
Abstract
Objectives:
Healthcare screening identifies factors that impact patient health and well-being. Hunger as a Vital Sign (HVS) is widely applied as a screening tool to assess food security. However, there are no common practice screening questions to identify patients who are nutrition insecure or acquire free food from community-based organizations. This study used self-reported survey data from a non-Medicaid insured adult population approximately one year after the start of the COVID-19 pandemic (2021). The survey examined the extent to which the HVS measure might have under-estimated population-level food insecurity and/or nutrition insecurity, as well as under-identified food and nutrition insecurity among patients being screened for social risks in the healthcare setting.
Methods:
Data from a 2021 English-only mailed/online survey were analyzed for 2791 Kaiser Permanente Northern California (KPNC) non-Medicaid insured members ages 35-85 years. Sociodemographics, financial strain, food insecurity, acquiring free food from community-based organizations, and nutrition insecurity were assessed. Data from respondents’ electronic health records were abstracted to identify adults with diet-related chronic health conditions. Data were weighted to the age × sex × racial/ethnic composition of the 2019 KPNC adult membership. Differences between groups were evaluated for statistical significance using adjusted prevalence ratios (aPRs) derived from modified log Poisson regression models.
Results:
Overall, 8.5% of participants reported moderate or high food insecurity, 7.7% had acquired free food from community-based organizations, and 13% had nutrition insecurity. Black and Latino adults were significantly more likely than White adults to have food insecurity (17.4% and 13.1% vs 5.6%, aPRs = 2.97 and 2.19), acquired free food from community-based organizations (15.1% and 15.3% vs 4.1%, aPRs = 3.74 and 3.93), nutrition insecurity (22.1% and 23.9% vs 7.9%, aPRs = 2.65 and 2.64), and food and nutrition insecurity (32.4% and 32.5% vs 12.3%, aPRs = 2.54 and 2.44). Almost 20% of adults who had been diagnosed with diabetes, prediabetes, ischemic CAD, or heart failure were food insecure and 14% were nutrition insecure.
Conclusions:
Expanding food-related healthcare screening to identify and assess food insecurity, nutrition insecurity, and use of community-based emergency food resources together is essential for supporting referrals that will help patients achieve optimal health.
Keywords
Background
Food insecurity is defined by the United States (U.S.) Department of Agriculture as lack of access by all people at all times to enough food for an active, healthy life. 1 Food insecurity was experienced by an estimated 10.2% of U.S. households in 2021. 2 Food insecurity is driven by poverty, resulting in limited resources to purchase food.3,4 It leads to inadequate dietary patterns that increase risk of developing or exacerbating diet-related chronic health conditions.5,6 Nutrition insecurity is a broader term describing inconsistent access to enough affordable healthy foods that promote well-being and prevent or manage diet-related chronic health conditions. 7
Increasingly, healthcare settings implement social risk and social needs screening to identify and address factors that impact patient health and well-being, such as food security, housing stability, and social isolation. 8 Validated measures exist to estimate prevalence of food insecurity, including the 2-item Hunger Vital Sign (HVS) that is widely used in healthcare settings for universal patient screening for food insecurity as a social risk. 9 However, there are currently no universally recommended questions to use with the HVS screener to identify patients who are nutrition insecure.
Additionally, when a patient screens positive for food insecurity or nutrition insecurity, protocols should be in place for clinical professionals to refer patients to resources. 10 One key source of referral support in communities is emergency food supplies provided by community organizations, such as food banks, food pantries, and churches. Healthcare settings can include screening questions about emergency food supply use to understand if such a resource is already being used or may help address unmet food or nutrition needs. Currently, the HVS items do not identify patients who acquire emergency food supplies and there are no universally recommended screening questions.
Consequently, there is limited information about the extent to which food insecurity and nutrition insecurity overlap, the proportion of the population that is nutrition insecure but does not meet the criteria for being considered food insecure, the extent of emergency food supply use among food insecure and nutrition insecure populations, and the magnitude of food insecurity and/or nutrition insecurity among a sample of adults in an integrated healthcare system.
Given the importance of consuming a healthy diet for prevention and management of diet-related cardiovascular conditions (e.g., diabetes, ischemic coronary artery disease) and widespread implementation of screening for food insecurity in healthcare settings, it is essential to learn the extent to which the current HVS screener may be under-identifying patients who are food insecure and/or nutrition insecure. Furthermore, recommendations about ways to address food and/or nutrition insecurity that healthcare providers can provide to patients are needed.
In this study, we analyzed self-reported data from an existing survey of a non-Medicaid insured adult health plan population fielded in 2021, approximately 1 year after the start of the COVID-19 pandemic. Notably, food insecurity nationwide peaked at 20.4% during the early stages of the COVID-19 pandemic (2020), dropped to 10.2% in 2021, and rose to 12.8% in 2022.2,11,12
Our research examines the extent to which the HVS measure might under-estimate population-level food and/or nutrition insecurity and might under-identify patients who are being screened for food and nutrition insecurity in the healthcare setting. Our goal is to inform approaches for patient screening and referral, as well as population-level estimates of food and nutrition insecurity in healthcare settings and public health surveillance.
Methods
Study Design
This cross-sectional study involved secondary analysis of data from a 2021 self-administered survey. Survey data were also linked with diet-related chronic health condition diagnoses from respondent electronic health records (EHR) to examine the impact of using different measures to screen for food and/or nutrition insecurity.
