
Abstract
Introduction
Primary health care (PHC) is fundamental to the health and well-being of individuals, communities and populations. As a whole of society approach to promoting and supporting health and well-being, focusing on the wider determinants of health, “PHC is the most inclusive, equitable, cost-effective and efficient approach to enhance people’s physical and mental health, as well as social well-being” (World Health Organization, 2023). Certainly, strong PHC systems and services are associated with more accessible and efficient patient-centred health services, and can realise improved population health outcomes while reducing the costs associated with more expensive secondary and tertiary services (OECD, 2020). Underpinning strong PHC systems and services is a sufficient, knowledgeable, skilled and enabled PHC workforce, capable of proactive engagement with individuals and communities, and active collaboration with other health and social care professionals across the continuum of care (OECD, 2020). Recruiting and retaining a well-educated and trained health workforce is a key factor in ensuring a resilient health system (OECD, 2023).
In Australia, the PHC nursing and midwifery workforce comprises almost 100,000 nurses and midwives who work outside of hospital settings – including in primary care (general/family practice), aged care services, community health services, Aboriginal community-controlled health organisations, schools, corrections and defence – representing more than 22% of the total nursing and midwifery workforce (Department of Health and Aged Care, 2024a). Both in Australia and internationally, nurses and midwives are critical to ensuring accessible and effective PHC service delivery (WHO & UNICEF, 2018), and can play an important role in expanding the capacity of the primary care workforce (Laurant et al., 2018). Indeed, there is considerable evidence demonstrating that appropriately qualified and skilled nurses (and midwives) can ensure timely access to primary care (Ansell et al., 2017), and may provide equal or better care and higher levels of patient satisfaction across urgent physical problems and chronic conditions than can physicians (Laurant et al., 2018).
Following the peak of the COVID-19 pandemic, the International Council of Nurses (ICN) has called for a renewed focus on expanding PHC services and supporting nurses to work to their “optimal scope of practice” (International Council of Nurses, 2024). Likewise, in the Australian context, the 2022–2032 PHC 10-Year Plan has emphasised the need to ensure that nurses, nurse practitioners, midwives and allied health professionals are enabled to work to their full scope of practice (Department of Health and Aged Care, 2022a). Despite this, however, as in many countries, already existing shortages in the nursing and midwifery workforce in Australia have worsened (Berlin et al., 2022). There is an increasingly urgent need not only to recruit nurses and midwives into PHC work but, perhaps more importantly, to retain those nurses and midwives already working in diverse PHC settings.
Across a range of international studies and settings (Al Zamel et al., 2020; Halcomb, Smyth, & McInnes, 2018; Halldorsdottir et al., 2018; Russell et al., 2017), nurse retention in PHC has been found to be influenced by personal factors, professional autonomy and recognition, access to education and training, staffing levels and work conditions, which comprise key elements leading to job satisfaction and organisational commitment (Pressley & Garside, 2023). Nonetheless, significant gaps remain in our understanding of key factors currently impacting on PHC nurses’ and midwives’ intentions to remain in PHC work, across the breadth of PHC service settings, especially in Australia. For example, the extent to which the ability of PHC nurses and midwives to work to their full scope of practice impacts on their decisions to stay or leave PHC work is unclear. Determining those factors may inform advocacy and policy development efforts that promote and support the recruitment and retention of PHC nurses and midwives in Australia. The aim of this cross-sectional study was to identify key explanatory factors for nurses’ and midwives’ intentions to remain working in PHC settings in Australia.
Methods
Data were obtained from the 2022 Australian Primary Health Care Nurses Association (APNA) Workforce Survey, the largest and only annual survey of PHC nurses and midwives working in diverse PHC settings across all Australian States and Territories. The primary purpose of the APNA survey is to describe and understand the PHC nursing and midwifery workforce, their pay and conditions, the services they provide, their commitment to and satisfaction with their work, and their workforce participation decisions. This self-report survey was conducted during the final quarter of 2022 on the AlchemerTM online survey platform. Recruitment of nurses and midwives working in Australian PHC settings was undertaken from the APNA membership and contact databases, and through organisational channels, professional networks and social media. Responses were sought from a large sample of eligible respondents across a broad range of personal and professional characteristics, and diverse settings and geographical locations. Consent to participate in the survey was implied by responding to the questionnaire items. Eligibility was determined on the basis of self-reported identification as ‘a nurse and/or midwife currently employed in primary health care.’ The conduct of the current study was approved by the Monash University Human Research Ethics Committee (Ref. 41623).
