
Abstract
Food is medicine (FIM) initiatives are an emerging strategy for addressing nutrition-related health disparities increasingly endorsed by providers, payers, and policymakers. However, food insecurity screening protocols and oversight of medically-tailored food assistance programs are novel for many healthcare settings. Here, we describe the pre-implementation planning processes used to successfully engage federally-qualified health centers (FQHCs) across Kansas to develop new FIM initiatives. A Kansas-based philanthropic foundation facilitated pre-implementation planning for FQHCs over 17 months across 3 stages: 1) Community inquiry, 2) FIM learning event with invitation for FQHC attendees to request pre-implementation funding, and 3) Pre-implementation planning workshops and application assignments for FQHC grantees to develop a FIM implementation grant proposal. We evaluated satisfaction and perceived utility of these pre-implementation planning activities via post-workshop surveys and qualitative comparisons of FIM design components from pre-implementation and implementation grant applications. All 7 FQHCs attending the learning event applied for and were awarded pre-implementation planning grants; 6 submitted an implementation grant application following workshop completion. FQHCs rated pre-implementation support activities favorably; however, most clinics cited limited staff as a barrier to effective planning. As compared to pre-implementation planning grant proposals, all FQHCs elected to narrow their priority population to people with pre-diabetes or diabetes with better articulation of evidence-based nutrition prescriptions and intervention models in their final program designs. In the midst of a nationwide FIM groundswell, we recommend that funders, clinic stakeholders, and evaluators work together to devise and financially support appropriate pre-implementation planning activities prior to launching new FIM initiatives.
Keywords
Introduction
Hippocrates, the father of Western medicine, is attributed for saying, “Let food be thy medicine and medicine be thy food.” Over 2000 years later, conventional treatment guidelines for obesity, 1 diabetes, 2 hypertension, 3 and cardiovascular disease 4 all endorse the role of diet in the etiology and management of these conditions, yet routine nutrition assessment and counseling by providers during the patient encounter remains an exception, not the rule.5,6 Contemporary additions to treatment guidelines further emphasize the need to tailor care planning according to unmet social needs, including food insecurity, which can now formally be added to the healthcare record via a unique set of Z codes. 7 Given the strong connections linking food insecurity to diet, 8 in addition to its role as an independent risk factor for morbidity and mortality, 9 healthcare systems are increasingly recognizing the potential of nutrition security screening to better inform patient treatment plans for optimal outcomes. Additionally, the charitable food system has expanded food distribution sites to include healthcare systems and federally qualified health clinics (FQHCs) in some communities.10,11 However, these 2 systems have historically operated in silos, yet share a common element of reliance on philanthropic funding to pilot and expand novel initiatives.
Formally defined by the Aspen Institute Food & Society Program, food is medicine (FIM) represents a new innovation in healthcare involving “the intersection of food and health care” as a multi-sector strategy for health equity. 12 The most common approaches for programmatically operationalizing FIM include produce prescriptions, medically-tailored groceries, and medically-tailored meals that are initiated by a healthcare provider to prevent, manage, or treat diease. 12 Additionally, for the first time since 1969, the White House separately launched a nutrition security initiative in 2022 that aims to “end hunger and increase healthy eating and physical activity by 2030,” with the ultimate goal of decreasing diet-related disease among Americans. 13 Enthusiasm has rapidly blossomed within this space among various professional medical societies and foundations, including the American Heart Association’s Health Care by Food Initiative and Presidential Advisory statement, 14 a committed $100 million investment by Rockefeller Foundation for advancing the science of Food is Medicine, 15 and the American College of Lifestyle Medicine’s launch of a free “food as medicine” CME for clinicians. 16 Collectively, the political, medical, and philanthropic interests are primarily aligned to support substantial investment in FIM as a potential strategy for simultaneously tackling nutrition and health inequities. However, such innovations require support systems beyond financial investments, including other forms of capacity building for these food and healthcare delivery systems. 17
Nutrition prescriptions for chronic disease (which collectively support achievement of a therapeutic eating pattern) are well established in scientific evidence and share many common dietary targets, such as increased intake of fiber-rich foods and reduction of ultra-processed foods.18 -20 However, decisions about which nutrition prescriptions and patient populations to prioritize, who should initiate the prescription during a routine office visit, and what type of food assistance mechanism (ie, medically-tailored meals, groceries, or produce vouchers) and complementary support strategies are best for supporting behavior change (eg, culinary medicine classes) to produce a specified health outcome(s) are all equally important elements of FIM program design. All these contextual elements are highly patient- and community asset-specific. Person-centered design requires development of programs that places patient needs first 21 and can help to answer all these important planning decisions. Further, rural America faces many geographic barriers to healthy food access that urban-based programs may not experience,22,23 yet rarely do philanthropic grants allow planning time for these critical elements, including solicitation of input from patients and implementation staff, as fundable program activities.
