
Abstract
Background:
Approximately two-thirds of diabetes patients develop multimorbidity, which is associated with increased mortality. We aimed to examine whether, and to what extent, the time interval between pre-existing diabetes and a second chronic disease may be associated with the risk of mortality.
Methods:
We carried out a territory-wide nested case-control study using incidence density sampling, utilizing electronic health records from Hong Kong’s public healthcare facilities. Among 158 732 patients first diagnosed with diabetes from January 1, 2010 to December 31, 2012 and subsequently developed multimorbidity as of December 31, 2019, we extracted those who died before December 31, 2019 as case participants. For each participant, we randomly matched with up to 4 people of the same sex, multimorbidity age, and second chronic condition who had not died after going through the same survival period of the case participant. Multimorbidity interval was included as a continuous variable. We used conditional logistic regression to estimate adjusted odds ratios (aOR) for mortality.
Results:
In total, 3508 case participants were matched with 14 032 control participants. Conditional logistic regression showed there were 19%-reduced odds of mortality following the extension of multimorbidity interval by 1 year. Similar associations were observed in men, women, people aged 64 years or younger, and older people aged 65 years or more.
Conclusions:
Delayed multimorbidity among patients living with diabetes may be related to a lower risk of mortality. This study suggests that we should focus on mitigating and lowering the risk of multimorbidity in clinical management of diabetes to reduce further complication and mortality.
Introduction
Diabetes was ranked as the eighth leading cause of death and disability worldwide in 2019, representing a rapidly growing healthcare burden that affected 460 million individuals.1,2 Global prevalence among individuals aged 20 to 79 years was estimated at 10.5% in 2021. 3 Approximately 12% of the adult population in China has diabetes, accounting for nearly 1 quarter of all global cases. 4 Likewise, in Hong Kong, 2020, the prevalence of diabetes among individuals aged 15 to 84 years was 8.5%, and it contributed to 1.2% of all registered deaths in the city. 5
Multimorbidity, most often referred to as the coexistence of 2 or more chronic health conditions in the same individuals, is shown to be increasingly prevalent in people living with diabetes.6 -8 In China, the prevalence of multimorbidity among individuals with diabetes has been estimated at 65.2%. 9 Commonly observed clusters of multimorbidity mainly comprise conditions closely linked to the pathogenesis of type-2 diabetes, including hypertension, lipid metabolism disorders, and obesity. These conditions, together with those physiologically less connected diseases, represent at least part of the mechanism leading to a significantly increased risk of death. 10 There is an evident inverse relationship between multimorbidity and quality of life (QoL), 11 with more complex clinical challenges imposed for individuals and their healthcare providers, leading to poorer treatment and other health outcomes. 6 In addition, multimorbidity is consistently shown to be associated with a higher risk of mortality in older people. 12 Considering the high prevalence of multimorbidity among people with diabetes and the increased risk of mortality among individuals with multimorbidity, it is crucial to implement evidence-based strategies to reduce or mitigate the burden incurred by multimorbidity.
In this regard, clinicians who manage patients with diabetes and multimorbidity could benefit considerably from a temporally informed perspective of multimorbidity development in relation to subsequent health outcomes, which is beyond previously known evidence on the cross-sectional disease clustering patterning. 9 Of note, there is currently a lack of studies investigating the association of time interval between diabetes and subsequent multimorbidity with the risk of mortality. This study aims to use a territory-wide electronic public healthcare database in Hong Kong to determine whether, and to what extent, a longer time interval between first-diagnosed diabetes and a second chronic disease may be associated with the risk of mortality. We speculate that a shorter time interval from pre-existing diabetes to the diagnosis of the second chronic condition may indicate a tighter timeframe within which health care needs to be provided or an intrinsically rapid deterioration of the physical condition; that could hence worsen the risk of mortality. In this study, we hypothesize an inverse association between multimorbidity interval, that is the time interval between first-diagnosed diabetes and a second chronic disease, and mortality risks.