Setting and Study Population
KPNC is an integrated healthcare delivery system that provides health care to a sociodemographically diverse health plan membership with over 3 million adults who mostly reside in the Greater San Francisco Bay Area, Silicon Valley, Sacramento area, and Central Valley. The sociodemographic and health characteristics of the KPNC adult membership have been shown to be very similar to those of the non-Medicaid insured adult population of Northern California. 13
This study focused on middle-aged and older KPNC health plan members who were not covered by Medicaid (government-funded healthcare coverage for financially eligible low-income adults, children, pregnant women, elderly adults, and people with disabilities) and had a stable address at the time of the survey. Medicaid-covered members were excluded from the sample because the aim of the survey was to estimate prevalence of different social risks and social needs among the majority of adult health plan members who had not already been identified as meeting financial eligibility for Medicaid. Additionally, Medicaid-covered members were already routinely being screened for social needs and referred to resources they were eligible for to address those needs as part of the health plan’s Medicaid member onboarding process.
Data Sources
We analyzed self-reported data from a self-administered social risk survey of KPNC health plan members conducted in 2021, approximately 1 year after the start of the COVID-19 pandemic. 14 The survey, which could be completed using a mailed print questionnaire or online version, had been designed to learn about social risks, social needs, and attitudes toward social risk screening among middle-aged and older adults who were not covered by Medicaid. The survey was fielded with a stratified random sample of middle-aged (35-65 years) and older (66-85 years) included adults who had been non-Medicaid-covered KPNC members for at least 2 years and had English listed as their preferred spoken and written language in the EHR since for cost and other reasons, the survey materials were only available in English. The survey had an overall response rate of 29.0% (final sample N = 2870). For this study of food and nutrition insecurity, the sample was restricted to 2791 adults ages 35-85 years who were not missing data for any of the five food and nutrition insecurity variables being studied.
Because we were interested in how the food insecurity and nutrition insecurity measures would affect identification of in vulnerable subgroups, we used diagnosis data from respondents’ EHRs to identify subsets of adults with a diet-related cardiovascular condition (diabetes, prediabetes, ischemic coronary artery disease, and/or heart failure).
Study Variables
Table 1 summarizes the variables used in our analyses. Study variables included sociodemographic characteristics, financial strain, food and nutrition insecurity, and diet-related chronic health conditions. While the majority self-reported survey questions utilized previously developed survey items, modifications to the questions were made or interpretation was applied as described below to better address the study’s goals.
Study Variables Utilized to Assess Food and Nutrition Insecurity Among Non-Medicaid Insured Adults in an Integrated Healthcare Delivery System.

Derived from self-reported survey items.
Derived from electronic health record data.
Food insecurity questions were part of a grid that asked whether it was often, sometimes, or never true that the individual had experienced difficulties related to the question. The food insecurity risk (Food_Insec) measure was based on the 2 validated HVS screening questions and HVS risk algorithm, using a 3-month recall window. 9 Individuals were considered to have Food_Insec if they had worried about running out of food at least sometimes and/or had run out of food at least sometimes. Individuals who had run out of food at least sometimes or had often worried about running out of food due to lack of money were considered to have high Food_Insec. We also used a third question, derived from the Current Population Survey (modified from the USDA’s Household Food Security Survey Module), that ascertained whether an individual had in the prior 3 months acquired free food from community-based organizations, such as a food bank, food pantry, church, or other. 15 We named this measure Emerg_Food. Notably, eligibility criteria for obtaining free food from community organizations varies widely. From the Food_Insec measure and the Emerg_Food measure, we created a compound food insecurity variable (Food_Insec2) that reflected food insecurity risk based on having Food_Insec and/or use of Emerg_Food resources.
Nutrition insecurity risk (Nutr_Insec) was measured using responses to 2 survey questions. In both items, the survey used the term “healthy food” because this term is now being used in lay public health communications (e.g., Healthy People 2030) and surveys rather than “nutritious” food.6 -18 The first nutrition insecurity question used the HVS format and ascertained whether it was often, sometimes, or never true that it was hard for the individual to get enough healthy food during the prior 3 months. This question was meant to ascertain difficulty obtaining healthy food for any reason, not restricted to affordability. Because some individuals who would not meet the criteria for being food insecure but may struggle to afford foods that supported their health, a second question asked whether during the past 3 months, the individual ate less fruit, vegetables, and healthy foods because of the cost. This question was not modified from a validated survey item. People were considered to have Nutr_Insec if they sometimes or often had a hard time getting enough healthy food or if they had eaten less healthy food due to the cost. Finally, we created a compound Food/Nutr_Insec risk measure that indicated food and/or nutrition insecurity based on Food_Insec/Emerg_Food and/or Nutr_Insec.
Subsets of adults with diet-related chronic health conditions (diabetes, prediabetes, ischemic coronary artery disease, and/or congestive heart failure) were identified based on ICD-10 diagnosis codes. Diabetes was assigned based on an ICD-10 code for non-gestational diabetes during that same interval or entry into the Kaiser Permanente in Northern California Diabetes Registry (based on diagnosis codes, pharmacology, and laboratory values). 19
Financial strain was assigned based on Conger et al.’s having enough money to “make ends meet” at the end of the month question, modified with the 3-month recall period interval used for most of the other survey questions. 20 An individual was considered financially strained if they reported having just enough money at the end of the month to make ends meet, almost enough to make ends meet, or not enough to make ends meet.