Variables
The 2022 APNA Workforce Survey questionnaire included a range of personal and demographic items, primary and secondary employment items, work and well-being items, and two items asking respondents if they intended (Yes or No) to remain working in PHC over the next 12 months and in the next 2–5 years. Intention to remain, also termed intention to stay (as compared to intention to leave), is a relatively positive construct that has gained increasing interest in the research literature (Nancarrow et al., 2014). The questionnaire also included items relating to the frequency of activities conducted in respondents’ PHC nursing work. There were no validated, multiple-item scales included in the questionnaire.
In this study, the 28 variables selected from the survey questionnaire for inclusion in analyses were considered by the authors to be the most likely to be associated with the binary outcome variables ‘intention to remain working in PHC over the next 12 months’ and ‘intention to remain working in PHC over the next 2–5 years’. Potential explanatory variables (predictors) included three numerical items (age, nursing experience and PHC nursing experience in years), and the 23 categorical variables of Aboriginal and/or Torres Strait Islander (First Nations) identity, gender identity, registration status (e.g., Enrolled or Registered Nurse, Registered Midwife), career stage (e.g., recently graduated, experienced nurse), primary work setting, State/Territory, employment status (e.g., permanent, fixed term/temporary, self-employed), employment hours (full-time, part-time, casual), 10 items on aspects of job satisfaction (5-point scales from very dissatisfied to very satisfied), whether or not currently studying or having completed a postgraduate university course, the degree working to full extent of education, training and qualifications, alternatively termed working to ‘full scope of practice’ (5-point scale from regularly to never), and four items respectively on the extent feeling burnt-out, exhausted, stressed and having an excessive workload at work (5-point scale from never to always). A rural location (rurality) variable comprised one of seven Modified Monash Model (MMM) categories of rurality (Department of Health and Aged Care, 2023). This was determined for each respondent on the basis of reported State/Territory, town/suburb and postcode of the primary work setting, utilising the most recently published Department of Health and Aged Care (2019) MMM suburb and locality classification table.
Statistical Analyses
All statistical analyses were conducted using Stata version 18 (StataCorp). Data were initially downloaded from the online survey platform in an Excel file for cleaning (e.g., removal of obvious duplicates and extreme outliers) and initial data transformation operations (e.g., rurality). To assess the extent to which the APNA sample was representative of the population of PHC nurses and midwives, respondents’ age categories, sex, registration status, State/Territory and Modified Monash (MM) classification were compared with 2022 results retrieved from the National Health Workforce Data Tool (Department of Health and Aged Care, 2024a), using chi-squared (X2) tests. To facilitate comparisons, some transformations were required to align the APNA Workforce Survey and the National Health Workforce Data Tool (NHWDT) data categories.
Logistic regression modelling was employed to identify statistically significant associations between predictors and each of the two outcome variables. Prior to commencing regression modelling (with the exception of registration status, career stage, primary work setting, employment status, employment hours, postgraduate course currently studying or completed, State and MM classification), categorical variables were transformed into binary variables to facilitate interpretation. This included First Nations (yes/no), sex (male/female), job satisfaction aspects (satisfied or very satisfied / not satisfied or very satisfied), working to full scope of practice (regularly or often/not regularly or often), and the extent feeling burnt-out, exhausted, stressed and having an excessive workload at work (sometimes, often or always/rarely or never). MM classification was transformed into four categories, namely MM1 (metropolitan centres), MM2-3 (regional centres and large rural towns), MM4-5 (medium and small rural towns) and MM6-7 (remote and very remote communities). Univariate associations with each of the binary outcome variables were then determined using the point-biserial test for the numerical variables and the Kruskal-Wallis test (corrected for tied ranks) for the categorical variables (retention criteria p < 0.05). All univariate associations between each potential predictor and each outcome variable included a minimum of 3,000 responses. Three variables not associated with either outcome variable (registration status, career stage, currently studying or completed a post-graduate course) were subsequently excluded from further analyses. Missing data were eliminated listwise in regression modelling.
All included variables were initially entered into each model. Using backward stepwise elimination (retention criterion p < 0.05), the most parsimonious models were determined. Associations between each predictor and outcome variable, holding the other predictors constant, are reported as an odds ratio (OR) with a 95% confidence interval (95% CI). The odds ratio compares the odds of a predictor state occurring with the odds of the comparison state occurring (e.g., the odds of ‘yes’ compared with ‘no’ in a binary variable). This is interpreted as a positive (OR >1) or negative (OR <1) association between a predictor and an outcome occurring, with OR = 1 representing no association (Hosmer et al., 2013). The 95% confidence interval (CI) provides an estimation of the certainty of the association being observed in a population – if the 95% CI spans across OR = 1, the conclusion can be made that the association is not statistically significant. Following Hosmer et al. (2013), each model was then assessed for goodness of fit (Pearson X2 and Hosmer–Lemeshow X2 with 10 equal groups) and discrimination (area under the receiver operating characteristic [ROC] curve).
