
Abstract
Background:
Globally, most patients with hypertension have suboptimal blood pressure (BP) control. Multiple barriers prevent primary care physicians (PCPs) from effectively caring for these patients. This study aimed to explore the challenges faced by PCPs in providing optimal care for patients with hypertension, with a specific focus on identifying new barriers.
Methods:
This qualitative study involved 17 PCPs across 5 primary care clinics in Singapore. A trained researcher conducted individual in-depth interviews using a topic guide. Purposive sampling was employed to ensure adequate representation of seniority until data saturation was achieved. The audio-recorded interviews were transcribed verbatim and independently checked. The data were managed using NVivo and thematic analysis was conducted.
Results:
New barriers were divided into patient, physician, drug, and systemrelated factors. Patient factors included a preference for natural health remedies and the inconvenience of blood tests. Meanwhile, physicians faced challenges diagnosing and treating patients with various BP phenotypes and BP variability. The initiation of dual therapy was a drugrelated barrier. Finally, system factors included the suboptimal layout of the electronic medical records (EMR) that impeded effective hypertension management.
Conclusion:
A multi-pronged approach is required to address the significant barriers to providing optimal hypertension care. Patients should be empowered through education and minimizing the inconvenience of medication titrations. Additionally, physicians should be better equipped to diagnose and treat patients with more challenging BP phenotypes. Finally, improved access to combination pills and an optimized EMR would contribute to improved care for patients with hypertension.
Introduction
Hypertension is one of the most common chronic diseases, affecting up to one-third of the global population. 1 In recent years, hypertension management has evolved rapidly, with robust evidence utilized to develop clear Clinical Practice Guidelines (CPGs) on diagnosis, monitoring, and treatment.2,3 Despite these advances, hypertension detection and management remain suboptimal, with a recent American study finding more than 60% of the participants had poorly controlled hypertension. 4 There is increased morbidity and mortality in patients with poorly controlled hypertension, with ischemic cardiac disease being a common sequelae. 5 Apart from the impact on patients, there are high costs associated with managing poorly controlled hypertension, with direct costs accounting for 10% of the total global health expenditure. 6
Globally, optimal hypertension care is impeded by barriers related to patients, healthcare providers, and the healthcare system. 7 American studies found poor patient insight into their disease and medication non-adherence are common barriers to hypertension management.8,9 European and Australian physicians faced challenges trusting and keeping abreast with the latest guidelines, with concerns over possible drug side effects affecting their prescribing practices.10 -12 Short consultation times and difficulties securing clinic appointments are common system factors hindering the provision of hypertension care in India and the United States.13,14 Locally, Singapore is not immune to the abovementioned barriers, with prior studies identifying similar challenges.15 -17
Singapore is a high-income country with a well-resourced hybrid private-public healthcare system. Most patients with hypertension are managed in public primary care clinics (polyclinics), where patients have access to affordable healthcare services, a trained multi-disciplinary team and an established electronic health record system. 18 Polyclinics are purposively sited by the government near housing estates to provide subsidized consultations and medications to the residents; 10 to 30 doctors staff each polyclinic. Most polyclinics are equipped with basic radiological and laboratory facilities, and some newer clinics boast additional physiotherapy, podiatry, and dental services. Despite the available resources and expertise, 23.5% of Singapore residents aged 30 to 69 years were hypertensive, with 57% of subjects exhibiting uncontrolled hypertension.19 -21
Although prior studies have identified multiple barriers to providing optimal care, persistently poor outcomes suggest additional challenges exist. Therefore, this study aims to explore the challenges primary care providers (PCPs) face in caring for patients with hypertension, specifically focusing on identifying new barriers.
Methods
Study Design
An exploratory qualitative study using the descriptive-interpretive approach was conducted to explore the views, experiences, and challenges faced by PCPs in managing patients with hypertension. 22 The descriptive-interpretive approach allows researchers to go beyond describing the actions and words (descriptive) to uncover deeper meanings, motivations, and interpretations (interpretive); this method can reveal richer insights into participants’ experiences and viewpoints.
