
Abstract
Introduction/Objectives:
Adults with food insecurity (FI) face barriers to hypertension management, including difficulty adhering to diet recommendations. Few community health worker (CHW) interventions focus on diet to improve blood pressure. This qualitative study elicited patient and CHW perspectives on healthy eating and a future CHW nutrition intervention for patients with hypertension.
Methods:
Twenty-five patients with hypertension and FI and 5 CHWs participating in a hypertension health coaching program from 5 Boston-area health centers participated in semi-structured interviews from July to September 2023. Interviews were audio recorded, transcribed, and analyzed using the Framework Method.
Results:
Themes included: 1) Variable patient knowledge about dietary patterns for hypertension management and low confidence in interpreting nutrition labels; 2) Culture influenced healthy food perception; and 3) Barriers to healthy eating included cost, limited cooking abilities/supplies, and competing demands. Patients and CHWs favored simple nutrition education materials (e.g., traffic light nutrition ranking, healthy meals on a budget). Patients had mixed opinions about CHW-accompanied supermarket visits.
Conclusions:
This study identified culture, knowledge gaps, and budget constraints as factors influencing diet among patients with hypertension and FI. A CHW-delivered intervention could include simplified nutrition education, strategies for healthy eating on a budget, and linkage to community-based food programs.
Introduction
Food insecurity, defined as limited or uncertain access to food, is associated with increased risk of diet-sensitive chronic conditions and disproportionately affects people with hypertension compared to normotensive individuals.1,2 Dietary modification is part of first-line, nonpharmacologic therapy for hypertension management, but following a healthy diet can be difficult, especially for people experiencing food insecurity, due to higher cost of healthier foods.3 -5
Nutrition security, a related but distinct concept, emphasizes not only availability and access to food, but also the intake and stability of nutritious food over time. 6 Although the US Preventive Services Task Force recommends that all adults with cardiovascular risk factors including hypertension be offered or referred to behavioral counseling to promote a healthy diet, 7 nutrition counseling rarely occurs during primary care visits for hypertension, largely due to time constraints, competing demands,8 -13 and inadequate nutrition education training for physicians. 14 Furthermore, research has shown that primary care clinicians seldom or never refer patients with hypertension to registered dietitians, 15 and referral rates may be even lower for low-income populations given that Medicaid coverage of nutrition services varies by state.16,17 Integrating community health workers (CHWs) trained in nutrition into care teams is a promising strategy for hypertension management, as team-based care models that include CHWs have been shown to improve blood pressure in underserved populations and are promoted by the American Heart Association.18,19
While existing studies of CHW interventions for hypertension management in the US have demonstrated improvement in self-monitoring behaviors, medication adherence, and appointment keeping,20 -25 few have integrated diet interventions to improve blood pressure and cardiovascular risk. The objective of this qualitative study was to explore patient and CHW perspectives on healthy eating among low-income community health center patients with hypertension, and to elicit participants’ opinions on a potential CHW-delivered nutrition intervention to improve diet for adults experiencing nutrition insecurity.
Methods
Study Design, Setting, and Participants
This study used a qualitative descriptive design, which was chosen for its ability to help researchers produce a rich but straightforward description of complex factors that contribute to a phenomenon 26 and gather information needed to develop or refine an intervention. 27 Semi-structured interviews were conducted with community health center patients and CHWs between July and September 2023 to explore sociodemographic and behavioral factors that impact dietary choices, and to obtain participants’ opinions on a potential nutrition-focused CHW intervention. Patients were recruited over the telephone from LiveWell, a cohort study (N = 1056) designed to evaluate a Massachusetts Medicaid program that provides accountable care organizations (ACOs) with funding to address participants’ food and housing insecurity. 28 LiveWell enrolled English and Spanish-speaking adults 21 to 62 years old who had Medicaid or commercial ACO insurance and at least 2 visits in the prior 2 years at 1 of 5 health centers within Mass General Brigham (MGB), a large integrated health system in eastern Massachusetts. LiveWell participants were followed over 3 years with annual surveys which collected data on various demographic, behavioral, and psychological measures, as well as health-related social needs such as food security status as measured by the USDA 10-item Adult Food Security Survey Module. 29 For this study, we purposively sampled LiveWell patients with hypertension who had marginal, low, or very low food security at least once during the 3 years prior to this study (N = 234) to gather perspectives on healthy eating and feedback on a potential nutrition intervention from patients at high risk of having low diet quality. Twenty-five patients approximating the racial/ethnic composition of LiveWell were included, a sample size generally sufficient to achieve data saturation.30,31 Five CHWs who served racially and ethnically diverse patients in an MGB hypertension health coaching program were recruited via email per the recommendation of their manager. Study procedures were approved by the MGB institutional review board on November 8, 2022. All participants provided verbal informed consent for participation. Patients were remunerated $50 and CHWs were provided a meal for participation.