Results
Categorical Profile and Work Variables
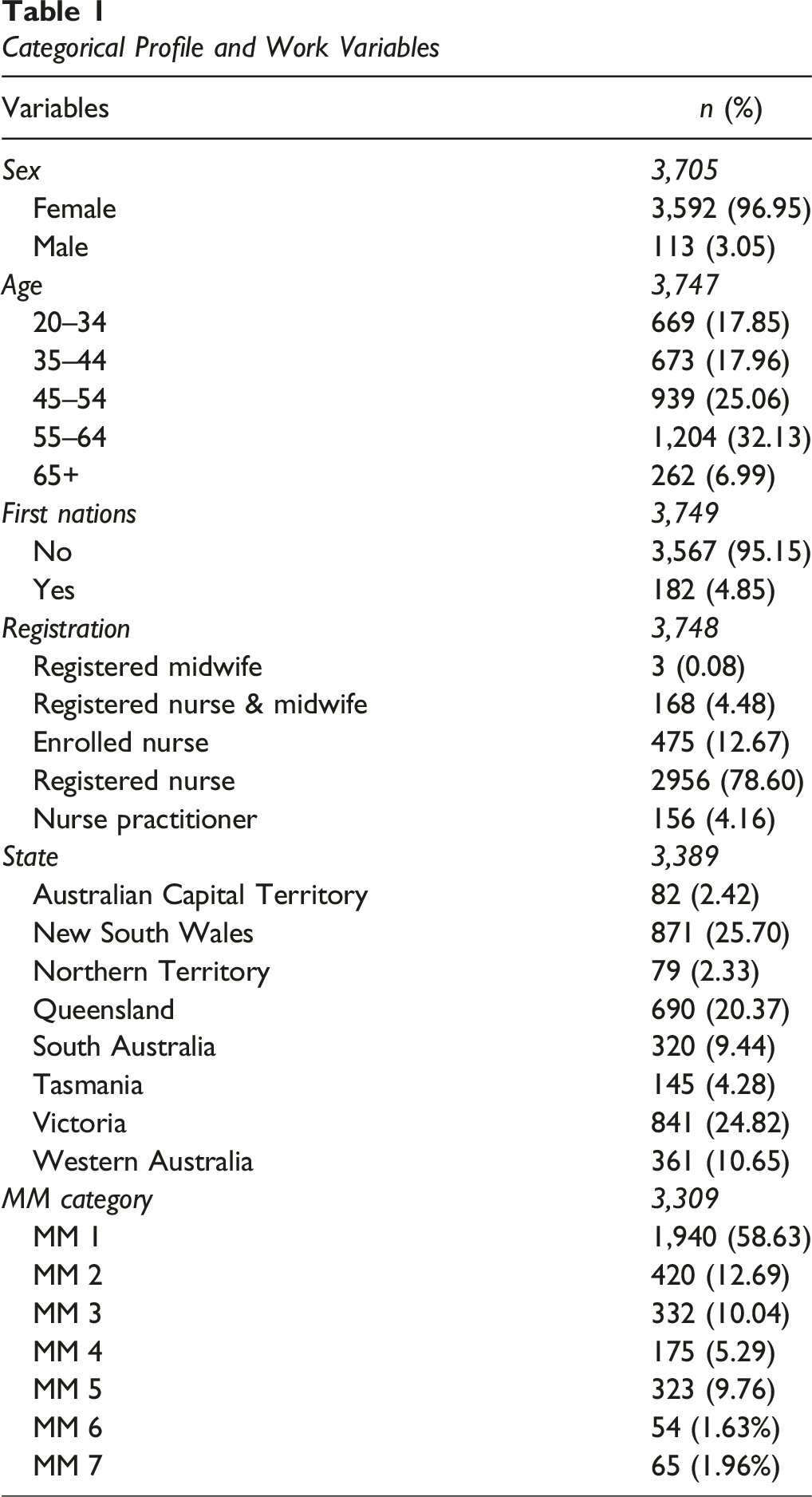
In relation to the representativeness of the respondent sample, there were statistically significant differences (p < 0.001) between the APNA Workforce Survey sample in terms of respondents’ age categories, sex, registration status, State and MM classification and the NHWDT 2022 data. The bias in the sample is evident in that PHC nurses and midwives who were male, younger, Enrolled Nurses, working in the State of Victoria and working in metropolitan settings were somewhat under-represented in the 2022 APNA Workforce Survey sample (Supplemental Table).
