
Abstract
Background:
Public health literacy (PHL) is a novel perspective on health literacy (HL). Differing from HL’s individualist approach, PHL is concerned with public health events and promoting health in the whole society.
Objectives:
To evaluate PHL, a newly developed concept, and related factors.
Methods:
In this cross-sectional study, people who visited primary healthcare centers in urban and rural settings were recruited using a questionnaire that includes Public Health Literacy Knowledge Scale (PHLKS) and Adult Health Literacy Scale (AHLS). Out of four Primary Healthcare Centers (PMCs) in western Turkey selected randomly, one PMC was located in a rural setting, while three PMCs were located in an urban setting. Multiple linear regression was used to determine the predictors for PHL.
Results:
The study group consisted of 1672 people, of which 55.3% were male. The mean age was 40.94 ± 15.22. The median score (min–max) from PHLKS was 13.0 (0–17). Multiple linear regression showed that income level had a negative impact on PHL. Higher education, fondness for reading, hospital admission and HL, however, increased PHL levels. Additionally, living in an urban area and not having auditory problems were positively associated with PHL.
Conclusions:
Participants had a moderate level of PHL. Improving PHL should be a priority to tackle global and local problems that have an adverse effect on community health. To increase community engagement in public health events, people with low education and HL levels should be targeted in future training programs.
Introduction
Simonds (1) first brought about health literacy (HL) in 1974. With time, plenty of different definitions and concepts for HL have evolved and, in 1998, Nutbeam and Kickbusch defined HL as: ‘The achievement of a level of knowledge, personal skills, and confidence to take action to improve personal and community health by changing personal lifestyles and living conditions. Thus, health literacy means more than reading pamphlets and making appointments. By improving people’s access to health information, and their capacity to use it effectively, health literacy is critical to empowerment’ (2).
Two years later, Nutbeam theorized a modeling of HL with three levels: functional HL, interactive HL and critical HL. Nutbeam discussed that all three levels of HL will provide community/social benefit such as increased participation in public health programs, positive influence on social norms and increased community engagement on top of individual benefits. Thus, he concluded that HL is a public health goal and plays a key role in promoting health (3).
Many public health authorities also had the same idea and took action. Gazmararian et al. (4) argued that being public health literate is an ethical imperative and that those who are public health literate are better at assessing the impact of health events on themselves, those around them and society. Freedman and colleagues also stated that ‘public health literacy’ (PHL) should be separated from HL and defined it as ‘The degree to which individuals and groups can obtain, process, understand, evaluate, and act upon information needed to make public health decisions that benefit the community’. It was also stated that the target of the PHL is not the individuals but the public, thus improving the community health instead of individual health. The authors also claimed that the primary object of PHL is to make more stakeholders engage in public health efforts and address the social and environmental determinants of health as opposed to the aim of HL, which is to enhance health communication between individuals and authorities as well as encouraging healthy lifestyle behaviors (5).
After the difference between PHL and HL has become evident, the need to develop measurement tools to assess the PHL levels of the public has arisen. Using the joint publication of ‘Facts for Life’ with the partnership of international organizations, Pleasant and Kuruvilla (6) developed the Public Health Literacy Knowledge Scale (PHLKS) and paved the way for PHL evaluation. The scale, following the footsteps of many before it, such as Test of Functional Health Literacy for Adults (TOFHLA) and Rapid Estimate of Adult Literacy in Medicine (REALM), approaches HL from a functional perspective (7,8). Yet they differ from each other as HL scales aim to measure the knowledge on health information while PHLKS’s goal is to assess the knowledge regarding the events affecting public health ranging from environmental problems to the spread of infectious diseases in a community setting.
Today, humanity faces dire public health threats such as climate change, armed conflicts, emerging and re-emerging infectious diseases, and pandemics. The successful collective response from humankind against such dangers is dependent on how well versed the public is. Although Sørensen et al. (9) conceptualized the benefits of increased HL with health care/disease prevention/health promotion domains, broader result could be achieved with an increase in PHL. For the healthcare domain, high PHL levels could equip the public with rapid response capabilities, reducing the burden on health care systems; for the disease prevention domain, it could lead to more people involved with infectious disease control policies halting the spread, and for the health promotion domain, it could create public engagement in local and national policy-making for a healthier society (4).
As PHL is a new concept developed recently, the literature on the subject is scarce. Therefore, it is vital to assess the PHL levels of the community and the factors affecting it, in both urban and rural settings. Our study is original in that to our knowledge this is the first study that aimed to evaluate PHL in different residential settings as well as the factors related to it. Due to the lack of studies on PHL, we have used variables established to have a relationship with HL in the literature, such as sociodemographic factors, lifestyle choices and general health status (10,11).
In the study, we sought to assess the degree of knowledge on PHL, its relationship to HL, and identify the factors associated with it in a western city’s urban and rural regions of Turkey, a developing country. We also wanted to determine where the public typically goes for health information.