Data Collection
Trained clinical research coordinators (KCF, AM, OB) conducted one-on-one telephone interviews with patient participants (average duration: 38 min); coordinators may have had prior telephone or email contact with patients when collecting LiveWell data. An endocrinology fellow physician (KDG) conducted hour-long, one-on-one interviews over virtual video meeting platform with 5 CHWs with whom she had no prior relationship. Interviews were conducted in English or Spanish (AM and OB). Patient semi-structured interview guides (Appendix) were developed with input from all study team members to target 4 main content areas: general nutrition knowledge and dietary habits, barriers and facilitators to healthy eating, opinions on 5 possible components of a CHW intervention, and anticipated barriers and facilitators to intervention participation. The proposed intervention components included simplified nutrition education about reading nutrition labels and using a traffic light labeling system to identify the healthfulness of foods32,33; shopping for groceries on a budget; 34 preparing culturally-relevant healthy meals; supermarket visits accompanied by CHWs to reinforce healthy choices and food budgeting; and linkage to community-based food programs. CHW interview guides (Appendix) explored the same content areas and additional questions about their perceptions of patients’ nutrition knowledge and opinions about home visits.
Patient demographics were previously collected as part of the LiveWell study. Data on household size, dependents, employment status, use of food assistance programs (eg, Supplemental Nutrition Assistance Program, food pantries), duration of hypertension diagnosis, and hypertension medication use were collected during interviews. CHW demographic data collected during interviews included years of CHW experience, age, gender, race, and ethnicity.
Data Analysis
Descriptive statistics were used to analyze demographic data. Coding and analysis of qualitative data was conducted by KDG, KCF, AM, and OB following the Framework Method, a seven-step systematic procedure commonly used for thematic analysis of semi-structured interview transcripts. This method was chosen for its ability to reduce and organize data into a structured framework matrix based on defined categories and codes, which allows all team members, even those not directly involved with the technical aspects of coding, to engage with the data and offer input in the analysis. 35 Interviews were audio recorded and transcribed using online digital transcription service. Three transcripts were initially chosen for independent review by 2 to 3 coders per transcript. Coders established a list of codes based on interview guide content areas, complemented by inductive addition of codes to capture novel concepts from the initial transcripts. Coders then compared and discussed codes and definitions. Once consensus was reached, a working analytical framework of codes was entered into Dedoose software (version 9.2.006, SocioCultural Research Consultants, LLC) to facilitate coding. Using this software, 2 coders (KDG and KCF for English or AM and OB for Spanish transcripts) independently indexed excerpts from each remaining transcript into this coding framework. Throughout the process, the coders discussed progress and questions to ensure consistent code application and added novel codes to the framework as they arose; any discrepancies were resolved with input from principal investigator ANT. Upon completion of coding, the coding team generated a framework matrix organized by interviewee, code, and excerpt to facilitate analysis of the data for common characteristics and themes.
Results
Participant Characteristics
Twenty-five patients and 5 CHWs completed interviews. Median age (IQR) of patients was 49 (33, 63) years. More than half of patients were female (60%) and Hispanic (56%); 32% spoke Spanish as their primary language. Participants self-identified race including 32% percent Black or African-American, 4% “mixed” race, 24% “other” race, and 40% White. The majority (88%) resided in a household of 2 or more people. Most (68%) did not have children in the household, and about half reported being unemployed. About 3 quarters of participants reported using at least 1 food assistance program such as Supplemental Nutrition Assistance Program or food pantries. All patients reported taking at least 1 daily hypertension medication. CHW ages ranged from 26 to 63 years old and most were female (N = 4). CHWs identified as Black, White, and Latinx. All had at least 2 years of CHW experience.
