
Abstract
Objective:
With the rise of medical and recreational cannabis use among older adults, concerns about the potential risks and benefits of cannabis use are increasing. This pilot study aimed to determine the attitudes, beliefs, and perceptions of older adults toward cannabis as a medicinal product, to establish a foundation for future research on how healthcare providers communicate with this population regarding cannabis.
Methods:
A cross-sectional survey was conducted on adults aged 65 and older living in Philadelphia. The survey included questions related to participants’ demographics, knowledge, attitudes, beliefs, and perceptions of cannabis. Participants were recruited via flyer distributions, publications in newsletters, and a local newspaper. Surveys were conducted from December 2019 through May 2020. Quantitative data were presented using counts, mean, median, and percentages, and qualitative data were analyzed by categorizing common responses.
Results:
The study aimed to recruit 50 participants, of whom 47 met the requirements, and had their data analyzed, resulting in an average age of 71 years. The majority of participants were male (53%) and Black (64%). Seventy-six percent of participants considered cannabis a highly important treatment for older adults, and 42% considered themselves highly knowledgeable about cannabis. Over half of the participants reported being asked about tobacco (55%) or alcohol (57%) use by their PCP compared to 23% being asked about cannabis. Participants indicated that they most commonly turned to the internet and social media for information about cannabis, while only a small number mentioned relying on their primary care physician (PCP) for such information.
Discussion:
The results of this pilot study highlight the need for accurate and reliable information about cannabis for older adults and their healthcare providers. As the use of cannabis as a therapy continues to rise, it is crucial for healthcare providers to address misconceptions and encourage older adults to seek out evidence-based research. Further research is needed to explore healthcare providers’ perceptions of cannabis therapy and how they can better educate older adults.
Introduction
As older adults tend to experience a higher frequency of medical and psychiatric co-morbidities that cannot be easily managed by current treatment methods, there is a growing interest in using cannabis as a therapy for various health conditions that are prevalent in this demographic. 1 This modality is gaining momentum in the United States, with cannabis use in adults, especially those aged 65, and above, rising at a faster pace than in younger age groups.2,3 In 2006, only 0.4% of older adults self-reported using cannabis, but this number has increased to 4.2% in 2018.4,5 With the older adult population projected to double by 2050, 6 the increased legalization of cannabis in the U.S. is likely to attract even more older adult users.
Cannabis use for medical and recreational purposes continues to rise and concerns about its potential risks and benefits are also increasing.7,8 Growing evidence suggests that cannabis may have adverse effects and potential interactions with medications commonly used by older adults. 9 Moreover, most medical cannabis dispensaries do not require a licensed healthcare practitioner to assist buyers with product selection and use, which further raises concerns about the accuracy of information provided to older adults. 10 This is concerning given recent trends showing older adults’ perceptions of the risks associated with cannabis are declining,11,12 making it crucial for them to have access to accurate and reliable information.
Unfortunately, a lack of self-perceived knowledge surrounding cannabis among health professionals has been reported,13-16 and older adults may not be receiving reliable information from their healthcare providers. In fact, a survey study on breast cancer patients showed that older adults were more likely to ask their physician about cannabis compared to other age groups, 17 indicating a need for more education and information for both patients and healthcare providers.
To address this issue, we conducted a pilot study to determine the attitudes, beliefs, and perceptions of older adults toward cannabis as a medicinal product. Our aim is to establish a foundation for future research on healthcare providers’ perceptions of cannabis therapy, including how they can destigmatize it, address misconceptions, and encourage older adults to seek out evidence-based research. By providing accurate and reliable information, we hope to improve the use of cannabis as a therapy for various health conditions that are prevalent in older adults, and ultimately improve their overall quality of life.
Methods
Design
This cross-sectional survey was conducted on adults aged 65 and older who were living in Philadelphia. The survey was designed based on a previous study conducted by 1 of the authors (IWM) 18 and included questions related to the participants’ demographics, knowledge, attitudes, beliefs, and perceptions of cannabis. To ensure the face validity of the survey, it was tested among several students and older adults.
Participants were required to review and sign a consent form before proceeding with the survey. Each participant had a non-recorded 1 h interview to complete the questionnaire, which was administered by 1 of the authors. To compensate the participants for their time and effort, they received a $25 Visa gift card and a Pennsylvania (PA) Department of Health pamphlet with information on the process for obtaining medical cannabis in PA.
All materials used in this study were reviewed and approved by the Institutional Review Board (IRB) of the University of the Sciences (IRB# 1547522). A copy of the survey used is included as Supplemental Material 1.
