
Abstract
Introduction/Objectives:
To understand the impact of introducing Additional Roles Reimbursement Scheme (ARRS) on the General Practice Nurse (GPN) workforce. A workforce/people impact assessment designed as a cross-sectional survey of a stratified sample of 900 GPN on the Queen’s Nursing Institute mailing list.
Method:
A workforce/people impact assessment was designed based on the UKCS 2014 piloted and distributed as a cross-sectional survey via a survey platform. This included questions on level of impact, kind of impact and perception of prior engagement. Data were analyzed using descriptive statistics and content analysis.
Results:
The survey consisted of 21 questions (531 responses, response rate of 60%). ARRS deployment appears to have impacted the GPN workforce in several ways. There was positive impact on workloads from ARRS roles working in original scope, for example pharmacists medicine reviews. However, any benefit was offset by the increased workloads created by those new to general practice and/or working outside of traditional scope. This ranged from a lack of resources to provide the support those new to primary care require to practice safely, the expectations of others-that GPN will fill the gap in support and teaching to GPN directly safety netting the work of others. There was a lack of consultation regarding a major workforce change, leading to feelings of devaluation. There are some significant equity issues highlighted particularly around pay and opportunity.
Conclusion:
The introduction of ARRS has had some positive but mostly negative impact on the workload and introduced pay inequity issues on GPN.
Introduction
The attainment of national and global health goals can be achieved only with a health workforce that is adequate in number, distribution, skills, motivation, and performance. This has been formally recognised by the inclusion of a “health worker density and distribution” indicator within the monitoring framework for the sustainable development goals by the United Nations. 1
Change in the workplace affects the workforce. Major changes should be assessed for potential impact on the workforce. Such changes should not disadvantage the workforce in terms of investment, labor, and equality. 2 Workforce impact assessments (WIA) or people impact assessments (PIAs) can clarify the potential or actual impact of major changes on the workforce and act as a meaningful form of workforce engagement. 3 If done prospectively they are multidimensional and focus on engagement however they are either rarely used in healthcare or used partially or inconsistently. 4
A General Practice Nurse (GPN) is a registered nurse who works autonomously within a Multidisciplinary Team within General Practice (GP) surgeries as part of a Primary Healthcare Team. They screen and treat people of all ages, including babies, children and adults in addition to providing traditional aspects of nursing care such as wound care, immunizations, vaccinations, cervical cytology sampling, and ECGs. They hold clinics for patients with long term conditions such as asthma, heart disease and diabetes and run vaccination programmes. A key role of the GPN is to offer health promotion advice in areas such as contraception, weight loss and smoking cessation in addition to emphasis on promoting women’s and men’s health.
A key focus of their role in health promotion is to work with and enable patients to manage their health care needs. According to NHS Digital there are over 16,000 registered nurses, who deliver more than 6 million patient appointments per month in England within general practice. 5
In 2019 the Additional Roles and Reimbursement Scheme (ARRS) was introduced into general practice in the English NHS by Health Education England. The scheme funded the salaries and in some cases costs, of 17 types of workers to expand the primary care workforce which could be “chosen to meet the needs of local populations.” 6 These roles included care co-ordinators, pharmacists, paramedics, and associate professionals such as Nursing Associates, Physicians Associates, and their trainees. There has been a rapid expansion of new roles in general practice compared to GPs and GPNs 7 but little evaluation of the impact of this on the existing workforce.
It is unclear if any demand modelling was done for these types of workers labor but a review of the literature and exploration of the grey literature, (policy documents, commercial and third sector research, and other publications that were not peer reviewed papers) did not yield a WIA, PIA, or any modelling of labor demand for this initiative. The only WIA/PIAs that appear to be done in the NHS, if at all, are equality impact assessments. 8 The Queen’s Nursing Institute (QNI), the world’s oldest nursing charity which supports nursing in the community, received several anecdotal accounts of impact on the GPN workforce of the introduction of ARRS. This included issues such as pay inequity and increased workloads. To understand the impact of the introduction of a large-scale workforce policy change, the QNI conducted a retrospective workforce impact assessment survey on the GPN workforce. WIA or PIA are usually prospective but as the change has already taken place, there is an opportunity to explore how the introduction of ARRS has impacted and what levels of engagement around this change were perceived to be.