Methods
Data Sources
This study obtained data from Hong Kong Clinical Data Analysis and Reporting System (CDARS), a territory-wide electronic health database of admissions to all public hospitals of Hong Kong, where the demographic information, diagnosis records, medicine records and death registrations of patients are available for the analysis. The CDARS is overseen by the Hong Kong Hospital Authority (HA), a public healthcare statutory body responsible for managing all 43 public hospitals and institutions, along with 122 outpatient clinics throughout Hong Kong. HA plays a crucial role in delivering outpatient services in Hong Kong. Data gathered from these institutions is automatically transmitted to the data warehouse and subsequently relayed to the CDARS system for reporting, auditing, and research objectives. 13 All CDARS records are anonymized and thus there is no risk of patient identification. The reliability of data from the CDARS has been demonstrated in previous epidemiological studies that used CDARS data. 14
Study Design and Participants
We conducted a territory-wide nested case-control study to explore the assumed relation between the multimorbidity interval and mortality risk among adults with diabetes merely. We adopted the death of participants with multimorbidity as the outcome of the study. The underlying cohort comprised all individuals initially diagnosed with diabetes from January 1, 2010 to December 31, 2012 and subsequently diagnosed with another 1 of the 29 chronic conditions that are specified in a well-validated and widely used list as of December 31, 2019. 15 It needs to be emphasized that patients with any diagnosis records of any listed chronic conditions 2 years before the diabetes diagnosis were excluded from the underlying cohort, that is, the wash-out period was 2 years. Supplemental Table 1 displays the diagnostic codes used to identify chronic conditions according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). The 29 conditions were atrial fibrillation, chronic heart failure, hypertension, myocardial infarction, peripheral vascular disease, stroke or TIA, cancer (metastatic), cancer (non-metastatic), lymphoma, alcohol misuse, dementia, depression, epilepsy, Parkinson’s disease, schizophrenia, asthma, chronic kidney disease, chronic pain, chronic pulmonary disease, chronic viral hepatitis B, cirrhosis, hypothyroidism, irritable bowel syndrome, inflammable bowel disease, multiple sclerosis, peptic ulcer disease, psoriasis, rheumatoid arthritis, and severe constipation.
Case and Control Participant Selection
We conducted incidence density sampling for matching case and control participants. From the underlying cohort, we selected the patients who died after developing multimorbidity within the follow-up period as case participants. We defined the time interval from the date of developing multimorbidity (day 0) to the death date (index date) as survival period of case participants. We randomly selected patients from the underlying cohort with the same age at the diagnosis of the second chronic condition, gender, and second chronic condition, who had not died after the same survival period as the case participants, to serve as control participants matched with the case participants. Each case participant was matched with up to 4 control participants. Control participants could serve as a control up to 4 times and were allowed to become a case later. 16
Exposure
The study focused on the multimorbidity interval as the primary continuous exposure of interest, measured in years. The multimorbidity interval was defined as the time interval from the date of diagnosed as diabetes (ie, the first chronic disease) to the date of developing multimorbidity, which is marked by the diagnosis of a second chronic disease.
Covariates
The covariates considered in the multivariable analysis were the age, sex, second chronic disease (already addressed using case-control exact matching, thus, not included in multivariable regression models) and the use of the following medication (dichotomized) during the survival period (included in multivariable regression models): renin angiotensin system agents, beta blockers, calcium channel blockers, diuretics, nitrates, lipid lowering agents, insulins, antidiabetic drugs, antiarrhythmic drugs, oral anticoagulants, antiplatelets, steroid, antidepressants, antiviral drugs, antibacterial drugs, immunosuppressants. Supplemental Table 2 displays the British National Formulary (BNF) codes used for identifying the medications.
