PCPs expressed a preference for no follow-up in their primary care consultation. Mental health consultancy services were available in 45.8% of the centers, which likely contributed to the moderate degree of collaboration with mental health services (Mean = 3.28, SD = 1.05) and the similar level of satisfaction with this collaboration (Mean = 3.29, SD = 1.10). Furthermore, the usefulness of having a list of patients within their primary care panel diagnosed with severe mental disorders, including psychosis and schizophrenia, was rated with high values (Mean = 4.00, SD = 1.05l; see Table 2).
General Information on the Treatment of Schizophrenia.

Rated on a scale of 1 to 5, with higher scores indicating a greater degree of agreement or satisfaction.
Specific information on the detection and treatment of the first psychotic episode
The second part of the questionnaire focused on specific information regarding the detection and treatment of a first psychotic episode, including 10 targeted questions. This section aimed to gather detailed insights into PCPs’ experiences and practices related to early identification and intervention for psychosis.
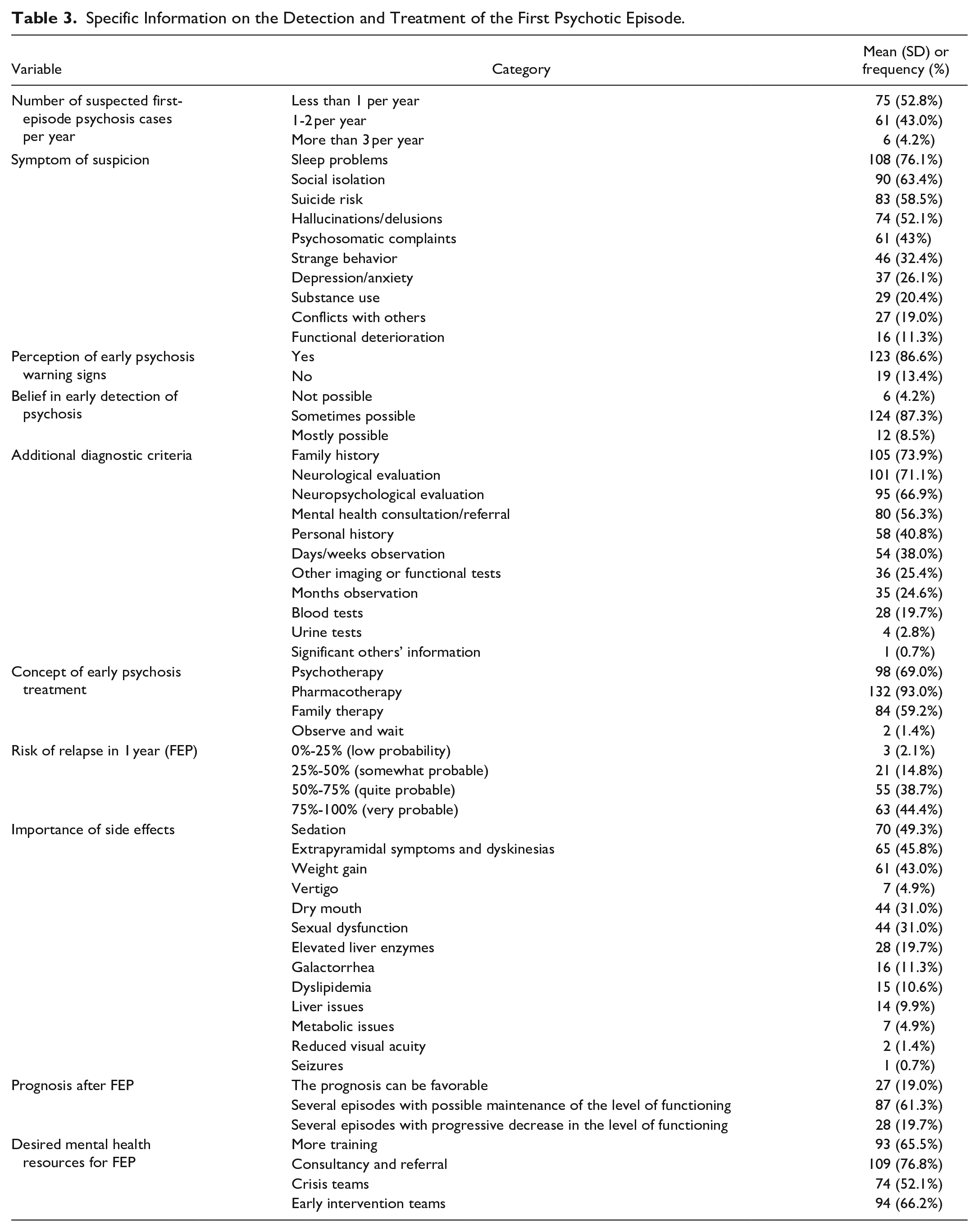
PCPs reported encountering suspected first-episode psychosis cases at varying frequencies, with just 4.2% encountering more than 3 cases annually. The most common symptoms prompting suspicion included sleep problems (76.1%), social isolation (63.4%), hallucinations or delusions (52.1%), and suicide risk (58.5%). Indeed, most PCPs (86.6%) recognized early warning signs of psychosis. The symptoms detected less frequently included anxiety and depression (26.1%), substance abuse (20.4%), and functional deterioration (11.3%). Furthermore, 87.3% believed that early detection of schizophrenia is sometimes possible.