Methods
A WIA/PIA was designed based on the UKCS 2014 methodology, 3 piloted and distributed as a cross-sectional survey via a survey platform (SurveyMonkey). This included questions on level of impact, kind of impact and perception of prior engagement. This survey distribution was based on a stratified sample (GPNs) using a balanced allocation,9,10 sent by the QNI to 900 GPN via a dedicated mailing list in September 2023. Data were analysed using descriptive statistics and content analysis of free text.
Results
The survey consisted of 21 questions and resulted in 531 responses. This gives a response rate of 60%. The estimated completion rate was 76% to 100% but this included the final free text question.
Length of Time Working as GPN
Respondents were all working as GPN. The most common length of time working as a Registered Nurse (RN) in general practice was over 20 years (30.3% of respondents) with a further 15.3% between 16 and 20 years. 21.2% in total of respondents had been working for 5 years or less (Figure 1).
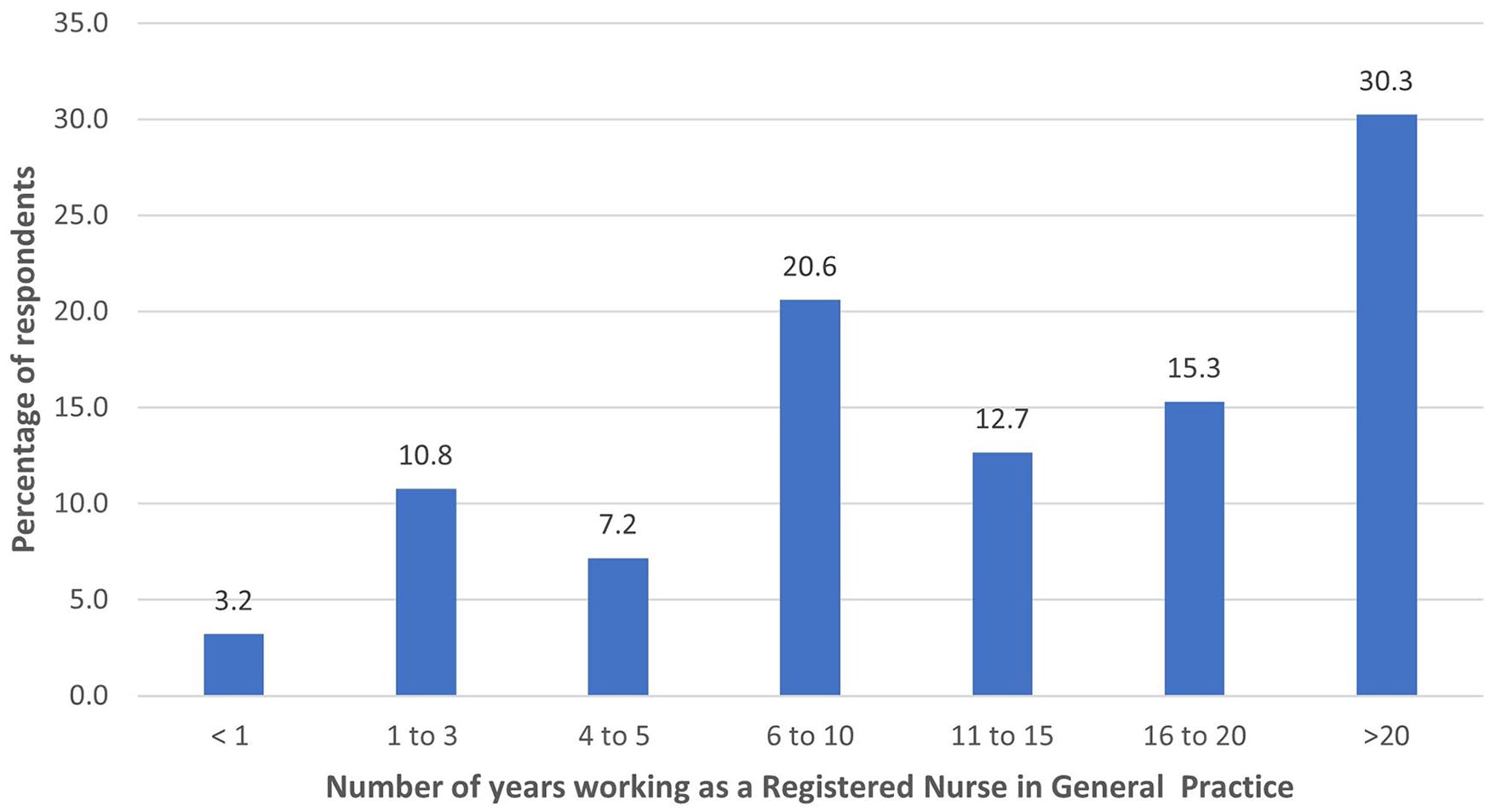
Respondents number of years working in general practice (n = −529).