Despite many types of evidence-informed interventions and programs that are available to the healthcare sector, the estimated start-up (initial implementation) rate of such initiatives is quite low. 24 Pre-implementation planning may help to address this challenge and involves naming and framing of the problem, identification of stakeholders, and consideration of evidence-based practices as essential prerequisites prior to the implementation of a new clinic-based initiative.25,26 During this process, pre-implementation occurs through a series of stages including engagement, consideration of feasibility, and readiness planning. 24 These important steps not only help to ensure essential elements are in place for the immediate viability of new programs (ie, ensuring readiness for organizational change), but they also can help to lay the foundation for the long-term sustainability of programs as well as help an organization decide whether its in their best interest to move ahead with implementation of the program. Participation in pre-implementation planning is strongly associated with the start-up of a new evidence-informed programs, as well as mastering full competency in delivery of that program. 24 Pre-implementation planning is arguably most critical when designing new patient services that require cross-sector collaborations, such as food systems procurement of specific foods to meet individualized nutrition needs of patients with complex health conditions.
The objective of this community case study is to describe the pre-implementation planning methods used in Kansas to initiate a statewide, multi-clinic FIM initiative. We also summarize findings from our formative evaluation of the pre-implementation training workshops and assignments, including clinic stakeholders’ perceived utility, satisfaction with, and completion of the planning activities and materials. Finally, we aim to evaluate the impact of the pre-implementation planning on shaping the direction of each clinic’s chosen population, FIM design approach, and selected health outcomes.
Methods
Community Overview and Partnerships
This project takes place in collaboration with a cohort of Federally Qualified Health Centers (FQHCs) with operations across 7 diverse counties across Kansas, a state where all but 3 of 105 counties are classified as rural (Figure 1). Known for its abundance of fertile agricultural land and resources, Kansas generates more than $18 billion in agricultural revenue each year, with family-owned farms and ranches representing the backbone of all agricultural production. 27 Despite this appearance of plentiful resources, poverty, limited access to healthy foods, and poor health outcomes continue to be a concern, particularly for frontier and rural counties across the state. For example, 1 in 10 Kansan households experience food insecurity each year, 28 and only 6.5% of adult Kansans meet the minimum daily intake recommendation for fruits and vegetables. 28 Rates for obesity, diabetes, and cardiovascular disease either mirror or exceed the national average. 28

Kansas-area food is medicine pre-implementation planning sites. Note: The Index of Relative Rurality (IRR) is a continuous measure of rurality between 0 (low level of rurality, ie, urban) and 1 (most rural) based on population size, density, remoteness, and built-up area. Counties with a score of >0.4 can be classified as rural. 29
This project is funded through Sunflower Foundation, a statewide health philanthropy established in 2000 with the mission “to serve as a catalyst for improving the health and wellbeing of all Kansans.” Sunflower’s approach to grantmaking involves eliciting information from community partners to better understand unmet needs, creating an environment of co-learning through foundation-sponsored Learning Collaboratives, and investing in long-term systems change with strategies derived from this process. 29
Pre-Implementation Planning Stages
Pre-implementation planning was achieved through 3 key stages initiated by the Foundation: Community inquiry, one-day stakeholder learning event, and pre-implementation training workshops (Figure 2).