Statistical Analysis
All analyses were formed using SAS v9.4 (SAS Institute, Cary, NC, 2014) and used respondent data weighted to the age (10-year intervals) × sex (male, female) × racial/ethnic (White, Black, Latino, Asian/PI, Other) composition of the 2019 KPNC adult membership with English spoken language preference. We produced descriptive statistics for sociodemographic and financial strain characteristics for the overall population, by sex (male and female), age group (35-65 vs 66-85 years), and race/ethnicity (White, Black, Latino, Asian/PI). We then estimated prevalence of Food_Insec, Emerg_Food, Food_Insec2, Nutr_Insec, and Food/Nutr_Insec by age group, by race/ethnicity, financial strain, and for subgroups with cardiovascular conditions.
Differences between the 2 age groups, the 4 racial/ethnic groups, and 4 levels of financial strain in prevalence of the food and/or nutrition insecurity measures were evaluated for statistical significance using adjusted prevalence ratios derived from modified log-Poisson regression models. Adjusted prevalence ratios (aPRs), which compare prevalence of a characteristic in 1 group to that in a reference group after adjusting for covariates, are a more appropriate measure than adjusted odds ratios to use when comparing characteristics that are not rare in the population.21,22 Age group comparisons (35-65 vs 66-85) controlled for sex and race/ethnicity; racial/ethnic comparisons (Black, Latino, Asian/PI vs White) controlled for age (10-year interval variable) and sex; and financial strain comparisons (not enough money, just enough money, enough money vs. more than enough money to make ends meet) controlled for age (10-year interval variable), sex, and race/ethnicity. Comparisons with aPRs that had 95% confidence intervals (CIs) not crossing 1.0 were statistically significant at P < .05. All estimates reported in the text are based on weighted data, all CIs are 95% CIs, and all subgroup differences mentioned in the text were significant at P < .05.
KPNC’s Institutional Review Board approved use of the survey data and linkage of survey data with EHR diagnosis data for this study with a waiver of written informed consent and HIPAA authorization. This study was supported by the KPNC Community Health Program.
Results
Cohort Characteristics
Based on weighted data, the study population (n = 2791) was 77.2% aged 35-65 and 27.8% aged 66-85 (mean age 66.3 years, std 11.6 years), 54.0% female, and 55.5% White, 7.9% Black, 13.7% Latino, 22.5% Asian/PI, and 0.4% Other race/ethnicity. Table 2 provides more details about the sociodemographic and health characteristics of the overall population and demographic subgroups. Overall, approximately three-fourths of adults usually had more than enough money to make ends meet (some left over or more than enough left over), but Black and Latino adults were less likely to be in this situation than White and Asian/PI adults (57.9% and 67.2% vs 78.7% and 71.3%, respectively). Black, Latino, and Asian/PI adults were more likely than White adults to have at least one of the diet-related chronic health conditions.
Sociodemographic and Health Characteristics of Study Cohort.

Abbreviations: Asian/PI, Asian or Native Hawaiian/Pacific Islander; CAD, Coronary artery disease; Wtd., Weighted.
Ns are actual numbers of respondents in the subgroup; Wtd. %s are estimates based on respondent data weighted to the age-sex-racial/ethnic composition of the adult health plan membership. Some multi-level variables have percentages that sum to >100% due to rounding.
Derived from ICD-10 diagnosis codes for the condition(s) found in respondent electronic health records in 2019, 2020, or 2021.
Prevalence of Food and Nutrition Insecurity
The overall prevalence of moderate/high Food_Insec based on the 3-month recall period was 8.5%, with 5.8% of adults considered to have high Food_Insec risk (had often worried about running out of food or ran out of food at least sometimes (Table 3). An additional 7.7% were at risk for food insecurity based on their use of Emerg_Food resources during that interval. Prevalence of Food_Insec2 risk (based on both measures) was 13.6%, a 60% increase over the Food_Insec risk estimate. Approximately 13% of adults had Nutr_Insec; by question, 10.7% (CI: 9.0%-12.5%) of adults sometimes or often had trouble getting enough healthy food, and 7.4% (CI: 5.8%-8.9%) had eaten less fruits, vegetables, and other healthy foods due to the cost. In total, nearly 20% of adults had Food/Nutr_Insec—more than double the estimate of food insecurity based on the Food_Insec measure alone.
Prevalence of Food Insecurity, Acquisition of Free Food, and Nutrition Insecurity, by Sociodemographic and Health Characteristics.