Patient and CHW Perceptions of Nutrition, Health, and Barriers to Healthy Eating
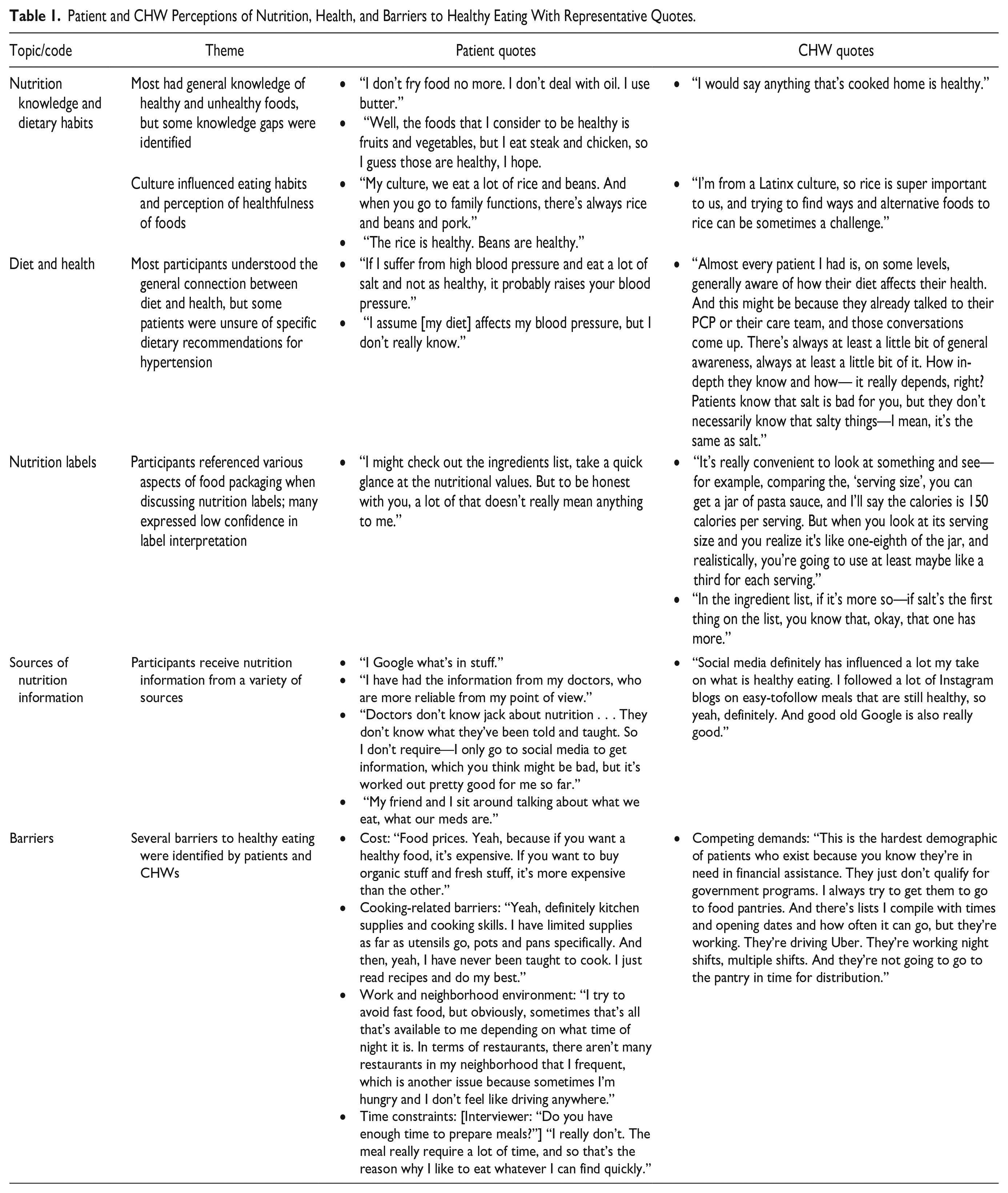
Table 1 presents themes surrounding patient and CHW perceptions of nutrition and eating habits with representative quotes. Patients and CHWs had general knowledge of healthy and unhealthy foods, but there were some inaccuracies (eg, cooking with butter is healthier than oil). Culture influenced eating habits and the perception of which foods were considered healthy; for example, Hispanic and Latinx patients and CHWs emphasized rice as a dietary staple but had mixed opinions on its healthfulness. While many patients and all CHWs understood the connection between diet and health, some patients were unsure of specific dietary recommendations for hypertension. When asked about nutrition labels, patients and CHWs referenced various items found on food packaging, including different aspects of the nutritional facts label (eg, serving size, calories), ingredient lists, expiration dates, brand labels, and price of food. Many patients expressed low confidence in interpreting these labels. Patients and CHWs reported receiving nutrition information from a variety of sources, including the internet, social media, television, family or friends, and healthcare professionals. However, patients had mixed attitudes about the reliability of nutrition information from healthcare professionals. While cost was identified as the primary barrier to healthy eating, other important barriers included concerns related to food preparation (ie, limited cooking abilities, lack of supplies or appliances, food spoilage), work and neighborhood food environments, time constraints and competing demands, and stigma related to use of food assistance programs.
Patient and CHW Perceptions of Nutrition, Health, and Barriers to Healthy Eating With Representative Quotes.
Opinions on CHW-Delivered Intervention Components
Table 2 displays participants’ attitudes towards potential intervention components and barriers to participation in a CHW-delivered nutrition intervention for hypertension management. Simplified education about nutrition label reading and the traffic light labeling system received positive feedback from most patients and CHWs; many patients expressed interest in learning about the best dietary choices for their health conditions. Patients and CHWs generally favored resources to guide them in shopping for healthy groceries on a budget, and patients expressed particular interest in learning how to create shopping lists, use coupons, compare prices, and purchase a variety of foods. Patients and CHWs also favored resources to prepare culturally-relevant meals. While patients were especially interested in healthy recipe ideas, food substitutions, and food preparation methods, 1 CHW expressed concern about certain cultures being less inclined to measuring ingredients, making them less likely to view recipe resources favorably.