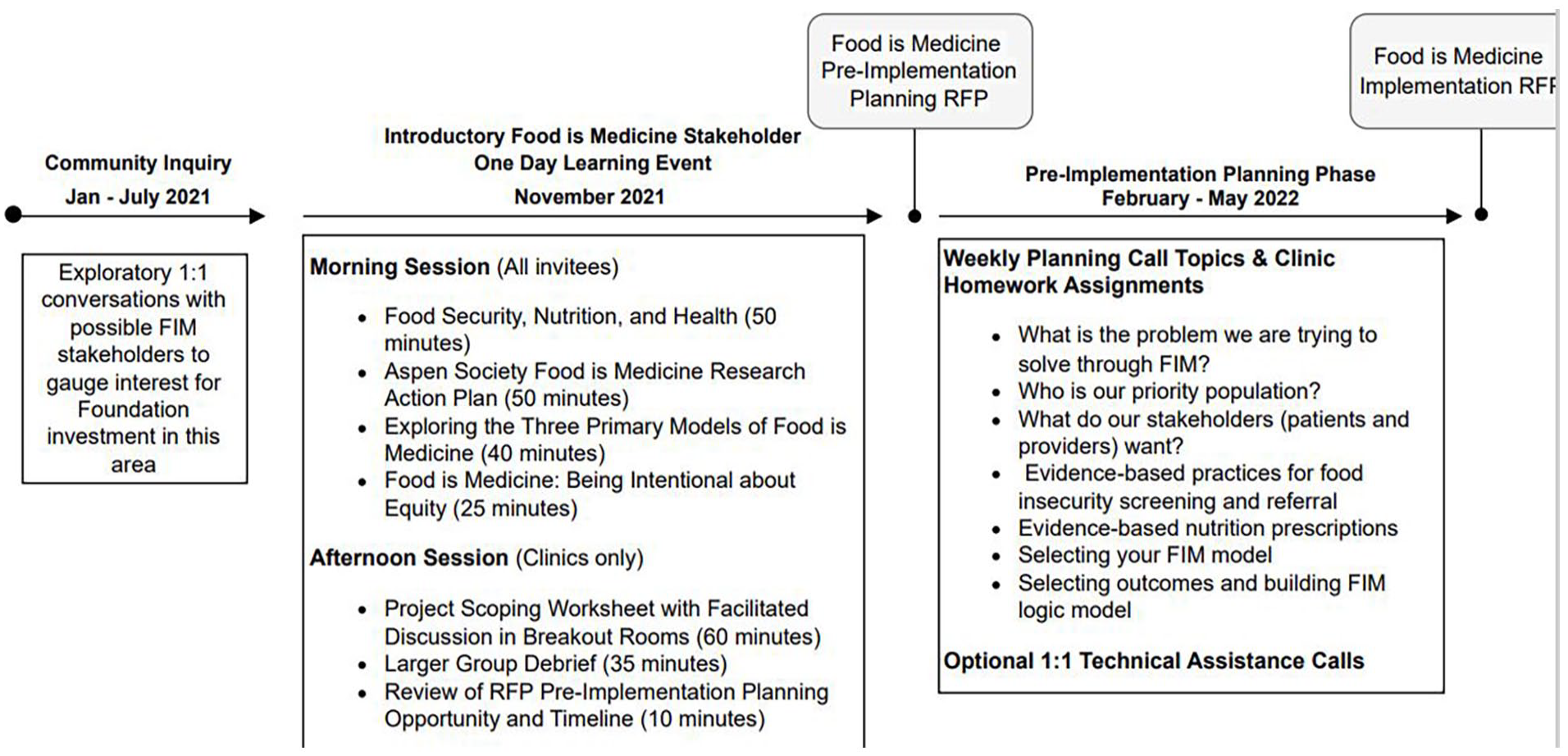
Overview of pre-implementation planning approach for food is medicine (FIM) interventions across multiple clinic sites in Kansas.