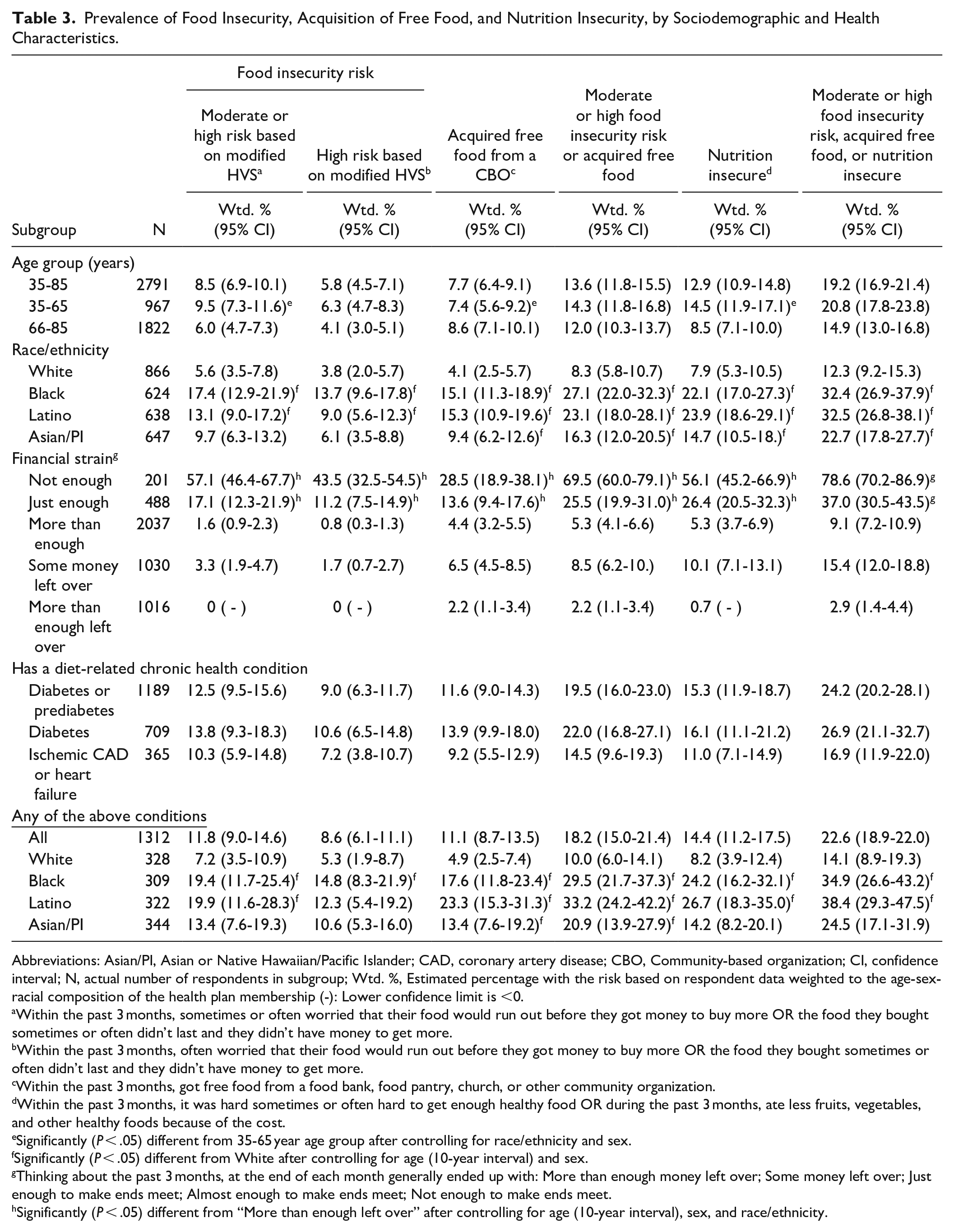
Abbreviations: Asian/PI, Asian or Native Hawaiian/Pacific Islander; CAD, coronary artery disease; CBO, Community-based organization; CI, confidence interval; N, actual number of respondents in subgroup; Wtd. %, Estimated percentage with the risk based on respondent data weighted to the age-sex-racial composition of the health plan membership (-): Lower confidence limit is <0.
Within the past 3 months, sometimes or often worried that their food would run out before they got money to buy more OR the food they bought sometimes or often didn’t last and they didn’t have money to get more.
Within the past 3 months, often worried that their food would run out before they got money to buy more OR the food they bought sometimes or often didn’t last and they didn’t have money to get more.
Within the past 3 months, got free food from a food bank, food pantry, church, or other community organization.
Within the past 3 months, it was hard sometimes or often hard to get enough healthy food OR during the past 3 months, ate less fruits, vegetables, and other healthy foods because of the cost.
Significantly (P < .05) different from 35-65 year age group after controlling for race/ethnicity and sex.
Significantly (P < .05) different from White after controlling for age (10-year interval) and sex.
Thinking about the past 3 months, at the end of each month generally ended up with: More than enough money left over; Some money left over; Just enough to make ends meet; Almost enough to make ends meet; Not enough to make ends meet.
Significantly (P < .05) different from “More than enough left over” after controlling for age (10-year interval), sex, and race/ethnicity.
Significant differences in Food_Insec and Nutr_Insec estimates were seen across age groups, racial/ethnic groups, and levels of financial strain. Table 3 shows unadjusted prevalence estimates and Table 4 shows aPRs. Compared to the older adult group, the middle-aged group had a higher prevalence of Food_Insec (9.5% vs 6.0%, aPR = 1.42) and Nutr_Insec (14.5% vs 8.5%, aPR = 1.43) risk. However, because the middle-aged group was less likely to have used Emerg_Food resources (7.4% vs 8.6%, aPR = 0.70), there was no significant age group difference in prevalence of Food_Insec2. Black and Latino adults were significantly more likely than White adults, to have Food_Insec risk (17.4% and 13.1% vs 5.6%, aPRs = 2.97 and 2.19, respectively), Emerg_Food use (15.1% and 15.3% vs 4.1%, aPRs = 3.74 and 3.93), to be food insecure based on Food_Insec2 (27.1% and 23.1% vs 8.3%, aPRs = 3.20 and 2.71, respectively), Nutr_Insec (22.1% and 23.9% vs 7.9%, aPRs = 2.65 and 2.64, respectively), and Food/Nutr_Insec (32.4% and 32.5% vs 12.3%, aPRs = 2.54 and 2.44, respectively). Asian/PI adults did not significantly differ from White adults in prevalence of Food_Insec risk but had a higher prevalence of Emerg_Food use (9.4%, aPR = 2.41), Food_Insec2 (16.3%, aPR = 1.91), Nutr_Insec (14.7%, aPR = 1.63), and Food/Nutr_Insec risk (22.7%, aPR = 1.71). These racial/ethnic differences were also seen in the subgroup of adults with diabetes or cardiovascular disease.