Statistical Analysis
Conditional logistic regression was employed to calculate the adjusted odds ratio [adjusted OR (aOR), with 95% confidence interval (CI)] of death among patients with different multimorbidity intervals. Subgroup analysis was performed on men, women, individuals aged 65 years or older, and those younger than 65 years. Additionally, stratified analysis was carried out for each of the second chronic conditions to explore any variations in mortality risk related to the multimorbidity interval among different disease groups (potential effect modifier). Sensitivity analyses were conducted to check for any influence from (1) those who used insulins within 1 year leading up to the date of diabetes diagnosis or (2) those who developed multimorbidity 3 months after diabetes diagnosis to the results by removing those people from the main analysis. These post-hoc sensitivity analyses were conducted to test for the robustness of the results given the potential biases from a delayed record of diabetes diagnosis and detection bias respectively.
Python (Version 3.9.13) and R (Version 4.2.1) were used to perform statistical analysis. The statistical tests were 2-tailed, with P values of <.05 considered statistically significant.
Results
Figure 1 illustrates the participant selection procedures. Among the 158 732 patients diagnosed with diabetes from 1 January 2010 to 31 December 2012, there are 31 299 patients whose first chronic condition is diabetes, after the exclusion of 127 429 patients with any 1 of the listed 30 chronic conditions within 2 years before the date of diabetes diagnosis and the exclusion of 4 patients without birthday information. Among the 19 987 patients with age over 18 years when developing multimorbidity as of 31 December 2019, 3508 unique patients dying before 31 December 2019 were chosen as the mortality case participants and were paired with 14 032 survival control participants of the same multimorbidity age by year, gender, and new chronic condition diagnoses at the date of developing multimorbidity, who kept survival after going through the same survival period of the case.
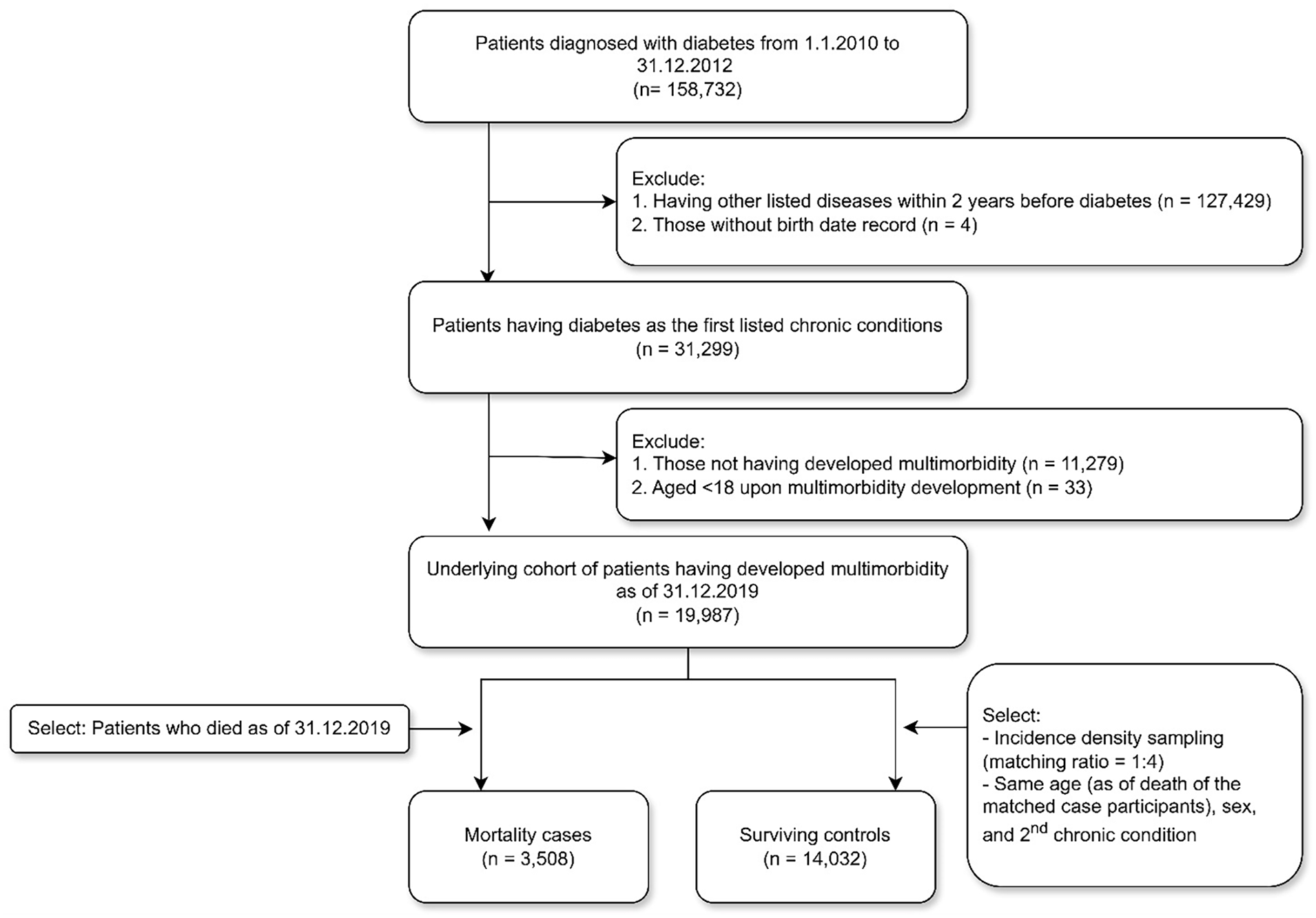
Flow diagram showing the selection of case and control participants.
Sample Characteristics
Table 1 displays the sample characteristics frequencies categorized by case and control status, along with the standardized mean differences computed between the 2 groups. Most characteristics were similar between case and control participants, except for the multimorbidity interval, which exhibited a standardized mean difference exceeding the commonly used threshold of 0.1, indicating a significant difference. The average age of the sample was about 75 years, with