Community inquiry
Program staff at Sunflower Foundation had been in conversation with multiple Kansas FQHCs over the years about the integration of food and nutrition into clinics with a known history of delivering team-based, integrated primary and behavioral care. Through informal, one-on-one interviews with FQHC leadership, foundation staff gauged community interest and needs regarding initiation of formal FIM activities. Conversations covered topics of each clinic’s past, current, and interested future efforts within the areas of charitable food, nutrition education, and how to address health-related social needs (HRSNs) as well as each clinic’s philosophy toward risk and innovation. Foundation staff knew from 2 decades of work with healthcare clinics that these established “Early Adopters” would most likely be the most receptive entities to explore new ideas (ie, innovations)30,31 and provide iterative feedback to inform future funding strategies. Kansas currently has 20 FQHCs, many with satellite clinics, with the vast majority on the more populous eastern side of the state. Seeking a diversity in patient demographics as well as geographic-setting diversity (urban, rural, frontier), foundation staff invited 7 FQHCs with operations in 7 different counties to participate in the subsequent FIM planning stages.
FIM stakeholder virtual learning event
Between 2 and 8 participant representatives from each of the 7 FQHCs participated in a Learning Event sponsored by the foundation in November 2021. These representatives included direct care providers (nurses, pharmacists, physicians, physician assistants, nurse practitioners, nurse midwife, behavioral health specialists, therapists, community health workers) and clinic leadership (chief administrative, operations, compliance, marketing, development, and executive officers; grant manager; wellness coordinators). Additional stakeholder attendees included Kansas area food banks, tribal food system programs, and representatives from SNAP-Ed, health insurance, managed care organizations (MCO’s), state agencies and other health funders. Sessions were facilitated by regional and national experts on FIM research, intervention design, and policy (authors MSW and KB and those named in acknowledgements) and by Sunflower Foundation program officers (authors EB and BS). The primary purpose of the event was to establish a mutual understanding of FIM, including definition, rationale, benefits, implications for equity, knowledge gaps, and high-level design considerations (Figure 2). All FQHCs that participated in the event became eligible to submit an application for a $5000 to $7500 FIM pre-implementation planning grant designed to provide clinic personnel with protected time to explore feasibility and design considerations for a future FIM initiative at their clinic. In this application, clinics were asked to describe their anticipated priority population(s) and nutrition/food prescriptions that might produce an expected health impact.
FIM project pre-implementation facilitated workshops
All 7 FQHCs applied for and were awarded the FIM planning grant. From February-May 2022, clinics participated in 12 weekly, 1-hour virtual sessions spanning 4 main elements of FIM program design that also represented portions of a future FIM implementation grant application. Between 1 and 4 clinic representatives attended each virtual session. As possible food providers for future FIM interventions, food bank representatives also participated in training sessions. Complementary application “homework” assignments were designed by facilitators (MSW and KB) for FQHC participants to complete with clinic staff as part of the planning process. These application assignments emphasized participatory approaches in program design that included direct input from patients and clinical stakeholders via semi-structured interviews. Additional assignments included electronic health records review to identify and quantify patients within clinic population who may benefit from FIM, review and revision of current food insecurity screening and response procedures, and logic model design. One-on-one technical assistance consultations were available to participating FQHCs as an optional activity. Many of the key recommendations for the planning and evaluation of FIM interventions as detailed in the Aspen Institute Food is Medicine Research Action Plan 12 were also incorporated into training workshops and homework assignments. Upon completion of the pre-implementation planning workshops that concluded with formal presentations of each clinic’s FIM program logic model, clinics were invited to apply for a 1 year, $88,000 FIM pilot implementation grant. In this grant application, clinics were asked to further expand upon and provide rationale for their priority population(s), FIM model, and expected health impact. Clinics were allowed to change any of these elements from previous responses in their FIM pre-implementation planning grant based on key learnings from the pre-implementation planning workshops (Figure 2).