In terms of diagnostic and treatment practices, 73.9% of PCPs considered family history, 71.1% utilized neurological evaluations, and 66.9% employed neuropsychological evaluations for diagnosis, such as the Mini-Mental State Examination (MMSE). Additional diagnostic criteria included personal history (40.8%), observation over days or weeks (38.0%), and consultations with mental health professionals (56.3%) as the most frequent practices. When treating early psychosis, 93.0% of PCPs favored pharmacotherapy. PCPs were asked to select the 2 most important side effects of antipsychotic treatment based on their experience. The most frequently chosen side effects were sedation (49.3%), weight gain (43.0%), and extrapyramidal symptoms or dyskinesias (45.8%). Less frequently selected side effects included vertigo (4.9%), reduced visual acuity (1.4%), seizures (0.7%), and metabolic issues (4.9%).
Regarding prognosis after a first episode of schizophrenia, 61.3% of PCPs believed patients would generally experience several episodes but maintain their level of functioning. Conversely, 19.0% were optimistic about a single episode with maintained functioning, while another 19.7% expected several episodes with a progressive decline in functioning. PCPs also estimated the risk of relapse within 1 year without treatment as either quite probable (50%-75%) or very probable (75%-100%).
Desired mental health resources for early psychosis included consultancy and referral services (76.8%), early intervention teams (66.2%), and more training (65.5%). Crisis teams were also identified as beneficial by 52.1% of the respondents (see Table 3).
Specific Information on the Detection and Treatment of the First Psychotic Episode.
Bivariate Analysis
The bivariate analysis explored several relationships between the PCPs’ profile, consultation characteristics, collaboration with mental health services, beliefs, needs for training, and the frequency of suspected first-episode psychosis (FEP) cases.