males making up approximately 56% of the group. As the most prevalent condition, more than 40% of the sample were diagnosed with hypertension as the second disease constituting multimorbidity, followed by chronic kidney disease in slightly more than 18% of the patients, and chronic pain was present in approximately 10% of the sample. The drug use of cases and controls are dissimilar. Case participants show a higher frequency of using antibacterial drugs, antidiabetic drugs and diuretics during their survival periods compared with other medications, whereas antidiabetic drugs, calcium channel blockers and lipid lowering agents were 3 of the most frequently used medications among the controls.
Participant Characteristics.

Abbreviations: Age, the age when developed multimorbidity; SD, standard deviation; TIA, transient ischemic attack.
Association of Multimorbidity Interval With Mortality
Table 2 displays the main analysis and subgroup analysis based on age and gender. Overall, conditional logistic regression indicated that the risk of mortality reduces by approximately 19% with the extension of multimorbidity interval by 1 year [95% confidence interval (CI) 17%-21%] after adjusting the medications prescription listed in the Supplemental Table 2 within the period from the date of developing multimorbidity (day 0) to index date. Similar correlations were calculated in men [adjusted odds ratio (aOR) for multimorbidity interval: 0.83, 95% CI 0.80-0.85], in women (aOR for multimorbidity interval: 0.78, 95% CI 0.78-0.81), in people aged 64 years or younger (aOR for multimorbidity interval: 0.81, 95% CI 0.76-0.86), in older people aged 65 years or more (aOR for multimorbidity interval: 0.81, 95% CI 0.79-0.83). Figure 2 displays the stratified analysis by second disease, that is, the new chronic condition diagnosis after diabetes that makes the person identified as having multimorbidity, with largely similar results with the main analysis. Supplemental Table 3 presents the sensitivity analysis that eliminated those who used insulins within 1 year prior to the date of diabetes diagnosis from the underlying cohort of main analysis, since the diabetes patients who used insulins before diabetes diagnosis might have delayed diabetes diagnosis and underestimated multimorbidity interval. Supplemental Table 4 shows the sensitivity analysis that eliminated those who developed multimorbidity 3 months after diabetes diagnosis from the underlying cohort of main analysis, since the diabetes patients who developed multimorbidity in really short time probably already had multimorbidity previously, but they had not diagnosed with multimorbidity until a series of physical examinations following the diabetes diagnosis.