Formative evaluation
Following the pre-implementation planning workshops, clinics were invited to complete a post-workshop satisfaction online survey to evaluate the impact of the workshops on that clinic’s FIM program planning. We used a modified version of the training evaluation framework developed by Kirkpatrick 32 to develop questions that focused on each organization’s collective reaction, learning, and behavior as related to the training (Supplemental File for complete copy of survey with response options). Most questions provided 5-point Likert-type scale response options to evaluate reaction and learning with remaining questions asking organizations to report on time spent and completion status of homework planning assignments. The survey also included 2 open-ended questions. The first open-ended question asked clinics to specifically describe the most challenging aspects of the planning phase. An additional open-ended question concluded the survey asking for any additional feedback about the organization’s experience with the training series. Clinic teams received questions in advance and were asked to submit 1 survey on behalf of their pre-implementation planning team. We summarized results for each survey item using descriptive statistics including percentages for Likert-type scale questions and means for numerical responses. Open-ended feedback was reviewed by the training team for the purposes of gaining further insights into Likert-type scale responses. 33
To further evaluate the impact of pre-implementation planning on each clinic’s ability to identify the problem and evidence-based practices to address the problem, we additionally reviewed each clinic’s pre-implementation and subsequent implementation grant applications to evaluate progression of each clinic’s planning. We evaluated each clinic’s set of applications for differences in their chosen priority population(s), planned nutrition or food prescriptions, and expected health impact to determine whether and how each clinic’s FIM program design evolved during their pre-implementation planning phase. Additionally, we counted the number of organizations that elected to move forward with FIM implementation via submission of an implementation grant application and those that decided they were not yet ready to proceed.
Results
Survey Responses
Each of the 7 participating clinics completed the organizational survey. Overall, participants responded favorably to the pre-implementation planning workshops. All participants strongly agreed or agreed that training sessions were enjoyable, met their planning team’s expectations, and were delivered in a clear manner. All but 1 organization strongly agreed that sessions covered all areas of information needed to plan their FIM pilot, with the remaining organization indicating in a follow up question that more time was needed for their clinic to discuss personal design considerations, for example, types of foods offered. Clinics also responded favorably to application assignment “homework” materials, with all clinics agreeing that instructions were clear, provided the opportunity to apply new concepts, and explore their priority population more critically. Though nearly all homework assignments were rated as extremely useful or very useful, the most highly rated assignments were 1) development of a FIM pilot logic model and 2) 2 rounds of patient interviews about their preferences for the FIM pilot (Table 1).
Formative Evaluation Survey Results: Pre-Implementation Planning Workshop Training for Food Is Medicine, n = 7 FQHC Organizations.

Question designed to assess: aReaction, bLearning, cBehavior
Homework completion rates for the 7 assignments were acceptable: all but 1 clinic fully completed the first homework assignment, 100% of clinics completed the second, third, and final logic model assignments (Table 2). More than half of clinics (n = 4, 57%) completed the remaining 3 assignments. For those clinics unable to fully complete these assignments, limited staff time was the reported barrier for all 3 clinics. Completion time for the homework activities varied by assignment, ranging widely between 1 and 17 hours across all assignments and clinics.
Homework Completion: Pre-Implementation Planning for Food Is Medicine (FIM), n = 7 FQHC Organizations.

Question designed to assess Behavior.
Each clinic described their most challenging aspects of the pre-implementation planning process, including 5 clinic descriptions of limited staff time to plan the project outside of the scheduled workshop training. As described by 1 clinic:
You realize how time consuming some of the logistical elements can be. Philosophically it feels reasonably straightforward, but you soon come to realize all the details involved. That is really the value of the planning sessions. It really pushes you to work this out ahead of time, which should increase the odds of success.
While most clinics were working to develop entirely new programs and procedures, 1 clinic commented on the unique challenges in revising their clinic-based food pantry operations to incorporate a FIM approach.
[Clinic name] has an existing food pantry that started in 2020. It was challenging to rethink how to implement some of the improvements after making much progress and gaining organizational “buy-in” over the past 18 months. The thought of asking staff to make new changes seemed daunting but exciting to be able to implement some of the new strategies!
The remaining clinic described language barriers that made patient interviews difficult:
Our promotoras [Spanish-speaking community health workers] helped, but the language and cultural differences made it difficult [for the English-speaking FIM planning team].