Materials and methods
Study design and sampling
This cross-sectional study was conducted on 1672 people aged 18 or over who applied to primary healthcare centers (PHCs) between 1 July and 31 December 2019 in Eskişehir province, located in the Central Anatolia Region, neighboring the capital city Ankara. The aim of the PHCs is to provide the registered population with preventive healthcare, early detection and screenings for various diseases and outpatient diagnostic and treatment services. At least one doctor and a nurse are responsible for the duties of a PHC. The study was carried out in four different PHCs; one from the rural district and three from the urban districts, which were drawn by lot. While the three urban PHCs included in the study were in Eskişehir, the rural PHC was located in Beylikova, 77 km from the center. The population of Eskişehir is 887,475 while Beylikova has a population of 5781. In Eskişehir city center, there are 243 PHCs and in Beylikova there are three PHCs. While the main source of income in the city center is the service sector and industrial jobs, it is agriculture in Beylikova.
The sample size was calculated with the unknown population size formula. Convenience sampling method, one of the non-probabilistic approaches, was used in the study. The sample size was 384 when the PHL level was accepted as 50%, the error margin as 5% and the confidence interval as 95% (12). For every PHC, 384 people were calculated to be reached; therefore final minimum sample size was 1536.
Permissions
The ethical approval was obtained from Eskisehir Osmangazi University’s non-interventional clinical trials committee with the decision numbered 25403353-050-E.76039 and dated 25.06.2019.
Administrative permissions were acquired from Eskişehir Provincial Health Directorate and the selected PHCs.
Study procedure and data collection
A questionnaire was prepared for data collection based on the relevant literature on PHL (4–6). The first part of the questionnaire form included some sociodemographic variables such as age, sex, marital status, income status, et cetera, and factors thought to be related to PHL such as education level, their source for information on health, smoking, alcohol consumption, et cetera, and the second part of the questionnaire consisted of the PHLKS and the Adult Health Literacy Scale (AHLS).
Pleasant and Kuruvilla developed the PHLKS in 2008. It is a 17-item self-administered scale evaluating people’s basic knowledge on public health, hygiene, infectious diseases, air pollution, et cetera. The items are either ‘True’ or ‘False’ and the scores obtained from the scale range from 0 to 17, where every correct answer is one point. The scale is evaluated over a total score, where a higher score implies higher PHL knowledge (6). The PHLKS was adapted to Turkish by Arikan and Tekin (13) and was found valid and reliable. In our study, the Cronbach’s alpha value was 0.72.
Sezer and Kadioglu developed the Adult Health Literacy Scale (AHLS) in 2014 to evaluate the HL levels. The scale consists of 13 yes or no, 4 fill-in-the-blank, four multiple-choice, and two matching questions. The scores from the AHLS range from 0 to 23, and a high score means higher literacy (14). The scale had a good internal consistency, with a Cronbach’s alpha of 0.77 in this study.
After obtaining the necessary permissions, the researchers started to collect data by reaching out to individuals who volunteered to participate in the research after receiving information about the purpose and concept of the study. The pre-prepared questionnaire form was then given to the participants who completed it under the researchers’ observation. The researchers helped to fill in the questionnaire forms in place of volunteers who could not read or see well. The data collection lasted for five weeks between 29 July and 30 August. Every workday, researchers recruited participants from 8AM to 5PM. Since researchers were always present during the data collection, there were no missing data in the study. Per the personal data protection law of Turkey, no data were collected that could be used to identify the participants and only the research team has access to data, which will be deleted after 10 years.
According to their perception, the participants’ income level was evaluated as low, medium, or high. Those who smoked at least one cigarette a day were considered ‘smoker’ and those who consumed alcohol at least once a week were considered ‘alcohol drinker’. Participants who claimed they exercise five days a week and 30 min a day were accepted as ‘regularly exercising’. The body mass index was calculated with the formula weight (kg)/height squared (m²) using the self-reports of the volunteers.
Statistics
The data were evaluated using the IBM SPSS statistical package program (Version 15.0). The study used the Shapiro–Wilk normality test, descriptive analysis, Mann–Whitney U test, Kruskal–Wallis test, Spearman correlation analysis, and multiple linear regression analysis. As the scores obtained from PHLKS and AHLS did not distribute normally, logarithm base 10 was taken. Then, a three-level hierarchical multiple linear regression was performed with variables considered to be confounders and adjusted accordingly with 95% confidence intervals. The confounding factors were selected on the principle that was laid out by VanderWeele (15). For the confounding variables that were neither continuous nor dichotomous, dummy variables were employed. In the first step, sociodemographic factors, the second step, lifestyle choices, and in the last step, variables regarding medical history and scores taken from AHLS were included in the multiple regression analysis. A statistical significance value of p ⩽ 0.05 was accepted.