Setting and Participants
To be eligible for the study, participants had to be 65 years or older, live in Philadelphia, and be competent to complete the interview. Due to COVID-19 restrictions, the study had to shift its recruitment strategy from senior centers in 3 zip codes in Philadelphia to flyer distribution, publications in newsletters, and a local newspaper. The sample was expanded to include all Philadelphia neighborhoods, and phone calls were used as alternatives to face-to-face interviews. The study aimed to recruit 50 participants. The sample size was chosen based on the population size of the 3 senior centers, the face-to-face nature of the intended study, and similar pilot studies’ sample sizes. Surveys were conducted from December 2019 through May 2020.
Statistical Analysis
For the analyses, quantitative data from the survey were presented using counts, mean, median, and percentages. Qualitative data were analyzed by categorizing common responses. Categories were defined by the primary author (AK) and reviewed by a co-author (AP) until a consensus was reached. As this was a descriptive study with a small number of true qualitative questions, no specific program was used, and no statistical tests were conducted.
Results
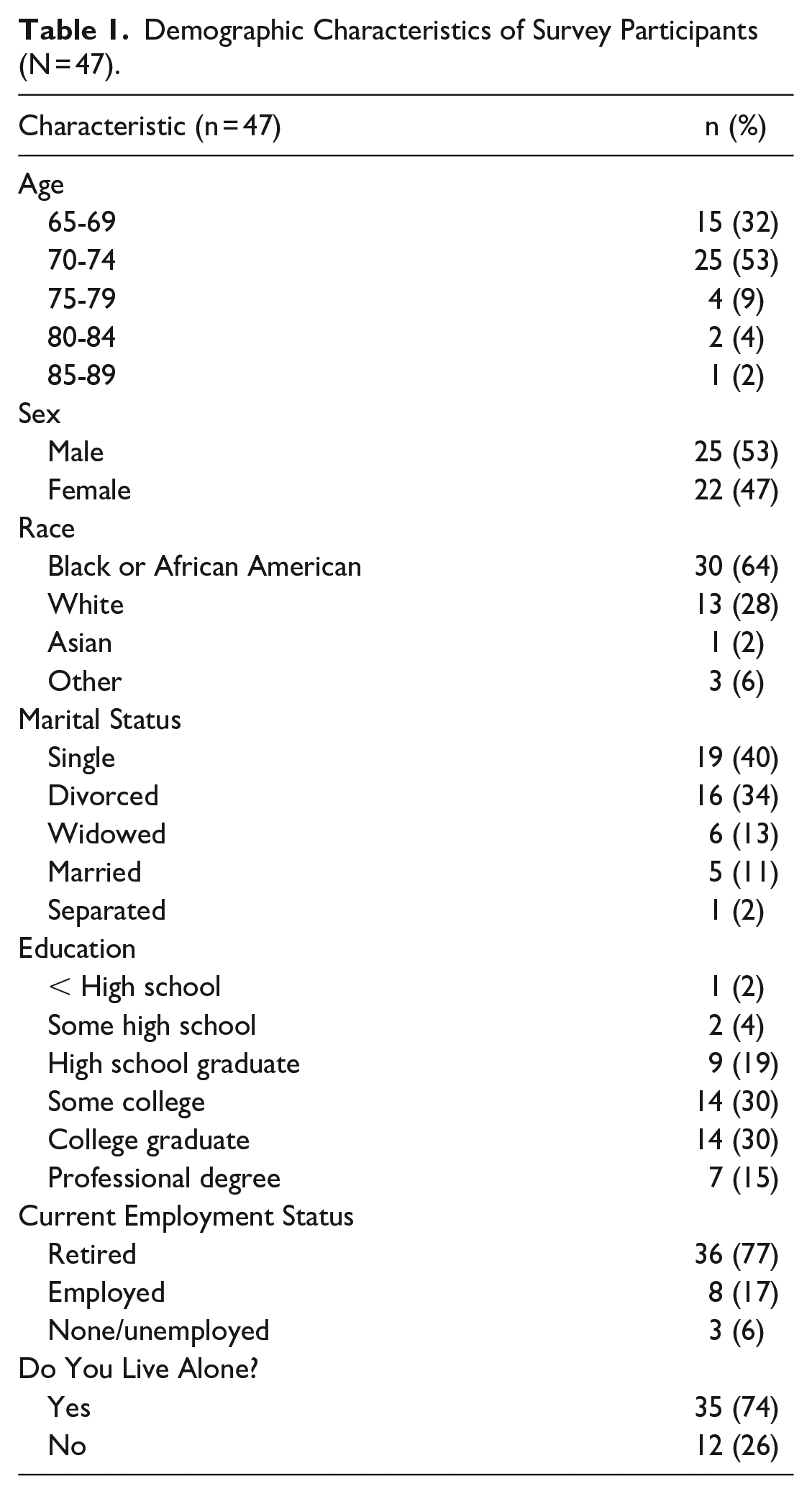
Out of the 50 participants that we aimed to include in the study, 47 of them fulfilled the requirements, and had their data analyzed. Three potential participants were excluded from the study: 1 for being under age 65, 1 for being a duplicative participant, and 1 for being lost to follow-up. The demographic characteristics of the participants are presented in Table 1. The average age of the participants was 71 years. The majority of the participants were male (53%), and most self-reported as Black (64%). Some college-level education or higher was reported by 75% of the participants. The participants’ relationship status was mostly single (40%) or divorced (34%). A majority of the participants were retired (77%), and most lived alone (74%).