Study Sites
The study was conducted across 5 primary care clinics located in Eastern Singapore: Bukit Merah, Eunos, Marine Parade, Pasir Ris, and Sengkang Polyclinics. In 2022, there were approximately 200 000 patient visits for hypertension and 850 daily attendances across the study sites.
Recruitment Period
Participants were recruited from April to August 2022.
Research Team
The team comprised 1 female and 2 male PCPs who regularly manage patients with hypertension. All researchers are trained to conduct qualitative research.
Study Population
This study included PCPs at the study sites involved in the clinical care of patients with hypertension. Those under 21 years of age were excluded from the study; no exclusions were made based on ethnicity or gender.
Recruitment
An email invitation was sent to PCPs to introduce the study and provide an opportunity for them to participate. Written informed consent was obtained from all participants before their in-depth interviews (IDIs). Participants were recruited through purposive sampling based on their seniority and clinical roles, as these factors might influence the challenges they faced when managing patients with hypertension. Recruitment was continued till data saturation was achieved. 23 Several interviewees were known to the study team, and steps were taken to maintain their autonomy by ensuring their participation was voluntary.
Study Instruments
Participants’ demographics, clinical experience, and qualifications were collected using a demographic data collection form.
Topic Guide
The topic guide was developed through a literature review and team discussions to explore the PCP’s experiences and challenges in managing patients with hypertension. The guide covered the profile of patients seen by the doctor, their clinical practice and the challenges faced in managing patients with hypertension. After pilot testing the topic guide with 2 doctors, additional topics (eg, challenges in managing diastolic hypertension and patient’s preference for natural health therapy for hypertension treatment) were included and asked in the subsequent interviews. The final version of the topic guide can be found in the Supplemental S1 Appendix.
Data Collection
The participants provided their demographic information before the semi-structured IDIs. One researcher (MD and PhD) conducted all interviews based on the topic guide in a quiet and unoccupied clinic room. Participants were given the option for the interview to be conducted in English, Mandarin, or Bahasa Melayu. All participants opted to have the interview in English with no language barriers encountered. The interviews lasted 45 to 60 min, and participants received an SGD20 voucher (approximately USD15) for their time and effort.
The interviewer was the only study team member aware of the participants’ identities. All participant particulars were redacted from the interviews before transcribing. Additionally, the remaining study team members analyzing the de-identified transcripts were blinded to the participant’s identities.
Constant discussion among the team members to challenge and debate the data collected and analyzed to ensure the credibility of the study findings. The study team members practiced reflexivity during the interview, data analysis, and manuscript writing through constant discussion, challenging each other’s views and reflection on the potential impact of our own biases on the research process. The study process and findings were presented to other researchers to improve dependability. Finally, a transparent audit trail facilitated the trustworthiness of the data collected. 24
Data Analysis
Audio recordings of the IDIs were transcribed verbatim by independent transcribers and audited for accuracy by independent study team members. Three researchers independently coded the first 3 transcripts to generate an initial coding framework using the NVivo© software. This framework was subsequently modified through discussions before the remaining transcripts were coded. The identified themes and codes were reviewed and refined, with any disagreements resolved before they were finalized. Data saturation was attained when no new codes surfaced.
Definition of Previously Identified and New Barriers
The systematic review by Khatib et al 7 provided the basis for the previously identified barriers to hypertension management. Among the barriers identified, the list was curated and contextualized to Singapore’s primary care setting through consensus among clinical experts and clinical providers familiar with the local primary care context. New barriers were defined as those not previously identified by the systematic review. Examples of previously identified barriers can be found in the introduction.
Results
A total of 19 eligible PCPs were approached, with 17 agreeing to participate in the study (response rate 89.5%). The demographic information can be found in Table 1.
Characteristics of Participating Primary Care Physicians.

Abbreviation: FCFPS, fellowship of the college of family physicians Singapore.