Results
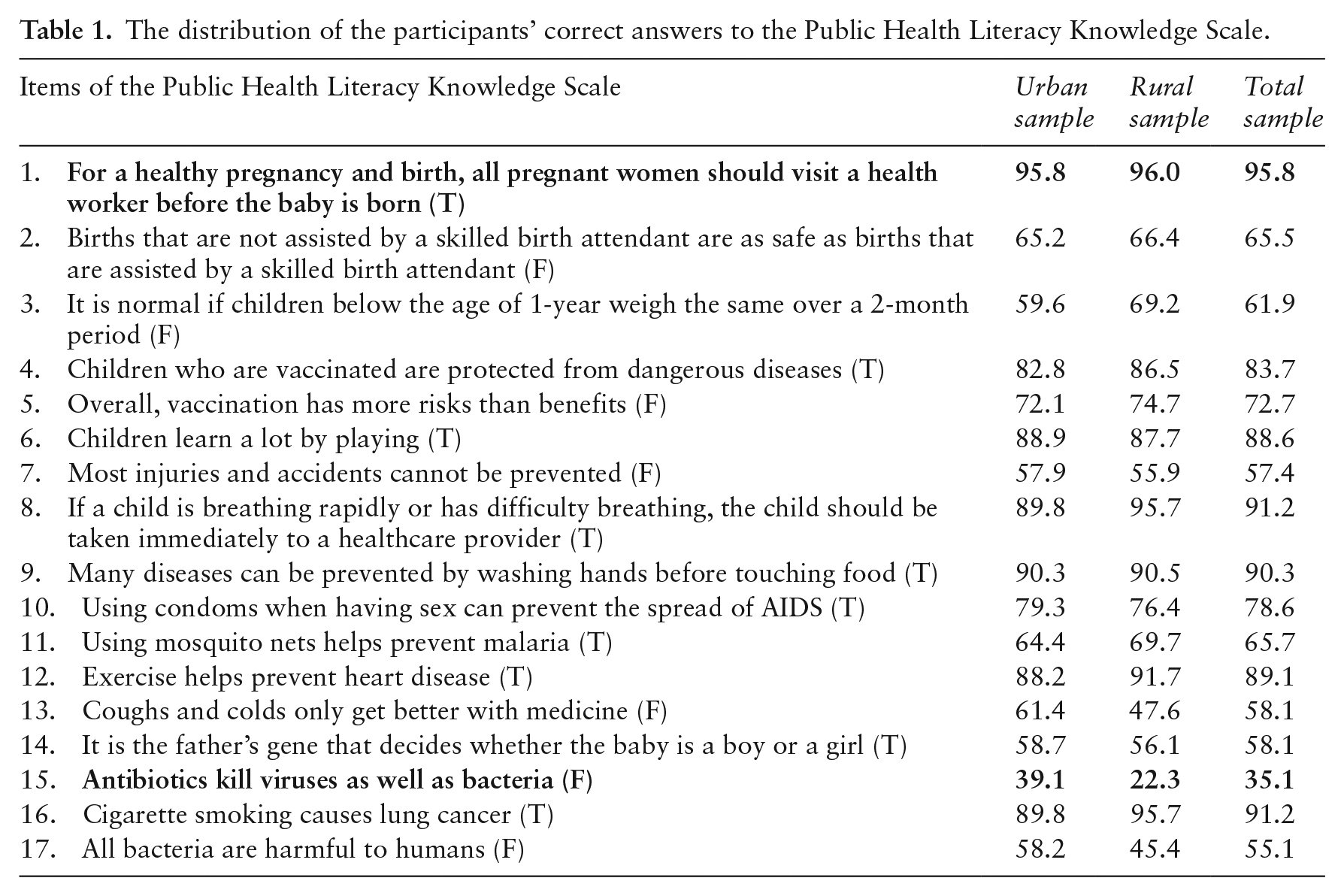
The study included 1672 individuals; 924 (55.3%) were male and 748 (44.7%) were female. The study group’s mean age ± SD (min–max) was 40.94 ± 15.22 (18–87) years. The scores taken from PHLKS ranged from 0 to 17, and the mean score was 12.38 ± 2.99 (median: 13.0). While the statement ‘For a healthy pregnancy and birth, all pregnant women should visit a health worker before the baby is born’ was the most correctly answered item with 95.8%; the statement ‘Antibiotics kill viruses as well as bacteria’ had the lowest correct answer rate, with only 35.1%. The distribution of the participants’ answers to PHLKS is shown in Table 1.
The distribution of the participants’ correct answers to the Public Health Literacy Knowledge Scale.
In the study group, being younger, married and having a higher education was associated with high PHLKS levels while having a low income and being unemployed were associated with lower scores from PHLKS. The distribution of the scores obtained from PHLKS according to some sociodemographic variables is shown in Table 2.