Patient and CHW Opinions on CHW Nutrition Intervention Components and Barriers to Program Participation.

The idea of supermarket visits with CHWs was met with mixed attitudes. Many patients were interested in assistance with reading nutrition labels and choosing healthy, affordable options when shopping, but some patients described concerns about potential stigma associated with shopping with a CHW. Several patients and CHWs expressed worry about logistical challenges (eg, lack of transportation, scheduling conflicts). Similarly, patients provided mixed feedback on assistance connecting with community-based food programs, such as food pantries. While some patients expressed concern about quality of food provided at pantries, many patients expressed interest in a consolidated guide to food resources in their neighborhood that could accommodate their primary language, food preferences, and physical limitations. Some CHWs viewed home visits as an opportunity to provide tailored nutrition support while others expressed concerns about travel time and scheduling. Both patients and CHWs suggested that lack of time, motivation, or transportation, and stigma related to participation, could be possible barriers to enrolling in this type of intervention.
Discussion
This qualitative study of low-income community health center patients with hypertension and CHWs with hypertension coaching experience identified not only high cost of healthy food as a primary barrier to healthy eating but also several other factors that influenced dietary choices (eg, neighborhood and work environment, time constraints, competing demands, stigma surrounding the use of community food resources). Overall, patients and CHWs favored the development of a CHW nutrition intervention and were particularly interested in simplified education on healthy food choices using strategies such as traffic light labeling system to identify healthier food options32,33 and reading nutrition labels, as well as approaches to shop for healthy food on a budget. 34
In addition to health professionals, family and friends were important source of nutrition information for patients. Since CHWs typically reside in the communities they serve, 36 they can leverage their position as trusted community members to deliver evidence-based nutrition counseling. CHWs can relate to patients through shared ethnicity, language, socioeconomic status, and life experiences,37,38 empowering them with a nuanced understanding of their patients’ health needs and the ability to provide culturally appropriate health counseling. In their role, CHWs are typically trained in the navigation of community-based food resources, which was highlighted in the interviews as an important component of nutrition counseling.