Influence on Each Clinic’s Final FIM Approach and Newly-Identified Implementation Needs
Clinics indicated through the survey that both the workshops and the application assignments were influential in the direction and design plans of the FIM intervention (Table 1), and all but 1 clinic elected to move ahead with an FIM implementation grant proposal. A comparison of each clinic’s responses (n = 6) to questions in their pre-implementation and implementation grant applications further demonstrated changes and/or improved clarity pertaining to each clinic’s chosen priority population(s), nutrition or food prescription, and expected health impact (Supplemental Table). Pre-post changes were most notable in the final selection of the patient population. Patient populations originally encompassed people with hypertension, pregnancy, mental health, obesity, eating disorders, pre-diabetes, and diabetes in initial grant applications with all clinics choosing to narrow their priority population to people with pre-diabetes or diabetes in their final program design. For several clinics, food/nutrition prescriptions or planned outcomes were unspecified in their pre-implementation grant proposals and all clinics described these components in their implementation proposals. The FIM model ultimately selected by FQHCs varied, with most clinics choosing medically-tailored groceries with several choosing hybrid models, for example, step down from medically-tailored meals to medically-tailored groceries. Anticipated outcomes in the final applications all included reduction in hemoglobin A1c with some clinics adding additional outcomes such as weight, blood pressure, mental health, quality of life, and self-efficacy for healthy eating.
Clinics identified multiple implementation support needs for their final projects as reported in their survey responses (Figure 3). Collaborative learning events and specific list of recommended food items were requested by all clinics and the majority requested evaluation support, continued access to 1:1 technical support from trainers, and guidance from a registered dietitian for program planning elements.
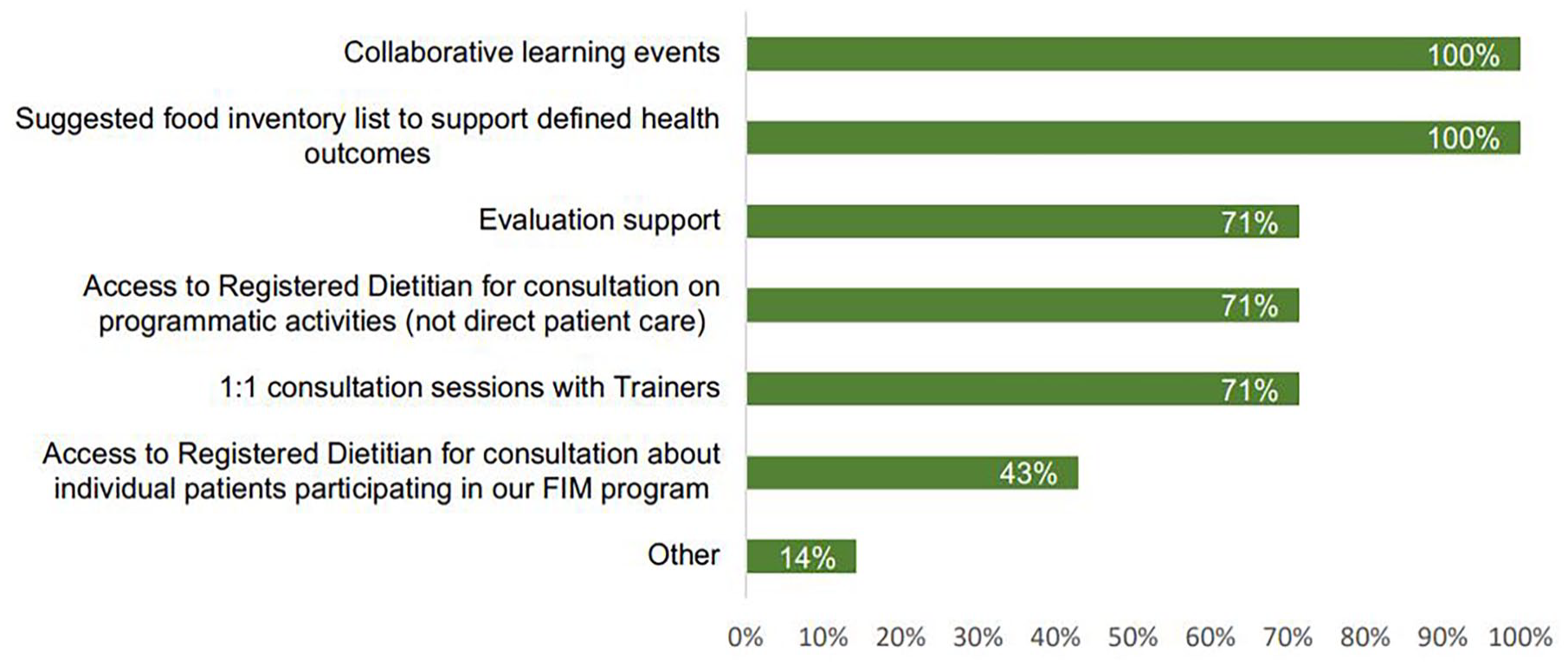
Food is medicine implementation support needs, n = 7 Federally Qualified Health Centers (FQHCs) in Kansas.