The distribution of the scores obtained from the Public Health Literacy Knowledge Scale (PHLKS) according to some sociodemographic variables.
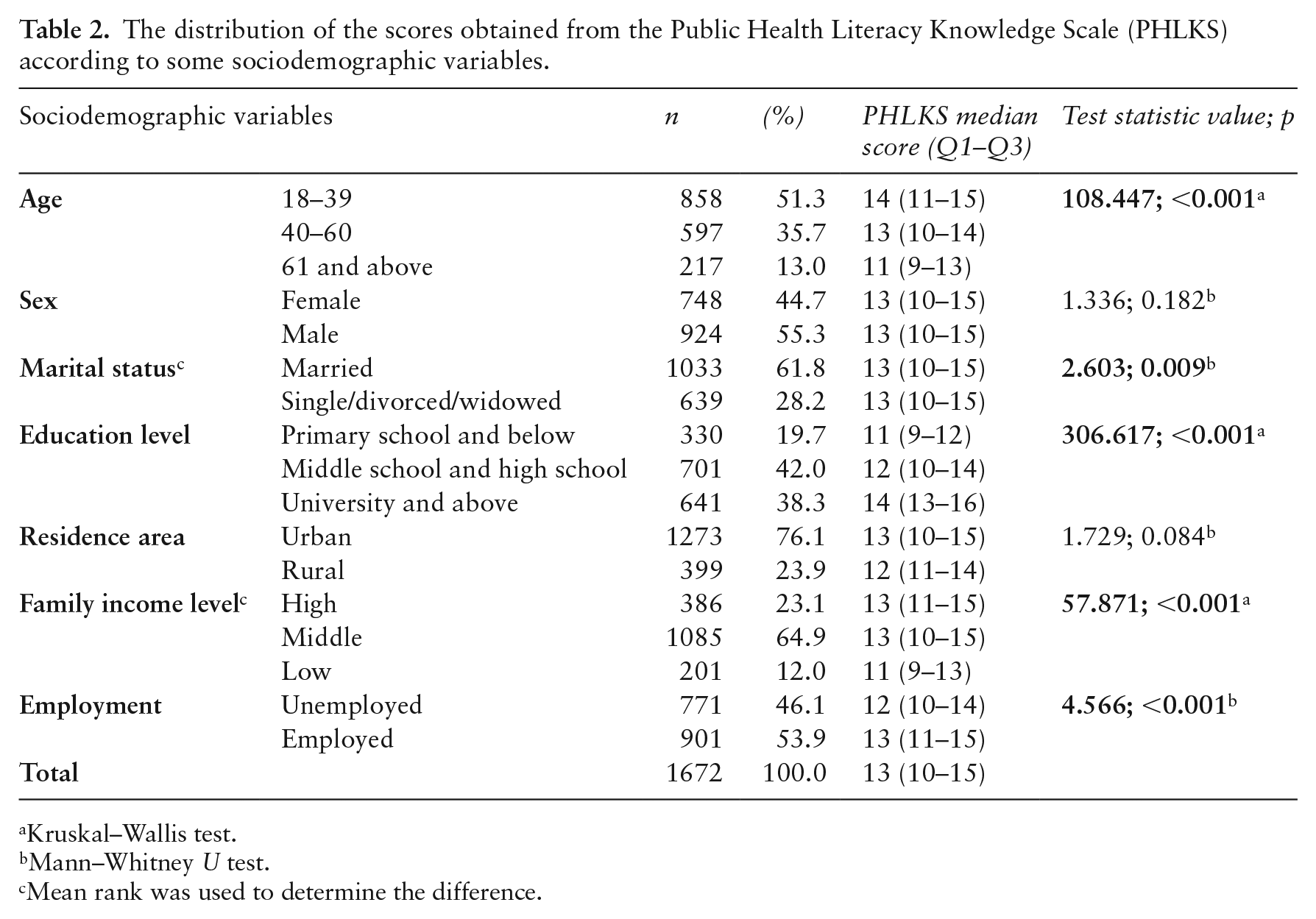
Kruskal–Wallis test.
Mann–Whitney U test.
Mean rank was used to determine the difference.
In the study group, those who were non-obese, did not smoke, claimed they regularly exercise and did not have a chronic disease scored higher on the PHLKS. On the other hand, those who were admitted to a hospital at least four times, those who were hospitalized, and those with visual and auditory problems had a lower PHL knowledge level. It was found that, as the general perception of self-health and the fondness for books/newspapers/magazines increases, the scores taken from PHLKS also increase. The distribution of some variables regarding PHLKS scores has been shown in Table 3.
The distribution of scores taken from public health literacy knowledge scores according to some related variables.