Model 1 – Intend to Remain Working in PHC Over the Next 12 Months (Yes/No)
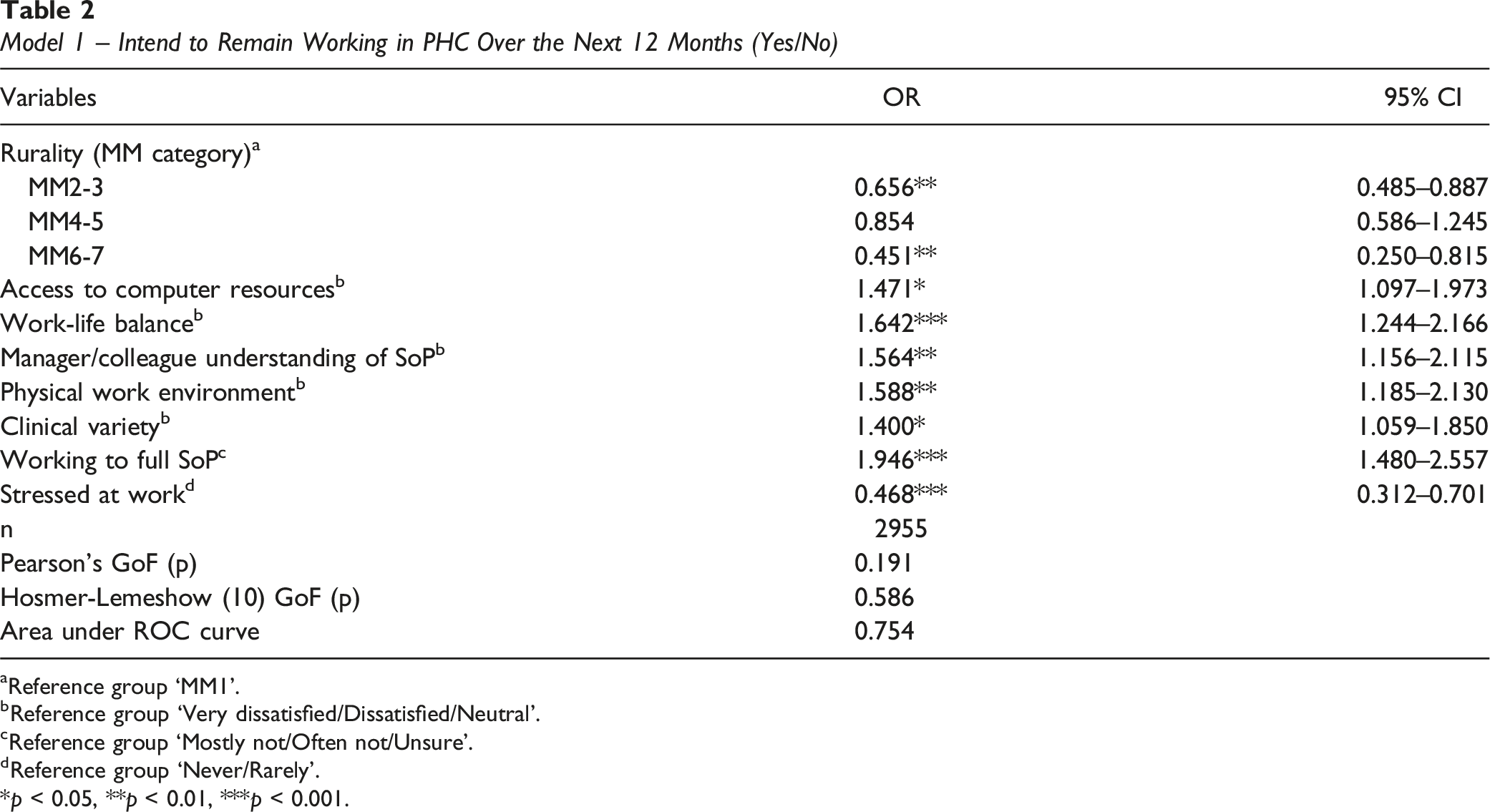
aReference group ‘MM1’.
bReference group ‘Very dissatisfied/Dissatisfied/Neutral’.
cReference group ‘Mostly not/Often not/Unsure'.
dReference group ‘Never/Rarely'.
*p < 0.05, **p < 0.01, ***p < 0.001.