Adjusted Prevalence Ratios for Food and Nutrition Insecurity Risks, by Sociodemographic Characteristics.

Abbreviations: aPR, adjusted prevalence ratio; Asian/PI, Asian or Native Hawaiian/Pacific Islander; CBO, community-based organization; CI: confidence interval; N, actual number in subgroup.
Within the past 3 months, sometimes or often worried that their food would run out before they got money to buy more OR the food they bought sometimes or often didn’t last and they didn’t have money to get more.
Within the past 3 months, often worried that their food would run out before they got money to buy more OR the food they bought sometimes or often didn’t last and they didn’t have money to get more.
Within the past 3 months, got free food from a food bank, food pantry, church, or other community organization.
Within the past 3 months, it was sometimes or often hard to get enough healthy food OR during the past 3 months, ate less fruits, vegetables, and other healthy foods because of the cost.
Significantly (P < .05)different from 35-65 year age group after controlling for race/ethnicity and sex.
Significantly (P < .05)different from White after controlling for age (10-year interval)and sex.
Significantly (P < .05)different from “Money left over (some or more than enough money left)” after controlling for age (10-year interval), sex, and race/ethnicity.
Diabetes, prediabetes, ischemic coronary artery disease, and/or heart failure.
We also found large disparities in estimated Food_Insec and Nutr_Insec by level of financial strain (ability to “make ends meet”). Among adults who were not able to “make ends meet,” 57.1% had Food_Insec, 28.5% had used Emerg_Food, 69.5% were food insecure based on Food_Insec2, 56.1% had Nutr_Insec, and 78.6% Food/Nutr_Insec risk. Among adults who had just enough money to “make ends meet”, 17% had Food_Insec, 13.6% had used Emerg_Food, 25.5% were food insecure based on Food_Insec2, 26.4% had Nutr_Insec, and 37.0% had Food/Nutr_Insec. In contrast, among the subgroup of adults who had some or more than enough money left over at the end of the month, <2% had Food_Insec, 4.4% had used Emerg_Food, 5.3% had Food_Insec2, 5.3% had Nutr_Insec, and 9.1% had Food/Nutr_Insec. However, those who had “some money left over” were more likely to have Food_Insec and Nutr_Insec and to have used Emerg_Food than those who had “more than enough money left over.” Table 4 shows that the large disparities in food insecurity and nutrition insecurity between the 2 more financially strained subgroups and the group with sufficient funds remained after adjusting for race/ethnicity, age, and sex.
Overlap of Food and Nutrition Insecurity Screening Measures
Figure 1 illustrates the extent to which Food_Insec and Emerg_Food use overlapped among adults who had either of these characteristics. Among adults with Food_Insec, 30.5% had used Emerg_Food. However, only 33.5% of adults who had used Emerg_Food would have been identified as food insecure based on the Food_Insec question. Figure 2 shows that while 74.7% of adults with Food_Insec also had Nutr_Insec, only 49.4% of those who with Nutr_Insec would have been identified as being food insecure based on the Food_Insec question. Additionally, 42.5% of adults who had used Emerg_Food had Nutr_Insec (not shown).

Overlap of food insecurity and use of emergency free food from a community-based organization in the prior 3 months among adults with one or both risks.