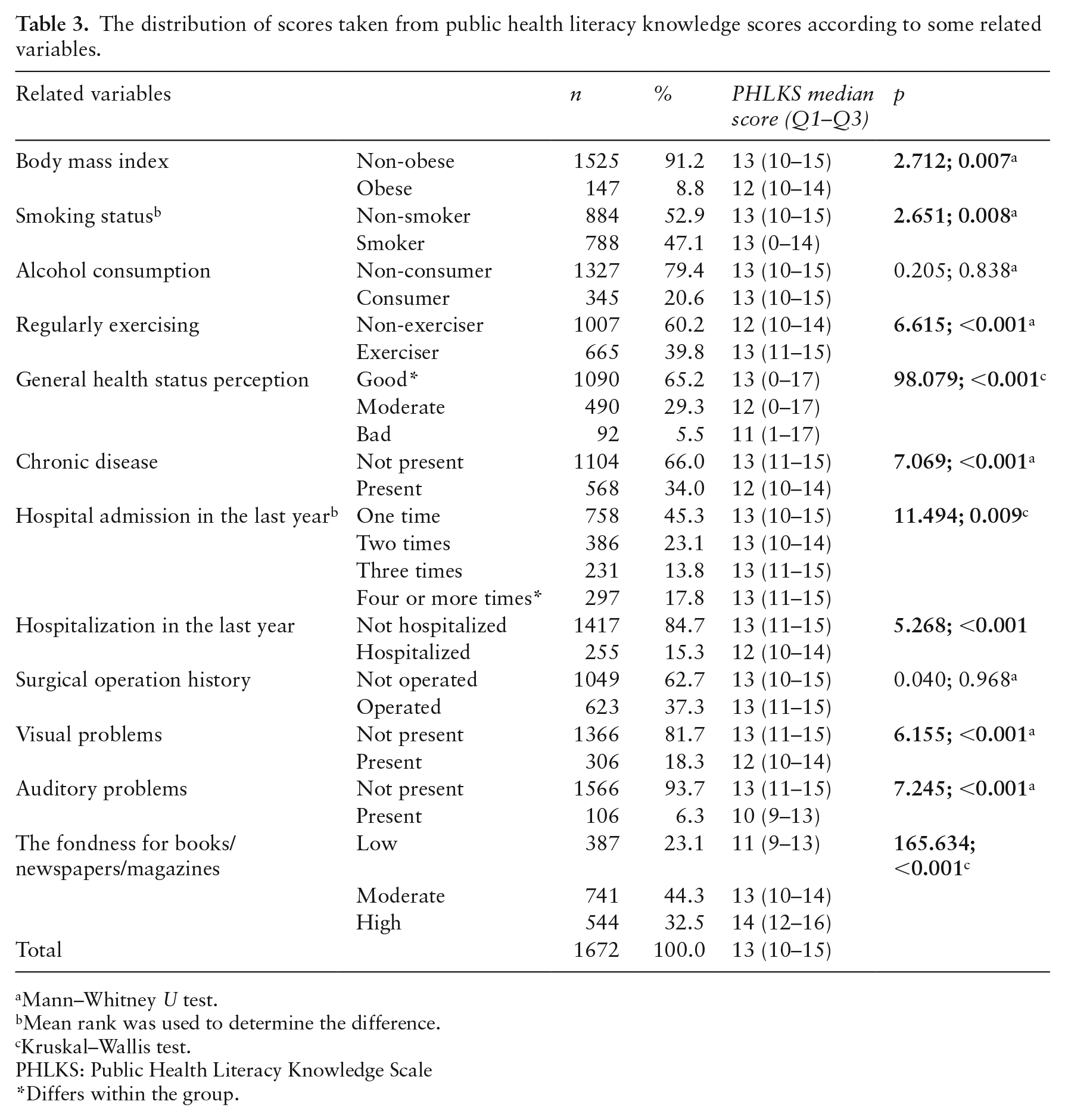
Mann–Whitney U test.
Mean rank was used to determine the difference.
Kruskal–Wallis test.
PHLKS: Public Health Literacy Knowledge Scale
Differs within the group.
Among the participants, the most common usual information source regarding health was health professionals, with 58.79%, followed by newspapers/television. Figure 1 shows the distribution of the usual source for health information.