Model 2 – Intend to Remain Working in PHC Over the Next 2–5 Years (Yes/No)
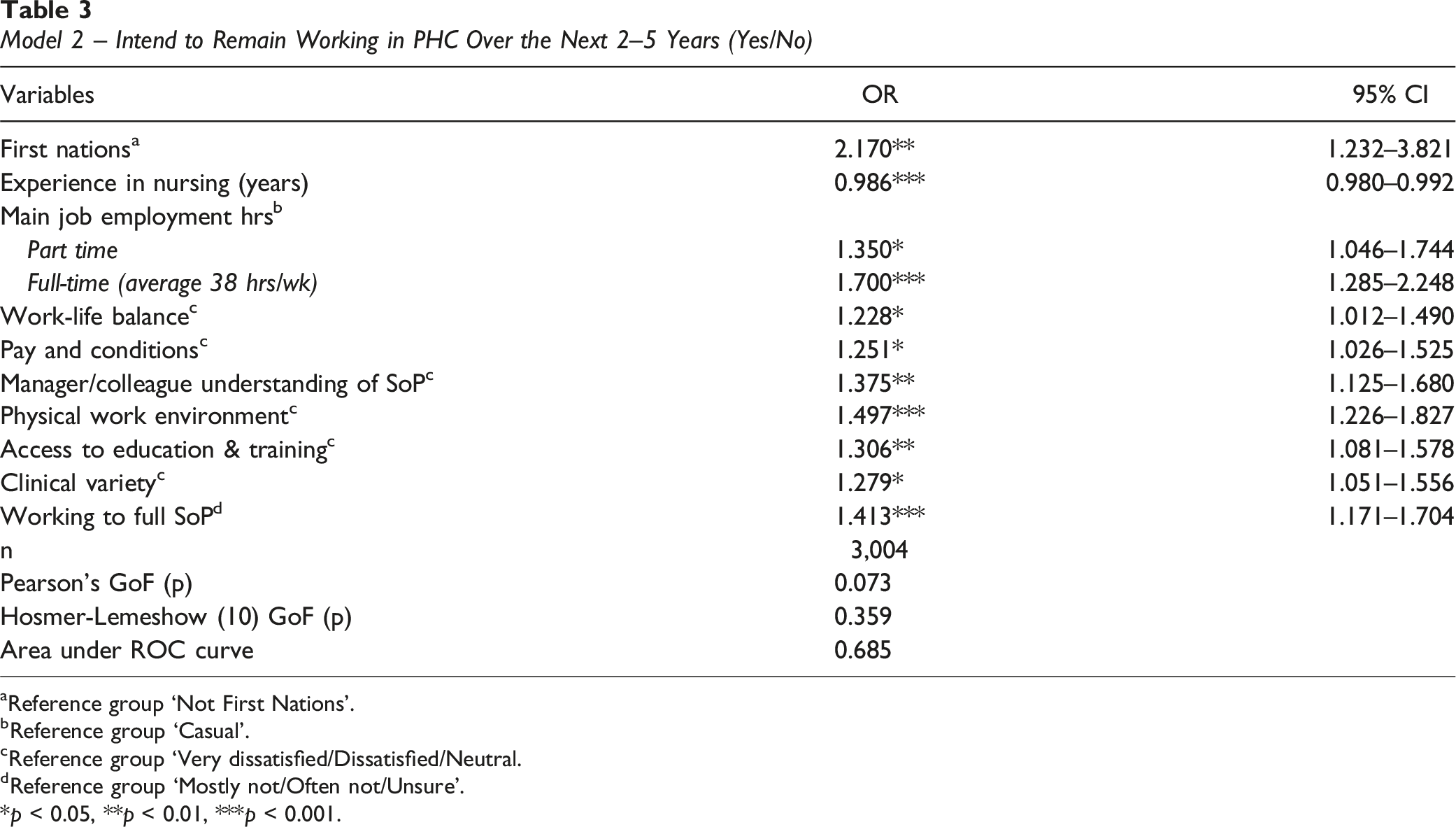
aReference group ‘Not First Nations’.
bReference group ‘Casual’.
cReference group ‘Very dissatisfied/Dissatisfied/Neutral.
dReference group ‘Mostly not/Often not/Unsure’.
*p < 0.05, **p < 0.01, ***p < 0.001.
There were notable differences in predictors determined across each model. In Model 1 (Table 2) only, primary work settings were strongly negatively associated with intention to remain in PHC work over the next 12 months in MM2-3 (OR 0.656, 95% CI 0.458–0.887) and MM6-7 (OR 0.451, 95% CI 0.250–0.815) locations, compared with MM1 locations. Also, being sometimes, often or always stressed at work, compared with being rarely or never stressed, was strongly negatively associated with intention to remain in PHC work (OR 0.486, 95% CI 0.312–0.701). On the other hand, being satisfied or very satisfied with access to computer resources was positively associated with intention to remain in PHC work over the next 12 months (OR 1.471, 95% CI 1.097–1.973).