Table 2 illustrates how thematic analysis was performed for a sample theme.
Sample Thematic Analysis.

The barriers PCPs face in managing patients with hypertension are summarized into 4 themes: patient, physician, drug, and system factors (Figure 1). The barriers were further divided into “previously identified” and “new” barriers.
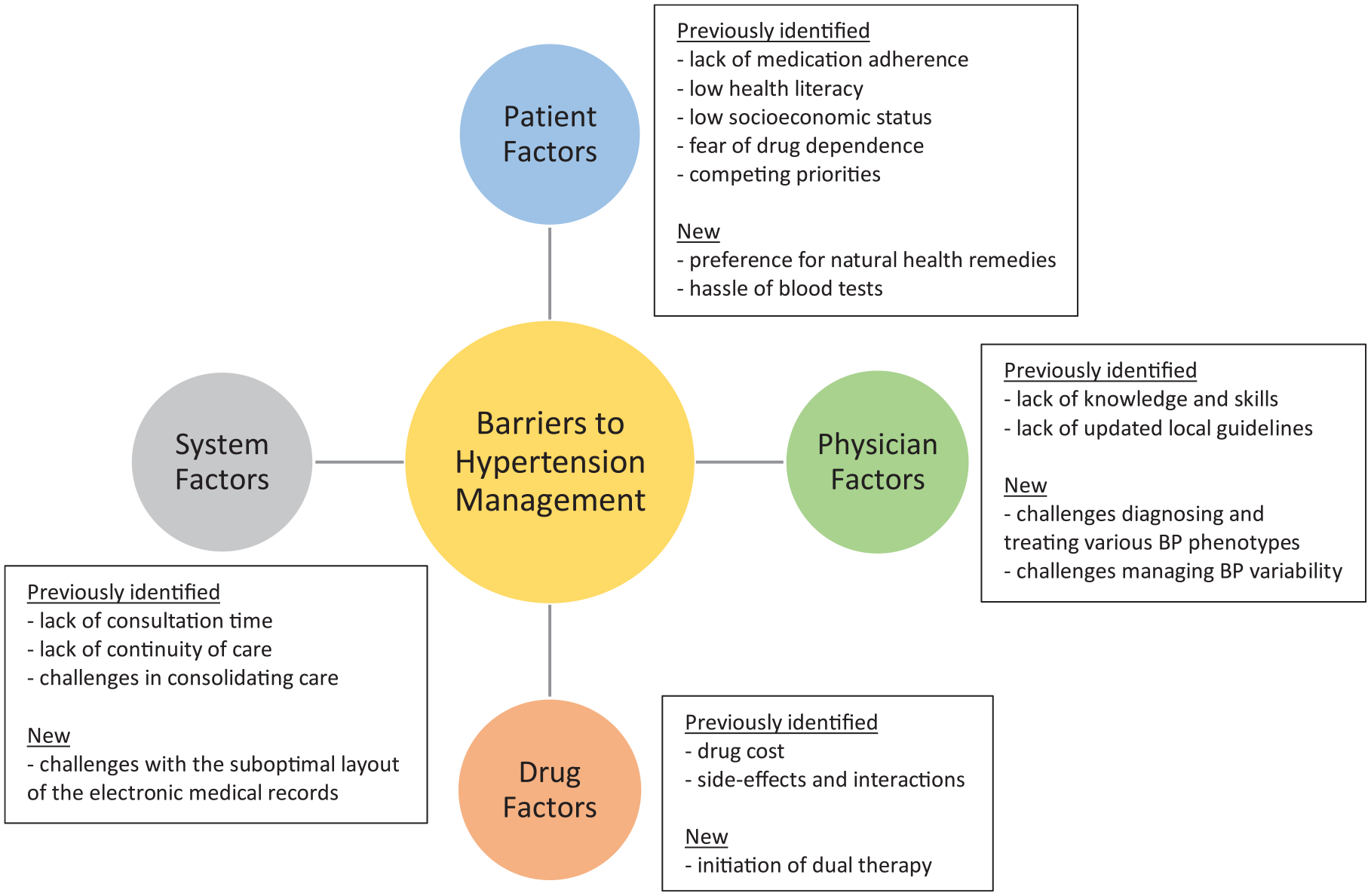
Barriers to hypertension management.