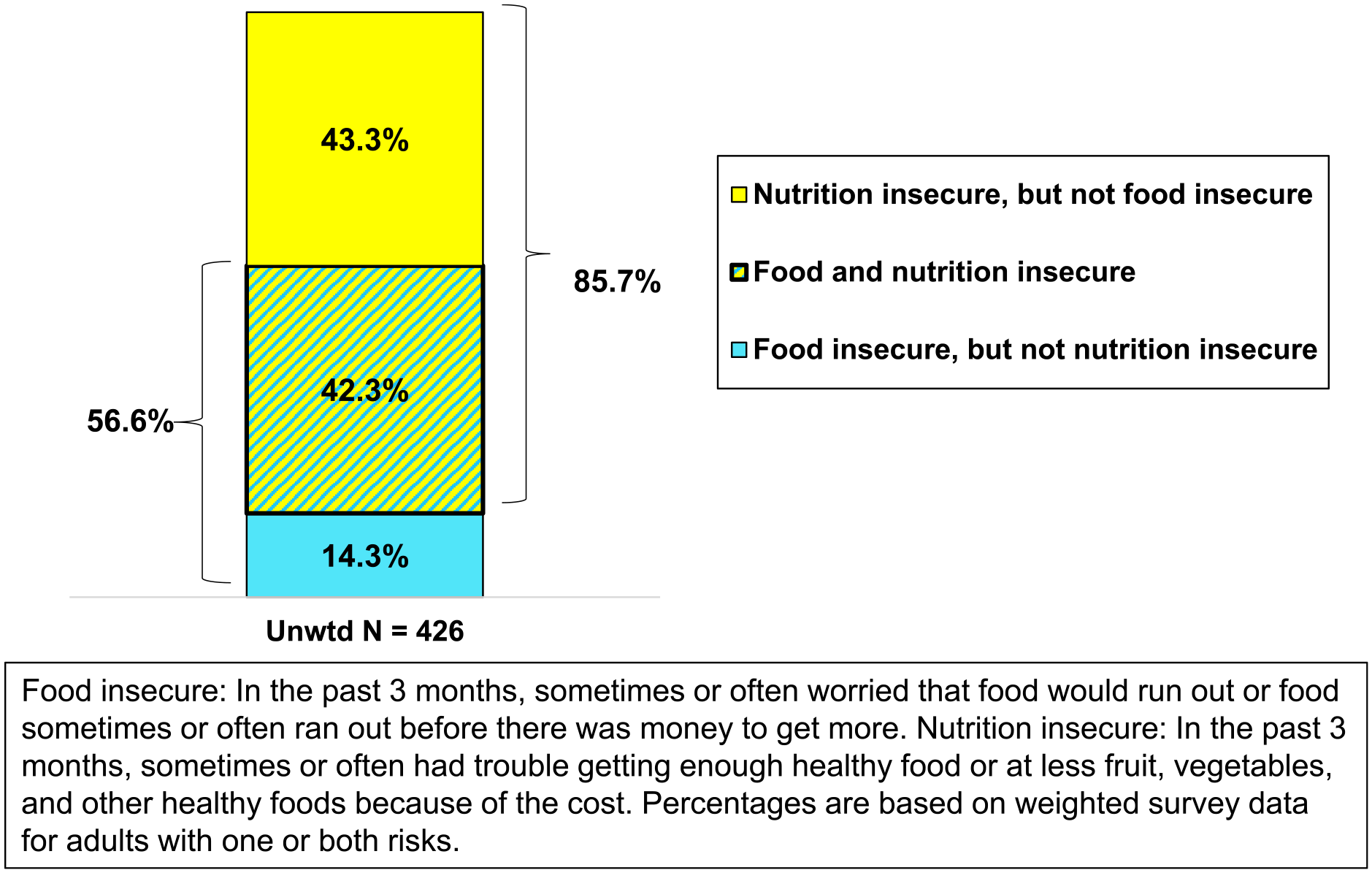
Overlap of food and nutrition insecurity among adults with one or both risks.
Discussion
This study found notable variations and overlap of measures used to identify food and nutrition insecurity derived from patient-reported data collected in a 2021 survey. These results can be used to inform recommendations about screening approaches and advising patients about actions they can take to improve their access to healthy foods.
Extent to Which the HVS Screener may be Under-Identifying Food and Nutrition Insecurity Among Patients Being Screened for Social Risks in the Healthcare Setting
Using the HVS screener modified with a three-month recall period window, we estimated that during 2021, 8.5% of English proficient health plan members aged 35-85 years who were not covered through California’s Medicaid insurance program had recently been or were currently food insecure. This is similar to the 9.6% estimate for California households based on the USDA Household Food Security Survey Module, under the national food insecurity estimate at 10.2%, and much lower than the approximately 25% of California households estimated to be food insecure at the end of 2020 when the full impact of the COVID-19 emergency was being felt.2,16 The lower estimate of food insecurity in this KPNC population is not surprising given the survey’s exclusion of non-English proficient adults and adults with very low-income covered by Medicaid. Compared to the general population of Northern California, the KPNC adult membership has a much lower proportion of adults covered by Medicaid and the Supplemental Nutrition Assistance Program (SNAP). 13 At the time of the survey, many COVID-19 relief measures were still in place for adults with a low income, such as pandemic EBT (P-EBT), expanded SNAP benefits, online SNAP, and additional fruits and vegetables for participants of the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC). These benefits may have increased food security for some individuals.
However, our results suggest that estimates based on the HVS screener alone likely underestimated food insecurity in this population, as an additional 5% of adults not identified through the HVS food insecurity measure got free food from a community organization during that same 3-month interval. This would have resulted in undercounts in population-level food insecurity estimates and reduced potential intervention paths for these patients beyond getting free food from a community organization (e.g., referral to SNAP, WIC, or other federal nutrition assistance resources).
Our study also estimated that nearly 13% of adults in the study population were nutrition insecure during the 3 months prior to the survey. In this population, while nearly three-fourths of adults who were food insecure were also nutrition insecure, only approximately half of nutrition insecure adults were also food insecure. The prevalence of food insecurity and prevalence of nutrition insecurity was similar among adults who were having difficulty “making ends meet.” However, among adults who reported that they usually had money left over at the end of the month, there was an approximately three-fold difference between prevalence of food insecurity and prevalence of nutrition insecurity. During the first year of the COVID-19 pandemic, many adults who would normally have been able to eat a healthy and balanced diet experienced difficulty accessing healthy foods due to concerns about potential exposure when shopping in grocery stores and using public transportation, as well as supply chain issues which limited the quantities, variety, and cost of many fresh foods.23,24 It is important to underscore that our survey was conducted shortly after communities were beginning to “re-open” due to the availability of high-quality masks and COVID-19 vaccines, and this likely reduced ready access to nutritious foods.