Length of Time on the GMC Register
64.7% of respondents had been on the NMC Register for over 20 years with a further 10% for 16 to 20 years. In total 9.6% had been on the register for 5 years or less (Figure 2)

Respondents number of years on the NMC Register (n = 530).
Equivalent Agenda for Change Band
Respondents equivalent Agenda for Change Band is shown in Figure 3. 39.4% of respondents reported being on Band 6 or equivalent with 23.4% on Band 7.
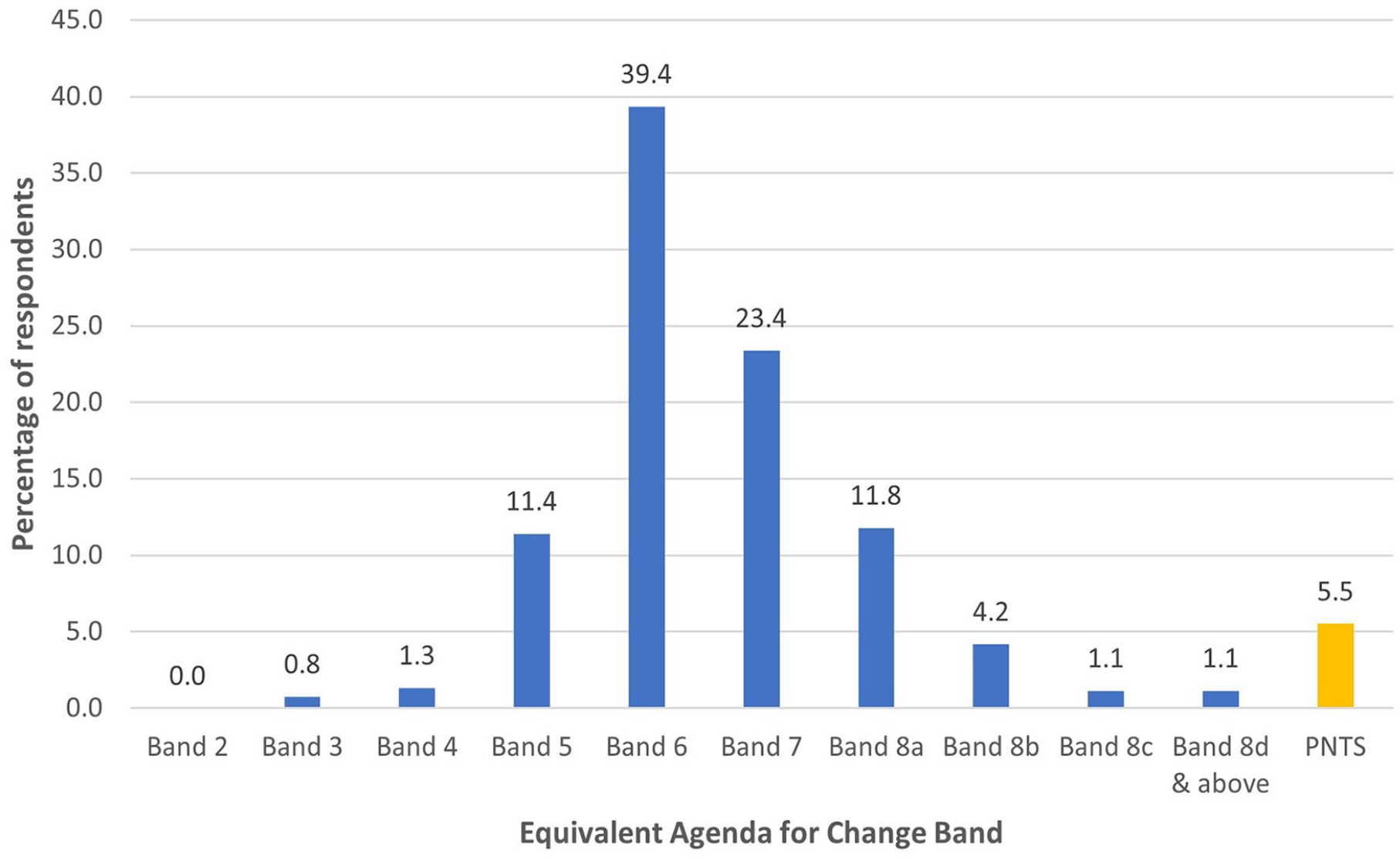
Respondents equivalent Agenda for change band (n = 526).