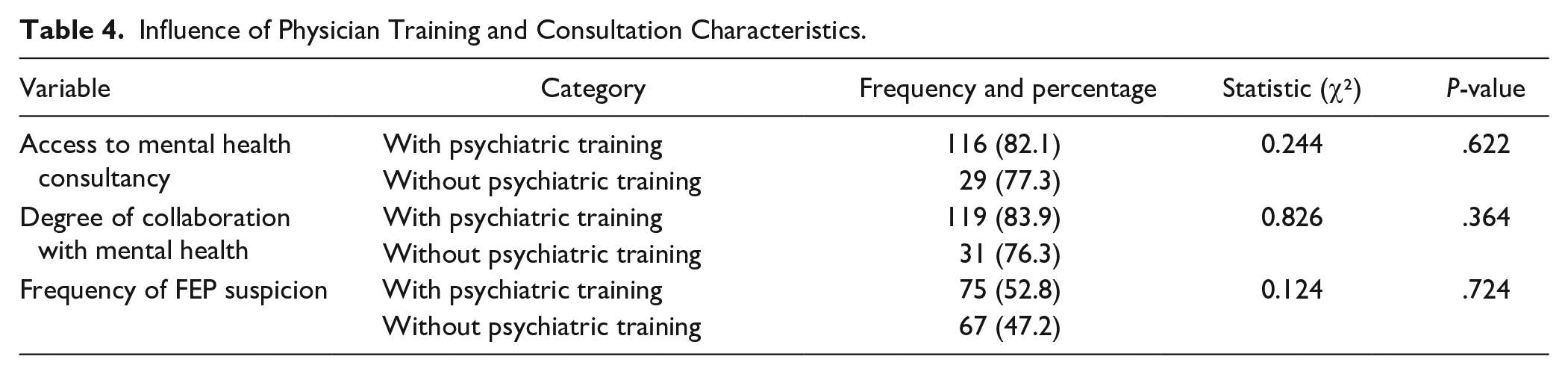
Firstly, findings showed that PCPs with psychiatric training during their residency (MIR) were more likely to have access to mental health consultancy services (82.1% vs. 77.3%) and showed higher rates of collaboration with mental health services (83.9% vs. 76.3%), although these differences were not statistically significant (P = .622 and .364, respectively). No significant difference was found in the frequency of FEP suspicion between those with and without psychiatric training (P = .724; see Table 4).
Influence of Physician Training and Consultation Characteristics.
Secondly, regarding the existence of consultancy services and collaboration, a significant relationship was found between the existence of consultancy services and the degree of collaboration with mental health services (χ² = 14.5, P < .001). PCPs with consultancy services reported more frequent collaboration. Satisfaction with the collaboration was also significantly higher among those with consultancy services (χ² = 86.5, P < .001).
However, the existence of consultancy services did not significantly influence the number of patients managed or the frequency of consultations (P = .998 and .895, respectively). Similarly, no significant differences were observed in the number of stable patients under treatment based on the presence of consultancy services (P = .591; see Table 5).
Impact of Mental Health Consultancy Services on Clinical Management Variables.

When exploring beliefs and perceptions, results showed that PCPs who perceived early psychosis warning signs were more likely to believe in the possibility of early detection of psychosis (χ² = 16.7, P < .001). Those with psychiatric training during their residency were more likely to believe in early detection (χ² = 8.00, P = .018; see Table 6).
Beliefs and Perceptions about Early Detection in Psychoses.

Lastly, the collaboration with mental health services and the training needs were explored, along with their impact on patient outcomes. The analysis showed that 63.4% of PCPs with a high degree of collaboration perceived a need for more training. Regarding the prognosis after the first episode, 56.3% of those PCPs who believed in early detection reported a positive prognosis compared to 43.7% who did not. However, none of these results were statistically significant. The perceived risk of relapse in 1 year for untreated patients was 57.7% for those with a high degree of collaboration versus 42.3% with a low degree (P = .050). Additionally, 59.9% of PCPs with longer consultation times perceived a higher risk of relapse compared to 40.1% with shorter consultation times (P = .082; see Table 7).
Relationship Between Collaboration, Expressed Training Needs and Some Beliefs.