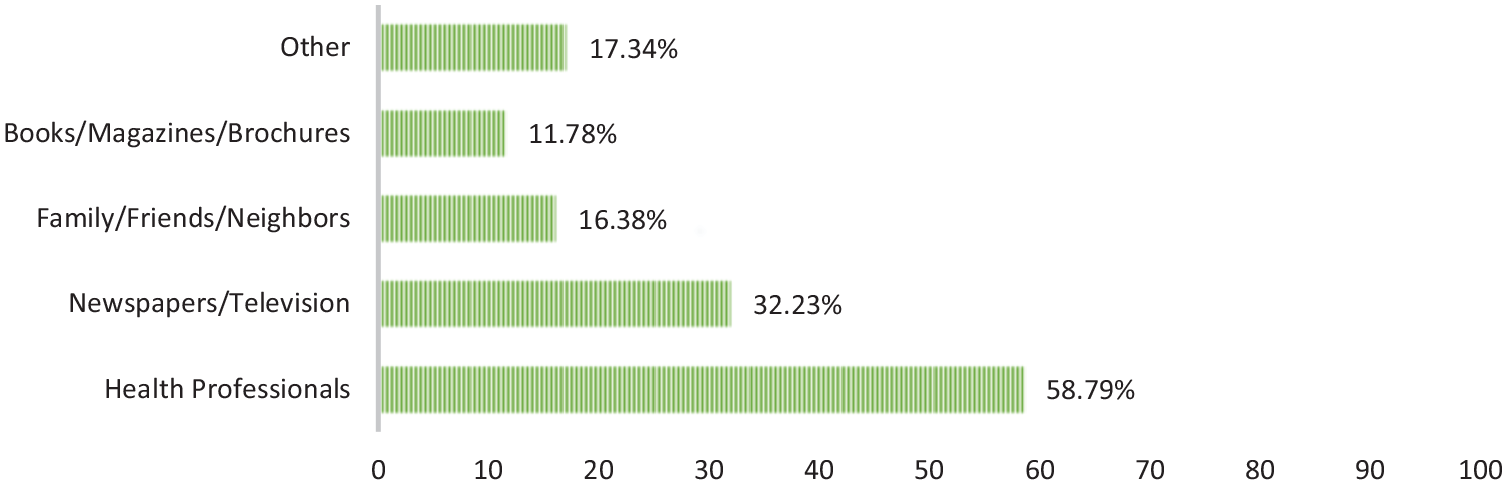
Distribution of the usual source for information regarding health.
The study participants scored between 0 and 23 on the AHLS; the mean score was 12.69 ± 0.10 and the median score was 13.0. Spearman correlation analysis to assess the relationship between PHLKS and AHLS showed a positive moderate correlation (r = 0.586, p < 0.001). The relationship between PHL knowledge and adult HL is shown in Figure 2.
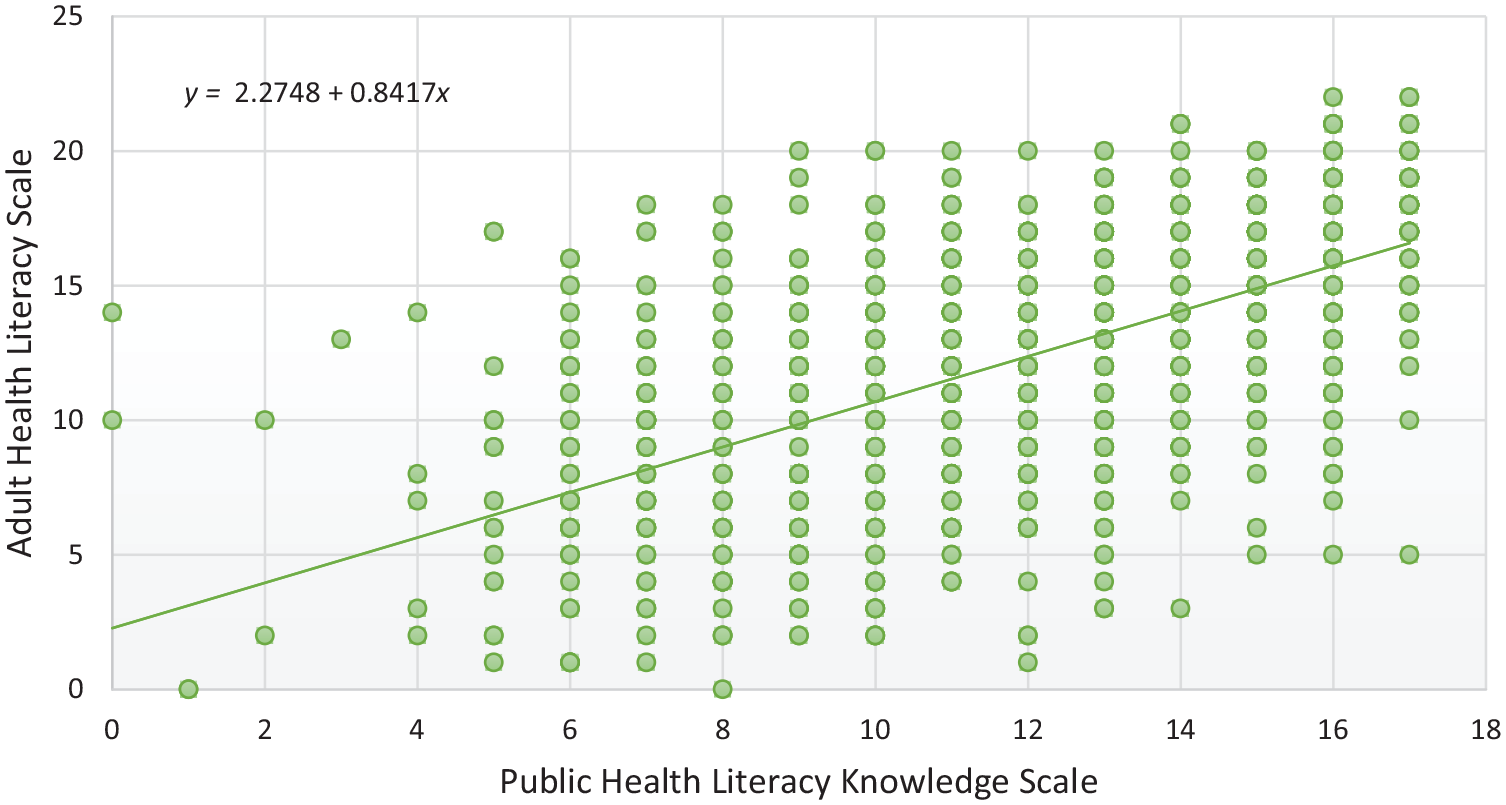
The scatter plot of adult health literacy and public health literacy knowledge.