The previously identified barriers with selected codes are summarized in Table 3. References supporting each barrier code are included in parentheses. The new barriers that emerged from the interviews are presented here.
Previously Identified Challenges Faced by PCPs in the Management of Patients With Hypertension.

Patient Factors
Preference for Natural Health Remedies
Some PCPs encountered patients with hypertension who preferred natural health remedies instead of prescribed medications due to safety concerns.
TCM (Traditional Chinese Medicine) is one common example. They will say, “No, I don’t want to take all these medications, all these chemicals. I’d rather take TCM because it’s natural, it’s herbs.” P15 [Family Physician (GDFM) with six years of experience]
Inconvenience of Blood Tests
PCPs found it challenging to initiate and titrate BP medications (eg, angiotensin-converting enzyme inhibitors [ACEi] and angiotensin II receptor blockers [ARB]) due to patients having to return frequently for blood tests and doctor visits.
I guess for the patient, the trouble is I come and see you, then you say my blood pressure is not so good. Then you adjust my medication, but because you adjust my medication, you have to come back in two weeks to do a blood test. Do your blood test already (and) after one week have to come back to see the doctor again. So let’s say you see the doctor again (and) your kidney function is OK, but your blood pressure is still no good. So you increase (medication) again, and this cycle repeats. So this actually creates a lot of trouble for people who are working especially. P11 [Family Physician (GDFM) with three years of experience]
Physician Factors
Challenges in Diagnosing and Treating Various BP Phenotypes
PCPs faced challenges diagnosing and treating patients with BP phenotypes, such as masked and isolated diastolic hypertension, resulting in missed diagnoses and potentially suboptimal care.
Ya, and also for those who have masked hypertension, they can have very good blood pressure in clinics right, but they might have end-organ damage and that could be because their home BP (readings) are very elevated, but we don’t know. P07 [Associate Consultant with 11 years of experience] Personally, I think it is very hard to treat diastolic hypertension. I really don’t know how to. . . P06 [Family Physician (MMed) with five years of experience]
Challenges Managing BP Variability
Some PCPs also voiced difficulties in managing patients with labile BP due to the risk of iatrogenic complications.
When they have very wide-ranging blood pressures, we cannot base it on just one reading. If they have a nocturnal dip, sometimes we miss that. Then, when they come to see us in the day, the blood pressure is very high, so we just keep up-titrating (their medications). So they can get hypotensive and fall at night. P07 [Associate Consultant with 11 years of experience]
Drug Factors
Initiation of Dual Therapy
Some PCPs expressed their preference not to start dual therapy for patients with hypertension due to concerns over the development of side effects and being unable to discern the causative drug.
I generally don’t do that (start two drugs at once). Because if you use one calcium channel blocker, the other will be something that you know either causes electrolyte disturbances or some other things. So I don’t like to start two because if the patients develop some side effect, it is a bit hard to determine. . . is it this drug or that drug. P15 [Family Physician (GDFM) with six years of experience]
System Factors
Challenges With the Suboptimal Layout of Electronic Medical Records
The suboptimal layout of the EMR impeded PCPs from easily accessing the relevant healthcare details necessary to provide optimal hypertension care.
I feel that the way the information is presented to you can be improved. P15 [Family Physician (GDFM) with six years of experience]
Discussion
The study revealed previously identified and new challenges to providing care for patients with hypertension. The themes labeled as previously identified themes were consistent with those identified in the literature review. The new themes identified add to the existing literature and provide further insights into barriers faced by PCPs when managing patients with hypertension, encompassing patient, physician, drug, and system-related factors.