Discussion
The objective of this study was to investigate the detection, management, and overall healthcare burden related to psychotic disorders and schizophrenia in the primary care system of the Andalusian Health Service. This included an exploration of both the initial management of first psychotic episodes and the long-term care of patients with established schizophrenia. In the case of first episodes, suspected psychosis is involved, so a formal diagnosis is not required, but an evaluation by the primary care physician (PCP) is necessary. In the second case, we are referring to patients with an already established diagnosis of schizophrenia, mostly individuals who have been under the care of mental health services for several years and have been diagnosed by specialists. The study aimed to explore the healthcare burden associated with patients with psychotic disorders or schizophrenia, the approaches, attitudes, and needs of family doctors, including how assessments are conducted, the types of management offered, and the collaboration with mental health services.
In the first place, regarding diagnosis, our results show that only around 25% of PCPs consider depression and anxiety as possible symptoms of a psychotic episode, a significantly lower figure compared to other countries. In previous studies this percentage ranges from 37% to 70% depending on the country. 27 This phenomenon is also observed in France, where 31.5% of PCPs identified anxiety and depression disorders in patients with suspected psychosis, 25 highlighting the difficulties in differential diagnosis between psychotic disorders and mood disorders. During the prodromal phase of psychosis, dysphoric symptoms and signs such as fatigue, depression, anxiety, irritability, or sleep problems predominate. 38 Although the latter are well identified as warning signs in our study, the dysphoric symptoms, despite being non-specific and having lower predictive value, are the most frequent in the early stages. 39
In contrast, the detection of suicidality in our study is remarkably high, with 58% of PCPs identifying suicide risk. Considering that the presence of suicidal ideation in early psychosis is 40% 40 this result suggests the advisability of adopting a cautious approach when treating the patient, which will presumably aid in the detection of suicidal risk. This contrasts significantly with data from other countries, which reported a range of 5% to 23%.25,27 This difference may be attributed to a more defensive healthcare approach in our context, as PCPs are more inclined to follow guidelines and best practices, not only for their clinical efficacy but also to reduce the risk of legal complaints and professional liability. 41 Nevertheless, the prevalence of suicidal ideation in early psychosis has been reported to be 40%, 40 often coexisting with a high comorbidity of severe depression (nearly 50%). 42
The findings highlighted that PCPs play a crucial role in managing patients with schizophrenia and psychosis, despite encountering challenges in patient management. The study revealed variations in the frequency of suspected first-episode psychosis cases and identified common symptoms that prompt suspicion. It also underscored the importance of physical health monitoring and the willingness of PCPs to assume treatment responsibilities, 43 particularly with mental health consultancy support. This study highlights that, while PCPs play a crucial role in managing both the mental and physical health of patients with psychosis and schizophrenia, challenges remain, particularly in terms of clearly defining responsibilities for physical health management. This uncertainty can lead to PCPs assuming that psychiatrists are addressing these needs, and vice versa, leading to gaps in care. Improved dissemination of guidelines and enhanced collaboration between PCPs and mental health professionals are essential to ensure that both mental and physical health aspects are comprehensively managed. 44 Indeed, patients have reported this lack of coordination between PCPs and mental health professionals. Additionally, the difficulties some patients face in navigating the healthcare system can exacerbate this issue.43,44 These factors combined may lead to the inadequate physical health care highlighted in various studies, emphasizing the need for clear guidelines and improved communication between primary care and mental health services to ensure comprehensive care for psychiatric patients. 45
Addressing the gaps identified in the study is likely to lead to improved health outcomes for these vulnerable populations. Enhanced communication and well-defined guidelines between primary care and mental health services are expected to result in better care for patients with severe mental disorders. Collaborative care models have a strong background in mental health treatments in PHC. 46 Despite the fact that more complex patients require additional specialized services, many ingredients of these models may contribute to improving provision of care for people with psychosis.