Consultation on the Introduction of ARRS Roles into Practice
11.8% of respondents reported that ARRS roles had been introduced into their practice before their employment. 12% of respondents agreed with the statement “I was consulted on the introduction of ARRS roles into the practice” while 76.2% disagreed (Figure 4).

Respondents opinion of the statement “I was consulted on the introduction of ARRS roles into the practice” (n = 530).
Deployment of ARRS Roles into Practice
In terms of ARRS roles deployed into their practice (Figure 5), the most frequently reported ARRS role was pharmacist (434) followed by physiotherapist (307), paramedic (244), advanced clinical practitioner (226), adult mental health practitioner (195), physician associate (191), nursing associate (155), and trainee nursing associate (138). The 3 most common “other” responses were social prescribers (22), health and well-being coaches (18), and care co-ordinators (13).

ARRS roles deployed into practice (n = 525).
Changes in Workloads
In total 24% of respondents agreed with the statement “The introduction of ARRS roles has decreased my workload.” 66.8% disagreed with the statement. 9.3% of respondents elected for don’t know (Figure 6).
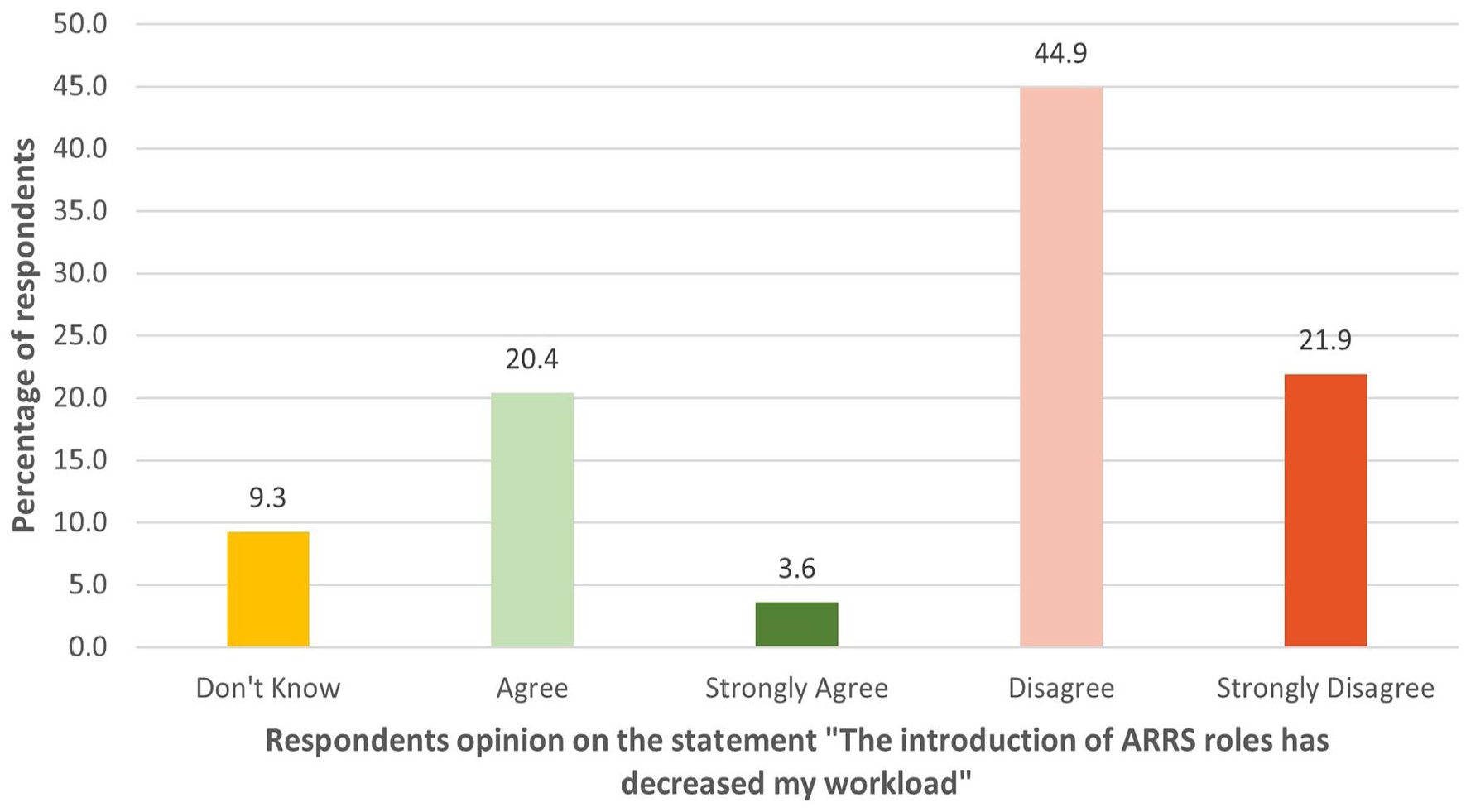
Respondents opinion of the statement “The introduction of ARRS roles has decreased my workload” (n = 530).
The free text for this question was completed by 113 respondents. All quotes are taken verbatim from the free text responses to the survey and have been anonymized where appropriate.
Although ARRS colleagues can see some of the patients the GPN would have seen, ARRS colleagues needed support, particularly those new to General Practice or working outside their traditional scope of practice.
In terms of workload, although some of this could be shared with ARRS colleagues such as long-term conditions, reviews were from the perspective of that professional group and so much of the holistic nursing work was not done:
“They will see long term conditions patients but leave complicated patients especially in diabetes to the GPN very often no follow up dates have been booked or even bloods”
Referrals to areas outside expertise such as complex musculoskeletal or mental health were helpful in terms of a positive impact on GPN workloads and patient benefits:
“I now have other colleagues I can refer patients to that are more knowledgeable and can enhance the care I am providing my patients”
ARRS colleagues seeing patients but only completing part of the work, for example leaving follow up not done or not requesting blood tests due to not being familiar with care was seen as generating more work and increased risk:
“Initially when the money was first released there was an explosion of new positions and roles, however many of these people had never worked in Primary Care, the support and training needed was provided retrospectively and, in my opinion, has been insufficient. This has also added to GP workload as they are accepting responsibility for supporting more staff, these means increased debrief time”
As part of a test-retest participants were asked if workloads had increased. 36.64% of respondents agreed with the statement “The introduction of ARRS roles has increased my workload.” 50.58% disagreed with the statement. 12.79% of respondents elected for don’t know.
There were 166 free text responses which resulted in 3 principal recurring topics in this response. The 3 topics were:
• having to teach and supervise new colleagues, new to roll or new to primary care without any additional time or resources,
• duplication of work due to inexperience in primary care or change of role, even if an experienced clinician,
• care left undone, and completing incomplete care provided by colleagues. Some ARRS colleagues new to role and working out of traditional scope such as paramedics and physician associates were reported as more risk averse and therefore sought support/education from GPNs which was welcomed but increased workloads.