The regression analysis showed that income level, education level, fondness for reading, area of residence, auditory problems, the number of hospital admissions and HL were still significant factors in the last model after controlling for other variables (R² = 0.342, F = 37.003, p < 0.001). The multiple linear regression analysis results of the related factors are given in Table 4.
The results of the multiple linear regression analysis of the related factors.
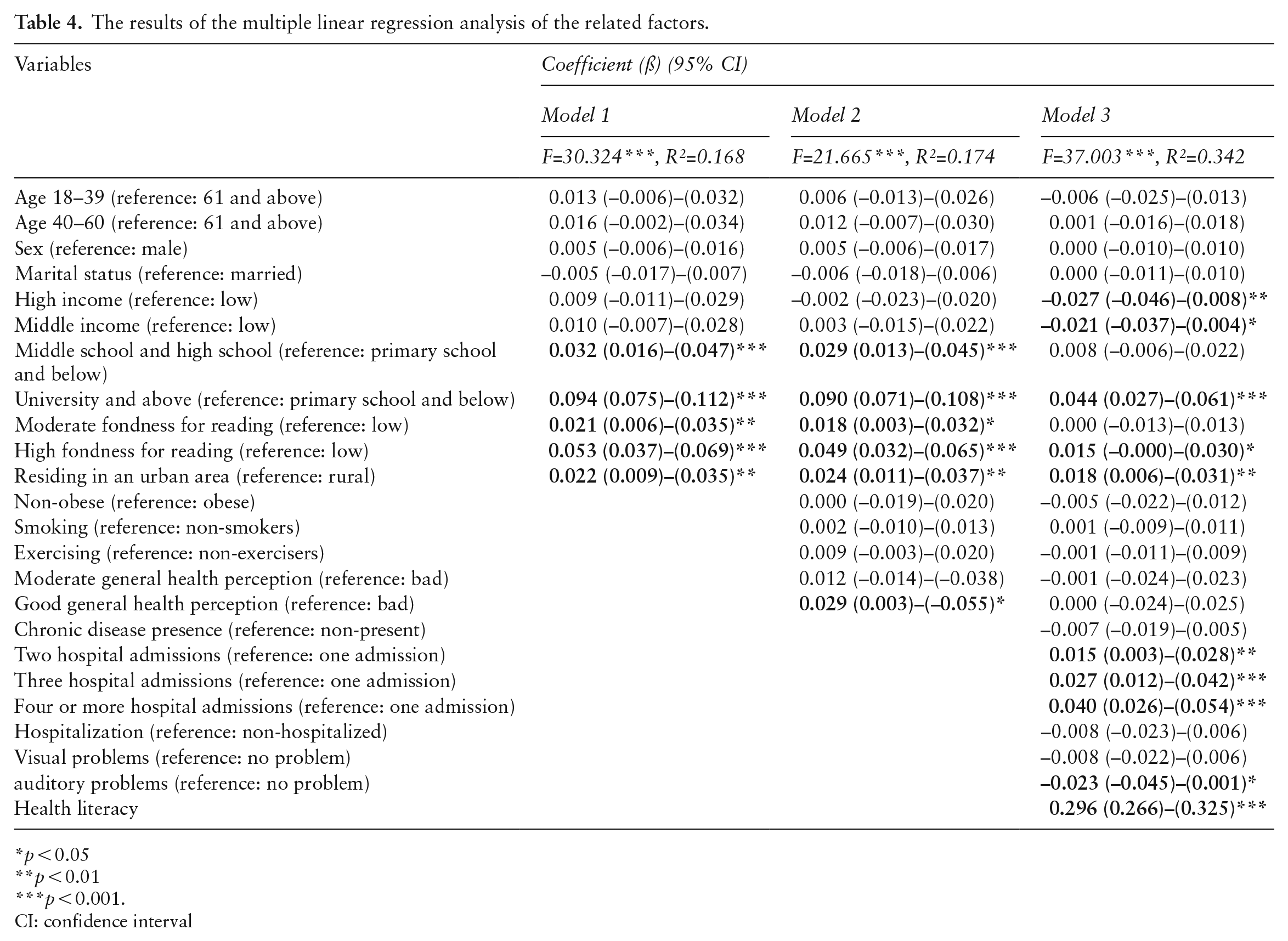
p < 0.05
p < 0.01
p < 0.001.