Demographic Characteristics of Survey Participants (N = 47).
Attitudes, Beliefs, and Perceptions
Table 2 provided information about the participants’ perceived importance of cannabis as a therapy, their knowledge of the uses and health risks of cannabis, and their comfort level discussing cannabis with their primary care provider (PCP). Seventy-six percent of participants considered cannabis a highly important treatment for older adults, and 42% considered themselves highly knowledgeable (“very knowledgeable” or “moderately knowledgeable”) about the uses of cannabis. Additionally, 79% of participants reported feeling very comfortable discussing cannabis with their PCP.
Participants’ Attitudes on Several Topics Regarding Cannabis (n = 47; [n (%)]).

Importance Scale: 1-Extremely important; 2-Moderately important; 3-Somewhat important; 4-Not very important; 5-Not at all important.
Knowledge Scale: 1-Very knowledgeable; 2-Moderately knowledgeable; 3-Somewhat knowledgeable; 4-Not very knowledgeable; 5-Not at all knowledgeable.
Comfort Scale: 1-Extremely comfortable; 2-Moderately comfortable; 3-Somewhat comfortable; 4-Not very comfortable; 5-Not at all comfortable.
The participants were presented with statements related to their beliefs regarding the uses and health risks of cannabis (See Supplemental Table 1). More than two-thirds of participants believed that cannabis could be effective in treating cancer pain, arthritis pain, glaucoma, and anxiety. Additionally, 51% of participants stated that cannabis was not an addictive drug. Almost 40% believed that cannabis could improve bipolar disease symptoms. However, the questions related to the potential of cannabis to interact with prescription medications used for blood pressure and diabetes, and medications used for depression and bipolar disorder, had the most “neutral/don’t know” responses (60% and 67%, respectively).
Eighty-three percent of participants considered cannabis to be less harmful to a person’s health compared to alcohol, while more than half (52%) of participants considered vaping cannabis as an unsafe method of delivery. Additionally, 87% believed legalizing cannabis would make its use more acceptable to older adults, and 98% thought physicians should offer cannabis to treat medical conditions commonly seen in older adults. (See Supplemental Table 2)
All 47 participants believed there were benefits to legalizing cannabis, and when asked to further elaborate, the responses generally fell into 3 categories: medical benefits, societal benefits, and economic benefits. Over two-thirds (72%) of participants cited medical benefits, with the most common being to treat mood disorders such as anxiety, sleep issues, and depression, followed by benefits for glaucoma, arthritis, and pain relief. Societal benefits mentioned ranged from reducing crime and unnecessary arrests to destigmatizing cannabis use, and almost half (45%) expressed these views. About one-fifth (21%) of participants mentioned economic benefits to legalization, specifically increased tax revenue.
Participants were asked about their perceived importance of understanding various health topics related to cannabis, including purity, side effects, potential adverse events, drug interactions, long-term effects, safest delivery methods, and abuse potential (See Supplemental Table 3). At least 80% of participants considered each topic to be of high importance, with almost two-thirds considering them “extremely important.” Understanding potential drug interactions (92%), purity (90%), and side effects (87%) were the topics with the highest response of high importance.
Provider Inquiry on Substance Use (n = 47; [n (%)]).

Participant-Provider Relationship
Table 3 presents the responses of participants when asked if their PCP had asked about their substance use in the past year. The participants were asked about 3 different substances: tobacco, alcohol, and cannabis. Over half of the participants reported being asked about tobacco (55%) or alcohol (57%) use within the past year by their PCP. However, only 23% of participants reported being asked about cannabis use.
Sources
Table 4 summarizes the sources of health-related and cannabis-related information reported by the participants. The majority of participants obtained health-related information from television news (N = 22) and the internet (N = 21). In terms of cannabis-related information, the internet was the most common source (N = 20), followed by friends or family (N = 13). It is important to note that this question did not distinguish between internet searches and social media postings.
Sources for Health-related and Cannabis-related Information (n = 47; [n (%)]).