The 3 topics are explored here.
Supervising and Teaching Those New to Role or Primary Care, Without Additional Resource
Participants reported that colleagues sought supervision and teaching from GPNs due to a deficit in knowledge either in clinical practice or the environment of primary care.
“More patients sent for tests that may not have been sent previously, constantly being asked advice/to review pts”
“training time, doing the parts they are unable to do (not holistic care)”
“The pharmacists and paramedics have limited ability to recognise and manage LTCs [long term conditions], limited knowledge of LTCs and their treatments, inability to have a joined up approach to pts care, poor knowledge of wounds, vaccinations and basically what general practice nurses do”
“I am a nurse manager so have organised training for pharmacists to undertake respiratory reviews. The paramedics are also undertaking simple asthma reviews. So my workload has increased. I am the only clinician able to undertake complex reviews. My concern is that some ARRS roles will not be able to do this. Their reviews are different and less robust. This is to do with time but also understanding. I am anticipating tasks asking me for advice which I’m happy about, but it makes me reflect on the role of ARRS”
Duplication of Work Done Generated by Those Not Familiar with the Work or Working Practices of Primary Care
Respondents stated that there was duplication of work due to the complexity of work, not within scope of work/practice and/or the work environment of primary care:
“repetition of work, they do a review but not everything is covered so you are having to go over it again, sometimes having to contact pt again. Review dates not being added to consultation, so pts are being missed for recalls”
“To an extent – these professionals review patients but don’t always complete the QOF requirements for reviews and then they are sent to the nursing team to mop up/review properly. I would say on occasions asking the nursing staff what to do with a patient re ?asthma diagnosis for example would save appts however I have found they have been advised to book in with a nurse after they have had a consultation with an ARRS role for us to explain we cannot do what they have been told we can and we need to do some diagnostics first before we can treat as they can’t prescribe they come to me to prescribe”
“Care is disjointed and there is duplication of work, misunderstanding of recall systems and ways of working causing patients to be asked to come in when there is no clinical requirement but the book is passed to the nurse as the solver of all issues – despite poor compliance and recent reviews/repeated education only weeks earlier or the patient would have been due to receive a letter to Tci for multiple LTC and early invites for 1 condition block the nurse appointment and unable to complete the review as we don’t have all the relevant information or not enough time has been booked as no info on f12 button ([place name] birthday recall)”
Incomplete Care and Care Left Undone
Incomplete care and care left undone was a common issue, often around ARRS staff working outside of traditional scope of practice.
“As per above often not even referring the patients to specific care like structured education, district nurse bloods”
“Have to double check pt notes / diaries are not being cleared and care plans not completed therefore additional work comes back to me”
“Extra appointments made with Nurse after seeing these”
Analysis of General Comments
When asked if respondents wanted to make any other comments, 227 responded. Several issues emerged in addition to the ones already reported such as the expectation of providing supervision.
Pay, Developmental Opportunities and Inequity
A recurring issue was inequitable pay and conditions. GPNs were expected to support and supervise ARRS colleagues, for lower pay (the most common (39.4%, n 211) GPN pay band was agenda for change band 6 equivalent). GPNs also had less access to developmental opportunities and paid time for learning compared to ARRS colleagues.