PCPs reported that patients preferred natural health remedies, such as traditional Chinese medicine (TCM), due to concerns over the safety of harmful chemical-containing Western medications. A Chinese study showed that up to one-third of participants used TCM for chronic disease management. 33 The preference for herbal remedies is not unique to Asia but is also observed in the West. A German study found that some patients preferred these remedies due to dissatisfaction with conventional medication and doctors. 34 However, most PCPs lack knowledge of complementary and alternative medicine (CAM) 35 ; in contrast, patients expect PCPs to possess this knowledge. 36 Al-Rowais et al 35 found that 85% of PCPs desired CAM knowledge. The lack of awareness has the potential to erode the therapeutic doctor-patient relationship. Improving PCP understanding of CAM could facilitate a more meaningful discourse with patients in their chronic disease management. 37 Awareness of this barrier may provide PCPs with insight into patients’ concerns regarding using Western medications and encourage CAM knowledge acquisition to better address patients’ misconceptions surrounding conventional pharmacological therapy.
Additionally, PCPs expressed the inconvenience of repeat blood tests and physician reviews imposed on patients when initiating and titrating anti-hypertensives as a barrier to optimizing hypertension management. Patients started on agents such as ACEi and ARB require blood tests to assess for known complications such as hyperkalemia and acute renal impairment.38,39 Physicians are also advised to repeat these tests with subsequent dose titrations, with the recommended interval being within 2 weeks. 33 The European Society of Cardiology also recommends ACEi and ARB as first-line agents for patients suffering from hypertension with comorbidities such as heart failure and nephropathy. 40 The need for multiple cycles of repeat tests potentially discourages patients from agreeing to have these agents started or adjusted. Strategies to mitigate this inconvenience could involve using scores to determine an individual patient’s susceptibility to hyperkalemia and facilitate an electrolyte monitoring regime that is more agreeable for the patient without compromising patient safety.41,42 Bandak et al 41 developed and validated a score to estimate an individual’s likelihood of developing hyperkalemia following ACEi or ARB initiation based on 6 commonly available clinical characteristics. Implementing simple scoring tools could help to risk-stratify individuals at increased risk of biochemical abnormalities. Such an approach could facilitate an individualized recommended interval for subsequent blood tests and doctor review, thereby reducing patient inconvenience and alleviating PCP apprehension around initiating or titrating ACEi and ARB.
Despite the diagnostic and monitoring recommendations for different hypertension phenotypes by the latest CPGs, the management remains unclear and awaits the outcome of definitive trials.2,40 PCPs expressed physician-related challenges in diagnosing and treating various BP phenotypes and managing BP variability. The interviewed PCPs expressed concerns that conditions such as masked hypertension were missed due to the lack of insight regarding the patient’s home BP. Similarly, physicians from other studies shared this difficulty and expressed concerns as individuals with masked hypertension are at increased risk of strokes. 43 A recent US study showed that only 55% of patients with hypertension owned a home BP machine, with approximately half reporting that they monitored their home BP regularly. 44 In addition to challenges in diagnosing certain BP phenotypes, PCPs also expressed difficulty treating phenotypes such as isolated diastolic hypertension. The matter is further compounded by the absence of local and international guidelines on treatment recommendations for isolated diastolic hypertension.2,40 Currently, the literature is divided regarding the need to treat isolated diastolic hypertension, with studies showing the absence of target organ damage and concerns surrounding treatment-induced systolic hypotension.45,46 Finally, PCPs found it challenging to manage patients with substantial variability in BP readings as it limited their ability to titrate their medication regime owing to a concern in causing iatrogenic complications. Ambulatory BP monitoring (ABPM) may better inform the patient and support PCP in tailoring a suitable treatment regime, especially in elderly patients due to their increased risk of exaggerated BP variability, morning surge, postural, or postprandial hypotension. 47 Unfortunately, despite the importance of ABPM, its access in the primary care setting remains limited, highlighting the mismatch between CPG recommendations and daily clinical practice. 20
The initiation of dual therapy was a new drug-related theme that emerged. PCPs expressed reluctance to initiate dual therapy in patients despite the American College of Cardiology and American Heart Association guidelines recommending that patients with more severe hypertension should be initiated with 2 low-dose anti-hypertensive drugs concurrently to control BP adequately. 2 They expressed concerns regarding potential drug side effects and the inability to discern the offending drug if 2 agents were prescribed concurrently. A feared downstream consequence is the potential deterioration of the therapeutic doctor-patient relationship stemming from possible medication-related side effects. Single pill combinations could provide a potential solution for patients requiring the initiation of 2 concurrent anti-hypertensives. A meta-analysis by Parati et al 48 found that patients are more likely to adhere to and persist with single pill combinations instead of their free equivalent combinations.