Discussion
The present study aimed to investigate the attitudes, beliefs, and perceptions of older adults toward cannabis as a medicinal product. The results suggest that there is a consensus among the participants that cannabis is a legitimate treatment for many physical and mental health diseases and could provide protection against several diseases and disorders commonly seen with aging. However, some participants lacked knowledge regarding its risks, drug interactions, or how cannabis could negatively impact their health. This highlights the importance of healthcare providers’ role in providing accurate and reliable information to improve the use of cannabis as a therapy for various health conditions that are prevalent in older adults, ultimately improving their overall quality of life.
Our study also explored the level of comfort of older adult patients in discussing medical cannabis with their PCPs. Similar to the Weiss et al study, 17 we found that a majority of our sample (nearly 80%) were comfortable speaking to their PCP about cannabis. However, our study also revealed that their PCPs inquired less often about cannabis use as part of their screening for other substances, such as tobacco and alcohol, despite the participants’ willingness to discuss it. This highlights the need for PCPs to initiate discussions with their patients about cannabis use and provide evidence-based information on its potential benefits and risks.
Although the participants in our study reported being knowledgeable about cannabis use, the results also revealed a phenomenon known as “overclaiming,” where individuals who believe they know more about a topic are more likely to claim knowledge of that topic which does not exist. 19 This is particularly concerning in the cannabis world, where failure to recognize or admit the knowledge gap could lead to poor decision-making with devastating consequences. This highlights the need for healthcare providers to address misconceptions and provide accurate information to improve the safe use of cannabis as a therapy.
A 2022 survey that noted only 11% of Canadians found public health information about cannabis in a healthcare setting, while 17% and 28% found information on social media or TV/Radio, respectively. 20 Our study is consistent with the data which demonstrates that older adults frequently sought information about cannabis from online resources, 10 which may not provide the most reliable information on the effects of cannabis use. Therefore, it underscores the importance of healthcare providers in educating their patients and providing evidence-based information on the potential benefits and risks of cannabis use.
When asked about their PCPs offering cannabis as a treatment for conditions seen in older adults, almost all participants agreed that cannabis should be included as a potential intervention. However, the lack of research regarding the effects of cannabis on older adults with specific diagnoses or disorders, the impact on cognition and mental health issues, drug interactions, and physical functioning, including the risk of falls, negatively impacts physicians’ ability to discuss the effects of cannabis with their older adult patients.21,22 Prior research has shown clinicians are generally supportive of medical cannabis; however, they have concerns about the scant evidence on effectiveness, product quality, and potential safety issues.13-16 The perceived benefits and minimal risks of cannabis use in this population signal an urgent need for research and dissemination of evidence-based information.
This study’s primary limitation is its sample size, which, although taken from most zip codes across Philadelphia, was small in each area. Furthermore, the study only obtained participants from Philadelphia, reducing the generalizability of the data beyond this region. However, the purpose of this pilot study was to identify areas requiring further research and assess the willingness of this population to discuss cannabis, particularly given its illegality on a federal level and the potential for cultural stigmatization. Our findings indicate that older adults are eager to discuss cannabis despite its federal illegality, likely due to a self-selection bias among supporters of cannabis use who responded to the survey. This bias may also explain the high number of college-educated participants in the sample, who exhibited an increased willingness to complete the survey and provide honest responses.
Conclusions
This study highlights the growing interest of older adults in the use of cannabis for medical purposes. Although participants expressed positive attitudes toward cannabis, they had limited knowledge of potential adverse effects and drug interactions. This lack of knowledge led many older adults to rely on less reliable sources of information such as the internet. PCPs may be better positioned to provide older adults with reliable information on the use of medical cannabis. However, it is unclear whether PCPs have the necessary knowledge and support to meet the increasing demand for cannabis-related information from their patients. Therefore, further research is needed to identify the availability of reliable information and support for PCPs as the demand for medical cannabis use among older adults continues to rise.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319231177284 – Supplemental material for Attitudes, Beliefs, and Perceptions on Cannabis Among Older Adults Aged 65 and Older: A cross-sectional Survey
Supplemental material, sj-docx-1-jpc-10.1177_21501319231177284 for Attitudes, Beliefs, and Perceptions on Cannabis Among Older Adults Aged 65 and Older: A cross-sectional Survey by Alex M. Kleidon, Andrew M. Peterson, Ilene Warner-Maron and Allen Glicksman in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The authors would like to acknowledge Nashia Brooks for her role in recruiting and scheduling the participants.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AK received summer salary support. IWM, AP, and AG did not receive compensation for their participation. AP is on a Medical Advisory board for a New Jersey Cannabis dispensary, Holistic LLC I. IWM is a principal in the consulting firm, Alden Geriatrics, the sponsor of this research.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Alden Geriatrics, a consulting firm located in Newtown Square, PA.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.