We found that 42.5% of adults who had acquired free food from a community-based organization were nutrition insecure during the same time period. While acquiring free food from a community-based organization helps to address food insecurity (having enough food), the nutritional quality of foods offered to users varies depending upon what is donated or can be cheaply procured, often resulting in fewer offerings of healthy foods like fresh fruits and vegetables. 25 Because nutrition insecurity was not being measured in U.S. national surveillance surveys and no validated nutrition insecurity measures were available at the time we conducted this study, no comparison data are available. Since the 2021 survey, 2 nutrition security measures have been released26,27; one has been evaluated across several public health settings 27 and the other has been validated, but not yet in healthcare settings. 26 Remarkably, food security has been measured on a national scale for more than 25 years. 11
The racial and ethnic disparities in prevalence of food insecurity and use of free food resources that we found in this non-Medicaid covered adult population were similar to those reported for populations that included low-income households. Specifically, compared to White adults, Black, Latino, and Asian/PI adults had a higher prevalence of food insecurity, of use of emergency food resources, and of nutrition insecurity. The higher prevalence of food and nutrition insecurity among these racial and ethnic groups paralleled the higher percentages of adults in these groups who were having difficulty making ends meet.
These findings demonstrate intersectionality. 28 During 2021, Black (19.8%) and Latino (16.2%) households experienced higher rates of food insecurity than White non-Hispanic (7.0%) in the U.S. 2 Importantly, during COVID-19 food insufficiency was measured alongside food security, and Native Hawaiian and Pacific Islander, Black, and American Indian and Alaska Native households had the highest rates of food insufficiency. Further, households with lower income and food insecurity also reported eating fewer fruits and vegetables than household reporting higher income. 29 At the root of these disparities is poverty, which is a multidimensional social condition that unequally impacts some minoritized racial/ethnic populations and influences dietary intake and related health outcomes.4,30 While healthcare providers can intervene to help patients address immediate food-related needs, food and nutrition insecurity will not be solved until these racial/ethnic disadvantages related to income inequality are systemically addressed on a societal level.
In our study, we found that nearly 20% of adults who had been diagnosed with diabetes, prediabetes, ischemic coronary artery disease, or heart failure were food insecure and 14% were nutrition insecure, including approximately 6% who had eaten less fruits, vegetables, and other healthy foods due to the cost. Further, Black and Latino adults with these diet-related cardiovascular conditions were more likely than White adults to be nutrition insecure. Zierath et al. (2023) surveyed Black adults and found that food insecurity was associated with coronary heart disease and heart failure. 31 In the U.S., when compared to non-Hispanic White adults, prevalence of cardiovascular disease is higher among Black and Latino adults, and diabetes prevalence is higher among Black, Latino, and Asian adults. 32 Screening for both food and nutrition insecurity is key to understanding the life context of patients who are having to manage or are at high risk for developing chronic diet-related health conditions.
Patient-Centered Approaches when Screening for Food and Nutrition Insecurity in the Healthcare Setting and Public Health Surveillance
Healthcare settings can play a role in addressing health disparities by implementing systematic approaches to screening for and addressing nutrition insecurity with a patient-centered approach.33 -35 This will include having follow-up interventions to connect patients with affordable, healthy, and culturally appropriate foods, along with providing ongoing patient education and access to healthcare services to manage diet-related chronic health conditions.
Cost is a major barrier to accessing healthy foods, but other barriers exist, including low-access food areas and inadequate or unaffordable transportation. 36 These barriers can be, in part, addressed by expanding access to healthy foods through food is medicine programs that provide free or subsidized fruit and vegetable prescriptions, home-delivered meals, medically-tailored meals, or food baskets. 37 For example, the Gus Schumacher Nutrition Incentive Program is funded through the Farm Bill to provide competitive grants for communities to implement produce prescription projects in healthcare settings. 38 Kaiser Permanente has also committed over $50 million to provide multi-year support for a Food is Medicine program serving Kaiser Permanente members and the broader community. 39
Some patients may require food skills education to equip individuals to shop for and prepare healthy foods. For example, patients can be educated about lower cost ways to achieve a healthy diet other than purchasing fresh produce, including bulk purchasing, buying frozen or low sodium/low sugar canned fruits and vegetables, and meal planning. Research demonstrates that individuals with a low income generally understand the components of a healthy diet and want to eat healthy, but face constraints to accessing and affording these foods. 40 Thus, nutrition education that is delivered in culturally appropriate ways should aim to empower individuals to make cost-effective shopping decisions in the context of their resources such as financial strain, food skills, transportation, food preparation and storage equipment, program enrollment, food preferences, and food availability in local area.
There has been growing interest among researchers, public health practitioners, and medical organizations to address nutrition insecurity as a social risk separate from food insecurity, as well as from federal entities as demonstrated with the White House Conference on Hunger, Nutrition, and Health.41,42 While validated nutrition insecurity measures are being developed for research and surveillance, there is also a need for a brief screening measure that can be added to current brief social risk screeners that also screen for food insecurity, financial strain, housing insecurity, and transportation risks. For this study, we used 2 questions to identify individuals who were acquiring free food from community emergency food resources and who were having a hard time accessing enough healthy food. Because these questions have a parallel structure to the widely used HVS screener, they can easily be incorporated with the HVS items into grid in print, online, and orally administered questionnaire formats. While these questions have not been validated against lengthier measures, they have demonstrated the ability to identify people with food and/or nutrition insecurity who would have been missed using the HVS alone.