In Model 2 (Table 3) only, increasing years of experience in nursing was slightly negatively associated with intending to remain in PHC work over the next 2–5 years (OR 0.986, 95% CI 0.980–0.992). In terms of positive associations, the odds of intending to remain in PHC work over the next 2–5 years for First Nations respondents were more than double that of non-First Nations respondents (OR 2.170, 95% CI 1.232–3.821). While a relatively large effect, given the small proportion of First Nation respondents (4.85%) compared with non-First Nations respondents, there is reduced precision demonstrated by a wide confidence interval. Also positively associated with intending to remain in PHC work over the next 2–5 years was working full-time (OR 1.700, 95% CI 1.285–2.248) or part-time (OR 1.350, 95% CI 1.046–1.744), compared with a casual appointment, as was being satisfied or very satisfied with pay and conditions (OR 1.251, 95% CI 1.026–1.525) and access to education and training (OR 1.306, 95% CI 1.081 - 1.578), compared with not being satisfied.
There were also some similarities across predictors for each model, though with a slightly diminished strength of association in Model 2 (Tables 2 and 3). Positive associations with the outcomes were determined for the job satisfaction variables (satisfied or very satisfied) of work-life balance (Model 1 OR 1.642; Model 2 OR 1.228), manager and colleague understanding of my scope of practice (Model 1 OR 1.564; Model 2 OR 1.375), the physical work environment (Model 1 OR 1.588; Model 2 OR 1.497) and experiencing clinical variety in the work (Model 1 OR 1.400; Model 2 OR 1.279), as well as often or regularly being able to work to one’s full scope of practice (Model 1 OR 1.946; Model 2 OR 1.413).
Discussion
Drawing on data from the 2022 APNA Workforce Survey, contemporary and robust models of explanatory factors associated with Australian PHC nurses’ and midwives’ intentions to stay in PHC settings over the next 12 months (the shorter-term) and over the next 2–5 years (the longer-term) were determined. Predictors only present in the shorter-term or with larger effects over the shorter-term as compared with the longer-term may relate more to ‘top of mind’ concerns or earlier decision-making in career choices, increasing the risk for employers of short-term turnover. Predictors of intention to remain in the longer-term, however, may be more reflective of factors that relate to supporting and sustaining retention. Understanding these factors is critical, given the worsening shortages in the nursing and midwifery workforce (Berlin et al., 2022), and the ongoing need to recruit and retain a well-educated and trained health workforce (OECD, 2023). Overall, in this study, predictors of intention to remain working in PHC settings fell into three main categories – personal, geographic location and work-related, with most falling into the latter category.
Regarding personal factors, years of experience in nursing was slightly negatively associated with intention to stay longer-term. While there is scant evidence in the literature of years of nursing experience being associated with intentions to stay or leave, years of experience may act as a more effective control variable than age in this sample, such as in accounting for nurses and midwives who are approaching retirement. A novel and significant finding in this study, was that the odds of intending to stay in PHC work over the next 2–5 years was more than doubled for identifying as First Nations (Aboriginal and/or Torres Strait Islander) compared to not identifying as First Nations. While the relative sample size of this sub-group was small, impacting on the precision of the results, this finding is important. There is a poor body of evidence on the First Nations health workforce in Australia, including in relation to retention and turnover (Lai et al., 2018). Notwithstanding the fact that the largest number of Indigenous employees in 2021 were nurses and midwives, Aboriginal and Torres Strait Islander people are significantly under-represented overall in the Australian health workforce, which likely contributes to reduced access to health services for the broader Indigenous Australian population (Australian Institute of Health and Welfare, 2024). In recognition of this need, the Australian Government has recently allocated more than $100 million and committed to continue developing and supporting the First Nations Health Workforce (National Indigenous Australians Agency, 2024). While the results of the current study indicate that First Nations compared with non-Indigenous nurses and midwives are more likely to stay in PHC work, concerted efforts nonetheless need to be made to recruit and retain an expanded First Nations PHC nursing and midwifery workforce. This will require attention to factors such as mentoring and support, culturally safe work environments, flexible working arrangements, access to clinical and cultural supervision and professional development, adequate salary and job security (Lai et al., 2018).
In the second category, geographic location, working in both remote settings and regional centres/large rural towns, compared with metropolitan locations, negatively predicted reported intention to stay only over the next 12 months. This may suggest that more immediate issues in these locations, such as experiencing the right fit in terms of home, work and community, can significantly impact on intentions to stay. For example, it has been found that nurses in remote settings value teamwork, being able to take short periods of leave (with backfill) and being able to establish cultural and social connectedness (Argent et al., 2022). In broader research, being able to successfully manage a range of personal and family concerns, place integration, and community participation and satisfaction can be influential in decisions to remain in rural and remote settings (Cosgrave et al., 2019; Russell et al., 2017). Being both the ‘right clinician’ and ‘feeling right’ can be critical. For example, in research on remote areas nursing in Australia (Dunbar et al., 2019), the character of the clinician and their cultural skills were found to be at least as important as their clinical skills. On the flip side, intentions to stay in rural and remote areas can be influenced by the clinician feeling like they and their significant others are able to live happy and satisfying lives in their community (Cosgrave et al., 2019).