“ARRS roles are paid more than GPN’s and have less qualifications, little to no experience and require support from GPN’s earning much less. It reinforces the message that nursing isn’t a valued profession”
“It has created more work. We were never asked about our input. We get paid less then ARRS staff for doing more They aren’t as highly experienced as we are. We have to supervise them, although they often are paid in excess of us. The GPN role is disappearing We are not valued like they are even though we do more of the work. The GPN role in a whole is under valued, under paid and underappreciated”
“It has increased the need for us to provide supervision and training, when we are paid less than these colleagues it is very demoralising”
“I feel the impact of the ARRS role has been double fold nurses feel undervalued, with less recognition and the pay terms and conditions difference is apparent. Due to the lack of communication from the PCN and practices there is a lack of understanding and communication re the ARRS roles in the team. With no clear direct supervision and embedding of the roles I feel that the ARRS also feel unsupported, like they don’t belong or feel part of the wider team all of which reduce the wellbeing of all staff and positive culture. Some of these need to be addressed for recruitment and retention of all the roles”
Changes in Work, Taskification, Rescue, and Duplication/Workload Intensification/Loss of Continuity
In terms of capacity 21.6% of respondents agreed with the statement “ARRS roles mean I have more appointments available to see patients.” 71.5% disagreed. 6.8% of respondents opted for don’t know. GPNs did not feel that ARRS helped increase their capacity. The introduction of ARRS did not means GPNs saw more appropriate patients either with only 26.4% of respondents agreeing with the statement “I have been able to see more appropriate patients since the introduction of ARRS roles.” 63.4% disagreed. 10.2% of respondents opted for don’t know. GPNs were asked if the introduction of ARRS had given them the capacity to provide more holistic nursing care. Only 26.6% agreed with the statement “I have been able to give more holistic care since the introduction of ARRS roles.” 57.1% disagreed with the statement. 16.3% of respondents opted for don’t know. In terms of utilising nursing expertise, 28.8% agreed with the statement “My nursing expertise is utilised more since the introduction of ARRS roles.” 59.8% disagreed. 11.4% of respondents opted for don’t know. The free text responses reported the reverse, more taskification of care.
The taskification of care was frustrating, to employ people with less experience in primary care including those with limited experience, GPNs reported an additional rise in care delivered as protocolized tasks which they found unfulfilling compared to person centered care they aspired to. There was also a theme of devaluation of the GPN role that occurred frequently.
“No consultation. No longer holistic care. Care now becoming a tick box exercise where patient doesn’t fit. Patients confused who they are and what they do. Care more fragmented. My job satisfaction has plummeted. Not sure I want to do it anymore”
“The main impact that saddens me is how we have devolved patient care into a series of tasks delivered by different people in the practice setting. Diabetes patients used to have one holistic appointment with a nurse once or twice a year dependent on their health status. Now they can have 4 or even 5 separate appointments. Patients hate it and I hate the lack of continuity, debasement of my skills and knowledge and the fact that patients are so inconvenienced. To be fair – the GP partners hate it too”
The GPNs felt they completed more rescue work due to fractured care/taskification
“I am seeing patients who have already been seen by an ARRS role because their needs were not managed properly leading them to come back. This leads to a lack of patient confidence and more appointment time taken up. This does not always occur of course but fairly often”
“Nursing staff are being pushed to focus more on treatment room work and more of the long term condition work is being passed to ARRS roles (particularly pharmacists). However these ARRS led reviews often focus heavily on medications and do not follow the holistic review that is usually delivered by the nursing team. We are finding that patients are coming to see us despite having already had a review because they have not been supported to self manage only received a change in their meds. We are therefore doubling up on work and patient satisfaction is affected”
“Too many too quickly. Patients seem to be increasingly frustrated by seeing so many different practitioners and I end up having to explain and sort things out for them, or they are sent back to see me for follow up anyway”
“Within general practice a GPN will know the patients well and have plans for care. These can be derailed by ARRS roles when they have input into patient care. GPN;’s already take responsibility for quality work with patients and generate their own workload. Add to that the GP’s generate workload and now ARRS also generate workload without being aware of how the individual practice works and the level of skills and expertise already within the nurses in the practice. We have never been asked about suggested/planned ARRS roles within the PCN and it seems that these roles are currently to reduce GP workload. We are then asked to mentor/train/sign off new skills developed by ARRS roles. There is plenty of work within general practice for all but certainly more consultation within the general practice team not just with GP’s . There appears to never be an assessment of the impact of these roles within the practices or how they are integrating within the practice”
An Unplanned Workforce