Results of Conditional Logistic Regression Examining the Association of Multimorbidity Interval and Risk of Mortality.

Abbreviations: CI, confidence interval; OR, odds ratio.
Adjusted variables include renin angiotensin-system-agents, beta blockers, calcium channel blockers, diuretics, nitrates, lipid lowering agents, insulins, antidiabetic drugs, antiarrhythmic drugs, oral anticoagulants, antiplatelets, steroid, antidepressants, antiviral drugs, antibacterial drugs, and immunosuppressants prescribed within the period from the date of developing multimorbidity (day 0) to index date.

Stratified analysis by the second chronic condition.
Discussion
In this territory-wide nested case-control study involving 20 000 patients with diabetes and multimorbidity in Hong Kong, we estimated a modest decrease in the mortality risk of about 20% following a 1-year extended multimorbidity interval between diabetes and the other disease. The result is consistent across various subgroups, including men, women, older adults, younger adults, and different disease groups (secondary chronic conditions). Our hypothesis regarding the link between an extended multimorbidity interval and the risk of mortality is, therefore, well supported by the data.
Impacts of multimorbidity on the risk of mortality and other adverse health outcomes, such as hospitalization, are consistently observed and well-established in the existing literature.17 -19 It has been shown, using real-world evidence, that continued care for the prevention and management of multimorbidity is highly important in lowering the risk of mortality.20 -22 In addition, there has been research showing the varying impacts of different multimorbidity patterns on mortality risks.23 -26 This study, nevertheless, is the first to investigate similar such impacts of the length of time interval between pre-existing diabetes and subsequent multimorbidity on the risk of mortality. This study quantified the potential protection against mortality from a delayed multimorbidity incidence among patients living with diabetes. Our findings suggest that clinical management of diabetes should focus on mitigating and lowering the risk of developing multimorbidity to reduce further complications and mortality. This implication is of high importance because multimorbidity is not only indicative of the healthcare burden in the population, but is also known to be an important risk factor of mortality. 12 This quantification of the reduced mortality risks associated with delayed multimorbidity of a wide variety will enable clinicians to better assess the risk and benefits of different treatment options and more accurately project the prognosis of patients with diabetes.
There could be various pathways or mechanisms underlying the association between an extended multimorbidity interval and a reduced mortality risk among people living with diabetes. In comparison to patients with shorter multimorbidity interval, those patients who experienced a longer interval before developing the second chronic condition are usually characterized by better physical conditions, better health awareness, and potentially also better disease management with regular follow-up, which accounts for the lower risk of mortality. Nevertheless, it is also possible that the diagnosis of diabetes was delayed in the first place and the disease progressed without proper management until it was detected or symptomatic presentation at a later stage. The risk of complications and second chronic diseases thus markedly increased. For these patients, it might not be clear whether further interventions to slow multimorbidity incidence would be as beneficial in reducing the risk of mortality. Multimorbidity patterns that include diabetes and related diseases, cardiometabolic multimorbidity, are shown in previous research to be associated with the highest risk of mortality compared with other patterns. 24 Since the diseases included in these patterns are typically physiologically related to diabetes, the probability of it developing and getting diagnosed is significantly higher, and time required for this incidence of the second disease would be much shorter as well. 24 In our study, for example, more than 40% of multimorbidity patients were diagnosed with hypertension after diabetes, which falls under the definition of cardiometabolic multimorbidity pattern. This could also be an explanation for the observed association.