In the third category, a range of work-related factors were found to be important associates of intention to stay in the shorter and the longer-term. Feeling stressed at work was determined to be a negative predictor of intention to stay over the shorter-term, reflecting findings in some international studies (Halldorsdottir et al., 2018; Stefanovska-Petkovska et al., 2021). It has been suggested in one international report that, in attempting to support employee well-being, addressing work demands and developing enablers can be important in managing a stressful working environment (Brassey et al., 2023). In the current study, working full-time or part time, compared to casual work arrangements, predicted intention to stay longer-term. Casual work in Australia, by global standards, is highly precarious and pervasive, and casualisation in the professions has been an issue of growing concern (Tweedie & Chan, 2022). Casual appointments may be a further source of stress for many nurses and midwives, and international research demonstrates the negative impact on mental health and well-being in those exposed to unstable or precarious work (Gray et al., 2021; Schneider & Harknett, 2019). While there is limited research on the impacts of precarious employment in nursing (Hult et al., 2022), a lack of tenure and other vulnerabilities embedded in unstable contracts has been found to influence nurse turnover in PHC work (Madrazo-Pérez et al., 2019).
Satisfaction with pay and conditions was also found to be a key predictor of intention to stay longer-term. There is a considerable body of evidence from Australia and internationally showing that remuneration for PHC work, especially in general practice, continues to be a significant source of dissatisfaction (Delobelle et al., 2011; Halcomb, Ashley et al., 2018; Halcomb & Bird, 2020; Halcomb et al., 2021; Halldorsdottir et al., 2018). This can be seen, for example, in turnover of nurses transitioning to primary care from acute settings (Ashley et al., 2018), and this has the potential to be a major constraint in attracting nurses and midwives to PHC work. Nonetheless, poorer pay rates may be counterbalanced by better working conditions, such as more favourable hours of work (Chamanga et al., 2020). Relatedly, and perhaps not surprisingly, satisfaction with work-life balance was a key predictor of intention to remain in PHC work. Work-life balance has been an important consideration for many nurses and midwives in Australia (Halcomb & Ashley, 2017), and has been identified as a key contributor to overall job satisfaction, enhancing productivity and care outcomes, and reducing turnover (Almalki et al., 2012; Chamanga et al., 2020).
Satisfaction with the physical work environment has been an important issue of concern for many nurses and midwives in Australia (Halcomb & Ashley, 2017). In the current study, satisfaction with the physical work environment increased the likelihood of intention to stay, both in the shorter and longer term, by around 50%. Satisfaction relating to access to computer resources was also identified as an important predictor of intention to stay, but only in the shorter-term. There is a dearth of research evidence related to access to information technology (including computers) and associations with intentions to stay or leave in health care, although significant limitations to accessing computers both in terms of numbers and locations in Australian health care settings have been noted in earlier research (Hegney et al., 2007). As electronic communication and data management systems have become more integral to clinical practice, including in relation to quality improvement initiatives, improving access to and managing patient care, and the digitisation of health and other records, nurses need dedicated access to contemporary computer resources to fulfil the requirements of their roles (Altmiller & Pepe, 2022). This is especially important, given the national digital health strategy to develop “… an inclusive, sustainable and healthier future for all Australians through a connected and digitally enabled health system” (Australian Digital Health Agency, 2023).
Further important aspects of work satisfaction predicting intention to stay in PHC work were identified in the current study. Satisfaction with access to education and training (i.e., professional development) predicted intention to stay longer-term, which is consistent with the research literature (Chamanga et al., 2020; Halldorsdottir et al., 2018; Rossiter et al., 2024). As a registration requirement for Australian nurses and midwives, and offering potential for enhancing professional knowledge and skills (Nursing and Midwifery Board of Australia, 2016), this finding should not be surprising, particularly where reasonable organisational support for continuing professional development might be expected for committed employees. Satisfaction with clinical variety in PHC work was also determined to be a predictor of intention to stay, though with greater effect in the shorter-term. In previous research, for example, nurses transitioning or who had already transitioned from acute to primary care work expressed concern about their loss of specialised and acute care skills (Ashley et al., 2018).