Additionally, the study examined the collaboration with mental health services and the perceived need for more training among PCPs. While the study found trends in these areas, it noted that further research is needed to draw definitive conclusions. In our findings the existence of consultancy services was highly valued by PCPs, although no significant differences were found regarding the burden of patients and the frequency of consultations. Nevertheless, current evidence has not confirmed if collaborative care is more effective than standard care in patient outcomes such as quality of life, mental state, or psychiatric admissions. 47 More high-quality experimental research should be necessary to elucidate the ingredients of this complex intervention that contribute to better outcomes. The existence of consulting services in our findings (45.8%) is higher than those reported in other studies. 48 However, it should be noted that the consulting service available in Primary Care with Mental Health is of a general nature, not only for cases of first episodes of psychosis, which means this finding should be interpreted with caution.
It is notable that PCPs with higher collaboration with mental health services report greater training needs. This aligns with the percentage of PCPs with recent mental health training, which is strikingly low compared to other countries (here 5.6%; in France, 10.4%; in Switzerland, 17.1%).25,26 Notably, in the present study the questionnaire inquired about any training in mental health topics, whereas in other countries, the focus was specifically on courses about psychosis and schizophrenia. As a result of adapting the survey to the Andalusian context, the question was modified to include any training in mental health topics. Had this adjustment not been made, a floor effect would have occurred, with the percentage not even reaching 1%. This significant difference in continuous training across countries underscores the disparity and the need for more extensive mental health education.
It has been reported that PCPs may refrain from seeking mental health consultancy because their lack of knowledge about resources and how to access them. 49 Educational interventions for PCPs have shown a positive impact on first-episode psychosis referrals. 50 It would be necessary to determine if extending training to different profiles of PCPs would have the same impact on managing patients with psychosis.
Finally, the appropriateness of referring patients with a first episode of psychosis must also be considered, especially if such referrals are excessively delayed due to factors beyond the PCP’s control, such as accessibility to specialized services and the perceived stigma by patients and their families. 49 Moreover, the existence of different models of health service organization, depending on the prominence given to Primary Care and the threshold for secondary mental health services, may also influence this outcome. 51
Limitations
The response rate was moderate, although higher than that reported in other similar studies.25,29 One consequence of this, as highlighted by some studies, is that it is unclear whether the profiles of responding and non-responding PCPs are the same. It is assumed that those who respond are PCPs with a special interest in mental health, which may compromise the representativeness of the sample. 25 The period when the survey was carried out could contribute to this fact, since the COVID19 pandemic was at its worst period.
We must not rule out the non-response bias, which could have presented a more optimistic view of the management of patients with psychosis in Primary Care than if those professionals with little interest in mental health had responded.
For all these reasons, we consider it necessary to conduct further studies that use strategies to involve a greater percentage of PCPs.
Another limitation to note is that the population of patients identified with a diagnosis of schizophrenia or psychosis is not validated, as in the case of established psychosis, the diagnosis is either obtained from medical records or based on the assessment of the primary care physician (PCP), which might raise doubts about whether the patient population the PCPs are referring to is actually the one being asked about. In the case of first psychotic episodes, a diagnosis has not yet been established.
Conclusion
Family physicians feel confident in managing the detection and initial management of first psychotic episodes, as well as subjects with established schizophrenia. These patients are regularly attended in primary care centers. However, it is not common for PCPs to have up-to-date training in this area. The availability of mental health consultancy services is highly valued, although collaboration remains moderate.
Footnotes
Acknowledgements
We would like to thank all the PCPs of the Primary Care Health District of Malaga Guadalhorce for their participation during the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded in the 2018 Research Projects Funding Call in Primary Health Care by IBIMA Plataforma BIONAND (Spain) and the Málaga-Guadalhorce Health District (DSMG) with the DSMG 18-011 grant (Management of psychosis and schizophrenia in primary care). It was supported for open access charge by IBIMA Plataforma BIONAND (Spain) and the Spanish Institute of Nursing Research belonging to the Spanish General Council of Nursing.
Ethical Standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional guidelines on human experimentation, with the Helsinki Declaration of 1975, as revised in 2008, and the Spanish legislation on data confidentiality.
Informed Consent
Written informed consent was obtained from all subjects.