CHWs could help improve diet for patients with hypertension as part of a collaborative care model in which primary care clinicians partner with a team of clinical staff to improve chronic disease management.22,39 -41 CHWs can serve as a natural extension to this model for populations experiencing health-related social needs; evidence suggests that patients with food insecurity have a high likelihood of being referred to CHWs by care managers. 42 As screening for health-related social needs becomes more common and as more states authorize Medicaid reimbursement for CHW services,43,44 primary care referrals to CHWs are likely to increase. 45
This study explored with patients and CHWs how a future CHW intervention to improve diet in patients with hypertension and nutrition insecurity could be designed. Another study similarly incorporated participant feedback to develop and implement a single-arm pilot of a nutrition-focused CHW intervention to improve food security for formerly homeless adults living in a permanent supportive housing community. The study developed CHW intervention components based on needs assessments of 83 community residents and qualitative resident feedback. Results of this study found that most participants reported improved food security scores at 90 days follow-up. 46
Given that cost was identified as the primary barrier to healthy eating in this study, a CHW intervention that provides strategies for shopping on a budget could directly address this barrier. Study participants also reported that factors such as culture and food preparation techniques and preferences impact dietary choices. CHWs could provide patients with simple and culturally-appropriate strategies to prepare healthy meals, such as basic cooking methods and meal planning guides. 47 Because CHWs often provide care in community-based settings such as homes, schools, local businesses, or community centers, 48 home and supermarket visits with CHWs may be effective components of a CHW intervention for people with hypertension and nutrition insecurity. Linkage to community-based food resources such as nutrition assistance programs or food pantries, a strategy employed by other CHW-delivered hypertension interventions, 49 may also be effective but must be designed to minimize perceived stigma.
There are several limitations of this qualitative study. While the primary objective was to inform the design of a CHW-delivered nutrition intervention to improve diet and blood pressure control in patients with hypertension and nutrition insecurity, the sample was drawn from a larger cohort study of low-income community health center patients who may not have been experiencing nutrition insecurity during the study period. In addition, the sample consisted primarily of younger and middle-aged adults with Medicaid or commercial ACO insurance and took place within an urban health system with an existing CHW program in the Northeastern US, which limits generalizability.
Conclusions
In summary, this study identified many barriers to healthy eating among low-income adults with hypertension. Nutrition counseling delivered by CHWs, including simplified nutrition education, strategies for healthy eating on a limited budget, and linkage to community-based food resources, could improve diet and hypertension control in adults with nutrition insecurity. A CHW intervention could extend the reach of nutrition counseling for hypertension management, which does not occur routinely in primary care visits, and could improve health equity in populations experiencing health-related social needs.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241285855 – Supplemental material for Patient and Community Health Worker (CHW) Perspectives on a CHW-delivered Nutrition Intervention for Low-Income Adults with Hypertension: A Qualitative Study
Supplemental material, sj-docx-1-jpc-10.1177_21501319241285855 for Patient and Community Health Worker (CHW) Perspectives on a CHW-delivered Nutrition Intervention for Low-Income Adults with Hypertension: A Qualitative Study by Kristine D. Gu, Jessica Cheng, Ashlie Malone, Katherine C. Faulkner, Oldy Bejarano, Emily Gelsomin and Anne N. Thorndike in Journal of Primary Care & Community Health
Footnotes
Author Contributions
ANT was responsible for the study design and funding. All authors contributed to the development of qualitative interview guides. KDG was responsible for drafting the manuscript text. All authors contributed to manuscript revision and have approved the final version, and all those who are qualified to be authors are listed.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health [K24HL163073 (ANT), T32DK007028 (KDG), T32HL098048 (JC), and R01DK124145 (ANT)].
Ethical Considerations
The study received ethical approval from the Mass General Brigham institutional review board on November 8, 2022.
Consent to Participate
All participants provided verbal informed consent for participation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.