Finally, two factors relating to PHC nurses and midwives working to their full scope of practice – manager and colleague understanding of my scope of practice, and often or regularly being able to utilise their education, training and qualifications to the full extent – were predictive of intention to remain in PHC work, particularly over the next 12 months. A body of literature has identified a range of barriers to optimising scope of practice in nursing, including in relation to lack of support, insufficient remuneration, legal and professional concerns and the absence of supportive guidelines for expanding scope of practice (Birks et al., 2019). Other factors include concerns related to professional identity, role confusion, regulatory policies, organisational structures and financial factors (Wiggins et al., 2022). Importantly, lack of autonomy, lack of manager appreciation and not being able to fully utilise competencies have been identified as key drivers of intention to leave nursing work in community settings (Chamanga et al., 2020). In Australia, recent inquiries have highlighted concerns about the underutilisation of the capabilities of nurses, midwives and other clinicians in primary care, which has been envisaged as the core of a modern and effective health system in this country (Department of Health and Aged Care, 2022b, 2024b). The primary aim of these inquiries has been to precipitate much needed change in the structure and function of non-hospital based health care, especially in primary care, through legislation, policy, funding and practice (Department of Health and Aged Care, 2022b, 2024b).
In summary, this study shines a light on a range of fixed and modifiable factors associated with nurses’ and midwives’ intentions to remain working in PHC, contributing to the evidence base in terms of the presence and size of the effect of these factors. These factors are important in terms of their potential contribution to the recruitment and retention of PHC nurses and midwives, and that are of recent or emerging policy and practice focus. The costs of poor clinician workforce retention can be considerable, including restricting access to safe, high-quality care, loss of skills and experience, and high recruitment costs. First of all, nurses and midwives need to be recruited to PHC practice, and it is vitally important for transitioning clinicians to be properly oriented and supported, including through further education, mentoring and supervision (Ashley et al., 2018; Cox et al., 2023; Delobelle et al., 2011; Rossiter et al., 2024). Then, strategies need to be in place to facilitate clinician retention, being sufficiently tailored to the specific needs of clinicians with differing qualifications, experience and capabilities, practising in diverse contexts and settings (Buykx et al., 2010; Nguyen et al., 2023; Russell et al., 2017; Wakerman et al., 2019).
There are some limitations to this study. Firstly, self-report data were obtained from a cross-section of PHC nurses and midwives in Australia. This may have affected the reliability of some responses and, because only associations between variables were able to be determined, attributions of causation cannot be reliably made. Threats to the generalisability of the results are also present. While the large sample of respondents provided good representation across demographic categories and PHC work settings, sampling biases were evident. Self-selection bias, especially by those who readily identified themselves as PHC nurses and midwives, and those who were current and past financial members of APNA, may also have been present. Importantly, it is likely that key explanatory factors, including those related to personal, life and work-related circumstances, may not have been fully captured in the APNA Workforce Survey questionnaire, particularly in relation to potential predictors of longer-term intentions to remain working in PHC. Additionally, the considered selection of variables for initial inclusion in the modelling may have omitted variables of potential significance. Further, in the regression models, the validity and precision of the results may have been impacted by the presence of missing data and small category sizes in binary factors. Overall, generalisability to other countries may be limited due to the specific contexts and characteristics of PHC in Australia.
Conclusion
Overall, in this study, a number of personal, job satisfaction and work-related factors were identified as key predictors of PHC nurses’ and midwives’ intentions to remain in PHC work. The results of this study provide information on important areas that may be addressed to support the retention of nurses and midwives in PHC settings. Some factors are fixed (e.g., First Nations identity), while others are modifiable (e.g., work hours, pay and conditions, aspects of job satisfaction, working to full scope of practice). Both types of explanatory factors need to be taken into consideration when developing strategies to recruit and retain appropriately qualified and experienced nurses and midwives in PHC practice, especially in relation to Indigenous clinicians, and those in rural and remote practice. Broader-scale initiatives are certainly warranted, such as Government initiatives to promote and support clinicians working to their full scope of practice (Department of Health and Aged Care, 2022b). Nonetheless, local and organisational strategies can and need to still be initiated to support nurses’ and midwives’ intentions to remain in PHC work, in consideration of local contexts and characteristics. Further research on this topic is certainly warranted, both in the Australian and international contexts. Including questionnaire items on individual health and well-being, and other personal and life factors may assist with building more robust models. Further inquiry into the more novel findings of this study, such as First Nations status as a predictor for intention to stay in PHC work, are recommended. Longitudinal study designs may also aid in the development of causal models, including taking into account structural and other broad scale changes that may emerge over time.
Supplemental Material
Supplemental Material - Factors Associated With the Workforce Participation Intentions of Australian Primary Health Care Nurses and Midwives
Supplemental Material for Factors Associated With the Workforce Participation Intentions of Australian Primary Health Care Nurses and Midwives by Danny Hills, Cressida Bradley, and Manan Mehta in Evaluation & the Health Professions
Footnotes
Statements and Declarations
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded internally by the Australian Primary Health Care Nurses Association.
Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.