CI: confidence interval
Discussion
It is hard to achieve a health-literate public where individuals can assess their health and act accordingly. Even after it is defined as a major public health issue, HL levels have stagnated (16,17). On the other hand, a high PHL is an even more challenging feat for the public health authorities since it requires proficiency in HL and a broader understanding of the social, environmental and systemic forces (5). One of the first steps in tackling this obstacle includes measuring the PHL levels of the population, as suggested by Gazmararian et al. (4). In our study, the participants were found to have a moderate knowledge level of PHL. Similar results have been reported in other studies (6,13).
In the study, four questions had a correct response rate of over 90%, similar to Pleasant and Kuruvilla. However, while our study group heavily associated cigarettes with lung cancer, they reported a higher correct response rate for the item ‘Children learn a lot by playing’ (6). The reason behind the high knowledge of smoking in our study group may stem from Turkey’s successful anti-smoking campaign, which applies WHO’s MPOWER package (18).
On the other hand, ‘Antibiotics kill viruses as well as bacteria’, the 15th item on the scale, was the only statement with a correct response rate below 50%, with only 35.1% of the study group giving the correct answer. Arikan and Tekin (13) also reported less than 50% correct response rate for the same item, citing that both viruses and bacteria are considered similar microorganisms detrimental to health, thus public interpreting both as the same. In this sense, having a high level of PHL may also assist with combatting antibiotic resistance, a substantial health issue.
Aging and losing cognitive functions are significant barriers to improving HL (19). In univariate analysis, PHL decreased with age, but the significance was lost after controlling for other factors. Similarly, the literature has reported no relationship (20,21). Since HL depends on individual skills and does not rely on support from others, age may have played a more prominent role than PHL.
Many studies have investigated the impact of gender on HL and reported contrasting findings, such as higher HL for males versus higher HL for females, and the reason for this is still unclear (22,23). We found no significant difference in PHL levels for genders in the study, similar to other studies (13,20). Collins et al. (24) reported that gender does not play a role for an individual in understanding and engaging in community engagement, which may explain why gender had no impact on PHL.
Education is one of the most critical aspects of social capital, composed of social trust and participation. Thus, education may implicitly create an environment where individuals participate in community health events (25). In the study, PHL was found to increase with education level. Various studies also reported similar findings (20,26). However, in a study by Krmac et al. (21), education level was not a significant factor among public health concepts of HL. The discrepancy may have resulted from using different measurement tools.
Health literacy has a tangible impact on healthcare utilization, hospital admissions and the usage of preventive public health measures (27,28). In this study, individuals who visit hospitals more than once a year were found to have higher PHL levels. Since the study was conducted on volunteers who visited PHCs, those who visited hospitals/PHCs more often may have been represented more, thus skewing the results.
The clinical approach to HL has been the main factor driving researchers to distinguish between HL and PHL. Nevertheless, in the grand scheme of things, both are still focused on the capacity of the individual to find, understand and evaluate the information they receive. Hence the assessment of HL and PHL may as well be made conjointly (5,6). In the study, there was a positive relationship between the PHL and HL levels of the participants. Arikan and Tekin (13) also reported a correlation between PHL and HL in their study.
This study had some limitations. The cross-sectional study type limits our results in causality. As the population of this study included those who visited a PHC, it is not representative of the general public. Despite these limitations, this study is one of the first large-scale studies to assess the PHL and related factors in Turkey and may be considered a milestone for the future of public health.
Conclusion
Our study group had a moderate knowledge level of PHL. Income, education, hospital admission, area of residence, auditory problems and HL were related to PHL. Because the groups with low educational levels struggled with PHL the most, efforts to increase PHL should prioritize the individuals who did not receive higher education. Also, it should be noted that campaigns focused on clinical and individual HL may also provide insight into PHL. Population-based studies on PHL with more assessment tools and extensive samples are needed to draw definitive conclusions.
Footnotes
Author’s note
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The ethical permission was obtained from Eskişehir Osmangazi University’s non-interventional clinical trials committee in June 25th, 2019.