ARRS was seen as both an opportunity and an issue of being an unplanned workforce with a poorly defined purpose apart from being a “free” resource to practices. Responses indicated there was little engagement with GPNs prior to implementing the roles, with only 12% responding that they had been consulted (Figure 4):
This lack of consultation is reflected in the comments, particularly the Trainee/Nursing Associate for which GPNs as RNs, were responsible for supervising. There was a call for associate level professionals, particularly nursing associates, to have more regulated definition of scope of practice. This was coupled with concerns about the future of ARRS and the sustainability of the GPN workforce:
“ARRS seems to be a “sticking plaster” over the issues that are currently being seen in general practice. Experienced GPNs are feeling pushed out and are underrepresented in implementation of these roles. The general GPN workforce feel undervalued. We do not know how long funding will be available for - what happens if/when it is withdrawn. Can the decimated GPN workforce pick up the pieces? There also seems to be no clear directive on the ARRS roles, especially that of NAs. Some seem to be encouraged to work outside their sphere of competence, undertaking LTC reviews and patient Management. Drivers seem to be reduced workforce cost for Management and lack of understanding of their own role. Black and white guidelines specific to General Practice for the NA role specifically need to be developed to assist with this and maintain best outcomes for patients. I have no doubt that some NAs are capable, but need to show this by completing appropriate training, ie top up to RN”
“. . . .No one seems to know what exactly they are doing let alone achieving. I thought initially that they would be a good thing to take some pressure off but they seem to create more and duplicate everything. Unimpressed by this initiative. Practice Management like them because they are funded by the PCN so “free” to the practice”
Discussion
ARRS deployment appears to have impacted the GPN workforce in several ways. There was positive impact on workloads from ARRS roles working in original scope, for example pharmacists undertaking medicine reviews or the addition of Mental Health Nurses to provide specific mental health care. Such workers impacted positively by offering more appropriate and timely care. However, any benefit was offset by the increased workloads created by those new to general practice and/or working outside of traditional scope of practice. The increase in GPN workload associated with these roles ranged from a lack of resources required to provide the support those new to primary care need to practice safely, the expectations of others that GPNs will fill the gap in support and teaching to GPNs directly safety netting the work of others.
There was a lack of consultation regarding a major workforce change, leading to feelings of devaluation. There are some significant equity issues highlighted particularly around pay and opportunity. There appears to have been no substantial demand modelling for new roles, either nationally or locally. Work/care previously done by GPs/GPNs was shifted to ARRS colleagues that they could not complete due to lack of knowledge, skill, being out of scope, regulatory/legal issues or unfamiliarity with context (primary care). This meant care was left incomplete with GPNs having to perform rescue work, complete the episode of care or teach colleagues. This was most reported in the management of long-term conditions.
There were high expectations and assumptions from employers that GPNs would support, educate, and supervise roles but without consultation or the provision of extra resources. It seems clear that a major workforce change would require support even to those experienced professionals adapting to working in primary care. In their study Bramwell et al 11 found that ARRS was perceived to save GP time by commissioners. Given that it requires additional GPN time, this assumption by commissioners may need to be tested. It is also an assumption that more people mean less work however novice workers are rarely efficient and require development in terms of skills acquisition before they become proficient in practice. 12 Developing such large-scale workforce interventions cannot be without consequence for the existing workforce. Francetic et al 13 also found that problems can arise from the complex adaptation required to adjust practice organization. Large scale changes delivered at speed also impact on the work of patients and families using the service, for example Dalgarno et al 14 found that those using services lack of knowledge about incoming practitioners constrained their agency in accessing primary care, with users of primary care reporting both increased and burdensome illness work as they were given responsibility for navigating and understanding new systems of access while simultaneously understanding new practitioner roles.
ARRS roles impacted GPN workloads as they required support because they were unfamiliar with the context of work (primary care) to the point work was left undone and GPNs had to pick up such work for safety reasons or achievement of the quality outcomes framework (QoF). In a similar finding by Penfold et al 15 the commissioning of ARRS roles was associated with small increases in patient satisfaction and perceptions of access, but not with QOF achievement. The need for support and oversight of ARRS staff has also been recognized in other studies. 11
Footnotes
Acknowledgements
The Authors would like to thank those who took part in the assessment.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This analysis was funded by the Queen’s Nursing Institute.
Ethical Considerations
The impact analysis was submitted to the HRA algorithm and determined to be evaluation. All opinions gathered from the workforce by QNI are done so in line with the MRS code of conduct.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Data Availability Statement
From the author upon reasonable request.