System-related themes such as challenges with the electronic medical records (EMR) layout impeded PCPs from optimal care delivery. The issues PCPs raised regarding the presentation of the information that affected a patient’s BP target affected their ability to identify and prioritize treatment goals. PCPs have to navigate the EMR to locate data such as recent laboratory investigations and the presence of comorbidities, which dictate the recommended therapeutic BP targets.2,40 The importance of equipping PCPs with tools to facilitate hypertension management cannot be understated, as it has been shown to improve the quality and efficiency of care. 49 Involving the end users in the selection, design and optimization of the EMR is crucial to improve ownership and usability, thereby facilitating achieving the intended treatment goals. 50
Strength and Limitations
The strength of this study is the pool of PCPs interviewed, evidenced by the comprehensive themes and codes derived as corroborated by the presence of previously identified barriers to hypertension management. In addition to identifying the previously identified barriers, the study also yielded new barriers to hypertension management that could be valuable to improving the provision of hypertension care in the primary care setting.
A study limitation was the lack of representation of PCPs practicing in the private healthcare sector. The resources available to PCPs in public practice may differ from those in the private sector and could translate into differences in the challenges faced. The decision was made to recruit only public PCPs because most patients with non-communicable diseases, such as hypertension, are managed in the public primary care setting. In contrast, private PCPs mainly provide acute, dermatological, or esthetic care.
The study findings did not capture patients’ perspectives, an important factor influencing PCP practice. We are currently conducting a study to explore the experiences and challenges faced by patients with hypertension to better understand how to provide optimal care.
Conclusion
This study highlights new challenges to hypertension care faced by primary care doctors in a well-resourced healthcare system. There is a need to empower patients and minimize the inconvenience of medication adjustments. Clinical guidelines must provide practical guidance to support PCPs in caring for patients with challenging BP phenotypes. Improved access to combination pills and an optimized EMR could improve care for patients with hypertension in primary care. Future studies exploring the perspective of patients with hypertension could provide further insights into how hypertension care can be optimized.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241291466 – Supplemental material for Exploring the Challenges Faced by Primary Care Physicians in Providing Optimal Care for Patients With Hypertension: A Qualitative Study
Supplemental material, sj-docx-1-jpc-10.1177_21501319241291466 for Exploring the Challenges Faced by Primary Care Physicians in Providing Optimal Care for Patients With Hypertension: A Qualitative Study by Prawira Oka, Aminath Shiwaza Moosa and Chirk Jenn Ng in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The authors would like to thank the polyclinics and primary care physicians who participated in the study.
Author Contributions
CJN conceptualized the study and conducted the IDIs. All authors checked the transcripts and performed thematic analysis. PO drafted the manuscript. All authors reviewed and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is supported by SingHealth AM General Fund (14/FY2021/G2/01- A167), SingHealth Polyclinics and Duke-NUS Medical School.
Ethical Approval
The study was approved by the SingHealth Centralised Institutional Review Board (CIRB No: 2022/2517) on 30 March 2022.
Data Availability Statement
The full interview guide and codebook generated during analyses can be found in the Supplemental Appendix. The interview transcripts generated and analyzed during this study are not publicly available due to their containing information that could compromise research participants’ privacy/consent.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.