There are some clear critical strengths in this study. First, this study utilized CDARS, a comprehensive database with standardized recording and coding protocols that cover over 80% of the total population in Hong Kong. 27 The trustworthiness of the electronic health records obtained from public healthcare facilities in Hong Kong has been previously validated.28 -30 Second, licensed doctors utilized an extensive, tertiary-wide electronic health record system to establish diagnoses and document prescriptions. The diagnoses records in this system have been rigorously validated, affirming their accuracy and completeness. Therefore, any potential biases introduced by the coding system are kept to a minimum. 31
However, it is also important to interpret certain limitations with caution. First, as with any observational study lacking randomization, we could not completely eliminate all potential confounding factors, particularly those stemming from residual confounders. The data used in this study did not include lifestyle factors and various biomarkers that could be linked to the risk of multimorbidity, such as HbA1c, blood pressure, tobacco use, and exercise, etc. The severity of diabetes at the time of diagnosis was also not observed and thus not included as a potential confounder in the analysis. Second, while the list of diseases used to define multimorbidity is well-validated, 15 it is not comprehensive, but prior studies has indicated that including more than 12 diseases does not significantly alter the prevalence of multimorbidity. 32 Third, the database utilized in this study exclusively encompasses public health care services in Hong Kong. Therefore, patients who sought care solely in the private sector are not included in this study. Fourth, the different drug dosages were not considered in analyses, which may affect the magnitude of the association. Fifth, the Hong Kong population is predominantly of ethnic Chinese descent, necessitating the validation of the findings in other populations. Sixth, we did not examine how multimorbidity intervals between the first 2 diseases might be associated with the risk of developing the third and fourth diseases. Further studies should examine this association and explore the potential of such an association as a mediating factor between multimorbidity intervals and mortality. Seventh, we only examined those who had diabetes and then developed a second disease without considering other possible sequences of multimorbidity development. Further studies should consider this important aspect of multimorbidity exposure and its impact on health outcomes. Last but not least, as a result of the case-control design, the study was unable to determine the incidence (absolute risk) of multimorbidity. Future cohort studies are required to ascertain this information.
Conclusions
In conclusion, we found that delayed multimorbidity incidence among diabetes patients may be related to a lower risk of mortality, with approximately 20%-decrease associated with 1 year of delayed multimorbidity. Emphasis should be placed on comprehensive health management of diabetes patients when allocating medical resources and health services to slow multimorbidity incidence. Further research should investigate interventions that aim at such a delay and examine how that may be related to a better survival among people with diabetes.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241293950 – Supplemental material for Longer Multimorbidity Intervals Are Associated With Lower Mortality in Diabetes: A Whole-Population Nested Case-Control Study
Supplemental material, sj-docx-1-jpc-10.1177_21501319241293950 for Longer Multimorbidity Intervals Are Associated With Lower Mortality in Diabetes: A Whole-Population Nested Case-Control Study by Wenlong Liu, Yuqi Hu, Cuiling Wei, Lingyue Zhou, Boyan Liu, Qi Sun, Rachel Yui Ki Chu, Eric Yuk Fai Wan, Ian Chi Kei Wong and Francisco Tsz Tsun Lai in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The authors thank the Hospital Authority for the provision of data for this study. F.T.T.L. and I.C.K.W.’s roles in University of Hong Kong were partly funded by D24H; hence this work was partly supported by AIR@InnoHK administered by the Innovation and Technology Commission, The Government of the Hong Kong Special Administrative Region.
Author Contributions
WL and FL contributed to the conception of the work and drafting of the manuscript. YH, CW, LZ, BL, QS, RC, EW, and IW read and critiqued the manuscript. WL and FL contributed to the acquisition and analysis of the data. All authors designed the study and contributed to the interpretation of the results. All authors revised the manuscript critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Data Availability
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Health and Medical Research Fund under the Health Bureau of Hong Kong.
Ethical Approval
This research was conducted in accordance with the Declaration of Helsinki. Ethics approval was granted by Institutional Review Board of the University of Hong Kong/ Hospital Authority Hong Kong West Cluster (HKU/HA HKW IRB) with an exemption for informed consent from participants as patients’ confidentiality and anonymity were maintained in this nested case-control study (Reference number: UW 24-296).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.