Nutrition security is a nascent construct, and the research community is divided about its value as a measure separate from food security.43 -45 We believe that the low overlap of food insecurity and nutrition insecurity risk that we found in our study and the wide disparities we observed among vulnerable populations support the importance of screening for both food and nutrition insecurity in the healthcare setting.
The translational goal of this research was to inform recommendations to improve population-level estimates and patient screening for food and nutrition insecurity in healthcare settings. Based on our findings, we suggest that healthcare settings:
Include questions about acquisition of free food from community resources and nutrition insecurity alongside the current 2-item HVS to better identify patients with food-related social risks.
Implement education programs to educate patients and their healthcare providers about different ways to get and prepare culturally acceptable healthy foods on a limited budget (e.g., nutrition-equivalents to fresh fruits and vegetables).
Implement referral systems to connect food and/or nutrition insecure patients to programs in their community that provide access to free or affordable healthy food. These programs should include services that provide home-delivered groceries and prepared meals, food banks and public benefit programs, Food as Medicine programs, as well as activities to promote health food access in the food environment.
Strengths and Limitations
A strength of our study was the sociodemographically diverse study population with large enough subgroups to examine differences in food and nutrition insecurity prevalence estimates for middle-aged and older adults, 4 racial/ethnic groups, and different levels of financial strain. However, there are limitations that affect generalizability of results to other settings. These include survey data from 1 Northern California health plan, a relatively low survey response rate, and exclusion of adults whose preferred spoken and written language indicated in their EHR was not English, who had difficulty reading and completing an English-language questionnaire, who lacked a stable mailing address, or who were covered by California’s Medicaid program for very low-income individuals. We also lacked information about survey respondents’ enrollment in government benefit programs like SNAP and WIC that address food insecurity. However, we also view the study sample as a strength since there is a gap in information about non-Medicaid covered adults and their needs and risks around food and/or nutrition insecurity. Although food insecurity has been reported as high among the Medicaid-covered population (upwards of 20%), not all Medicaid enrollees are food insecure and not all individuals with food insecurity are enrolled in Medicaid. 46 Our Asian/PI subgroup was not sufficiently large to enable examination of differences in food and nutrition insecurity among Asian and Native Hawaiian/Pacific Islander ethnic groups. A recent study of low-income adults in California found that food insecurity and CalFresh (SNAP) participation rates varied among different Asian American communities, with low-income Filipino adults being disproportionately affected by food insecurity, and low-income Chinese and Korean adults having the lowest rates of CalFresh participation. 47 While the survey questionnaire used the standard wording for the validated two-item HVS screener to estimate food insecurity, modified to reflect a 3- rather than 12-month recall period in keeping with the survey’s other social risk measures, the questions used to estimate prevalence of acquiring free food from community resources and of nutrition insecurity have not been validated. Cognitive testing of these non-validated items is needed before these additional questions can be recommended for inclusion in social risk screeners.
Conclusions
Identifying and addressing food and nutrition insecurity is important for achieving optimal health for all and reducing racial/ethnic health disparities. Many healthcare settings are currently screening for food insecurity using the 2-item Hunger Vital Sign measure, but thus far there is no widespread screening for nutrition insecurity. Further testing of nutrition insecurity tools for screening is necessary. It is incumbent upon healthcare settings to expand universal screening for food-related insecurity to include use of free community-based resources and nutrition insecurity, to implement patient and healthcare provider education about different ways to obtain and prepare healthy, nutritious foods on a limited budget, and to connect food or nutrition insecure patients with internally sponsored and community-based resources that provide healthy, affordable food.
Footnotes
Acknowledgements
The authors wish to acknowledge appreciation for Richard W. Grant, MD MPH, the Co-Principal Investigator on the survey project; survey team members Teresa Y. Lin and Pete Bogdanos; and the Kaiser Permanente Northern California members who participated in the survey.
Authors’ Contributions
NG and CBS conceived the study design. NG collected and analyzed the data. NG and CBS interpreted the data. CBS wrote the first draft of the manuscript and NG contributed to subsequent drafts. All authors approved the final version of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Nancy Gordon received support for her work on this study from the Kaiser Permanente Northern California Community Health Program.
Ethics Approval and Consent to Participate
The Kaiser Permanente Northern California Institutional Review Board (KPNC IRB) approved use of the Social Risk Survey data and linkage of the survey data with respondents’ electronic health record (EHR) data for this study as meeting the ethical standards of the Helsinki Declaration of 1975, as revised in 2000. The KPNC IRB approved waived the requirements to obtain informed consent for the survey as allowed under {§46.116(d)} and to obtain Privacy Rule Authorization for use and disclosure of protected health information (PHI) as allowed under {45 CFR 164.512(i)(1)(i)}.
Consent for Publication
Not applicable
Availability of Data and Materials
The Kaiser Permanente Northern California Institutional Review Board has not provided approval for these survey data or variables derived from electronic health data to be placed in a public access repository. However, researchers can request access to use this study data by contacting the senior author (NPG) or the DOR Data Sharing Workgroup at