Discussion
This paper highlights the components and formative evaluation findings of a pre-implementation training program designed to prepare FQHCs for the successful launch of new FIM initiatives throughout the state of Kansas. Participating organizations expressed high satisfaction with the training and completed most or all of the pre-implementation planning assignments. Six of the FQHCs opted to move forward with FIM implementation upon workshop conclusion with the remaining FQHC concluding it was not yet organizationally-ready for a FIM initiative. These findings suggest that structured opportunities, including a series of 1-hour virtual learning modules, application assignments, and optional technical assistance calls, can effectively support clinic leaders to develop new FIM programs and provide the valuable reflection time needed about whether its in the best interest of organizational stakeholders to proceed with such plans.
FIM involves several components that are novel to many healthcare settings, including routine food insecurity screening, nutrition assessment, and oversight of medically-tailored food assistance programs. FQHCs participating in the program grappled with institutional policies, screening procedures, and how to redesign existing clinic workflows amid their planning process. Application assignments required FQHCs to identify valid food insecurity screening tools, engage with patient and provider stakeholder groups to understand their interest and needs pertaining to FIM, define new FIM roles and responsibilities for existing clinic staff, and explore how existing programming (eg, cooking classes, diabetes education) could be modified or leveraged to boost the impact of FIM. While all FQHCs found these application assignments to be influential in their final chosen priority population and FIM program design, they also helped FQHCs to identify what additional implementation resources would first be needed. Specifically, clinics identified the need for better access to registered dietitians, evaluated the potential for community health workers (CHWs) to assist with program activities, and explored funding or reimbursement opportunities for such roles.
These recent clinic-level FIM planning conversations occurred amid the ongoing national discussion about multi-sector commitment to FIM programming, including the White House Conference on Hunger, Nutrition and Health, 13 guidance by nonprofit groups and think tanks like the Aspen Institute, 12 recommendations for health insurance companies to cover nutrition incentives, 34 as well as state-level policies for expanding Medicaid coverage of CHW services. 35 Some of the national and state policy decisions over the next few years will be informed by the successes (and failures) of these novel FIM programs, which underscores the importance of evidence-informed, scalable, and sustainable program design. FQHCs were reminded of the national and regional context in which they approached FIM during the one-day, multi-sector stakeholder learning event that preceded the 12-week facilitated workshops. Although FQHCs would be designing FIM programs tailored to their specific clinics, they were introduced to evidence-based FIM approaches used across the country and to regional stakeholders (food banks, payors, social service providers) who are excited by the idea of FIM and could become clinic partners.
The majority of FQHCs participating in this pre-implementation program serve patients in rural Kansas. Most published FIM interventions have taken place in urban environments,12,36,37 which limits their practicality for many rural communities. Anecdotally, all 6 clinics that moved ahead with FIM programs have expressed desire for more collaborative learning and networking opportunities. Since opportunities for health are often rooted at the state-level through geographic and political influences, we recommend that healthcare authorities and medical associations form working groups at the state-level to better understand implementation challenges, opportunities, and ultimately best practices for different types of healthcare settings.
The next stage of this project will focus on feasibility and effectiveness of the FIM interventions currently underway at each of the 6 participating FQHCs, thereby contributing useful information to this gap in the literature. The FIM expert team who led training during the pre-implementation phase have transitioned to leading the evaluation of the implementation, which will include evaluation of the essential stages of “start-up” implementation, including the status of staff hiring/training, fidelity monitoring, launch of services, and ongoing program delivery. 24 Since all clinics independently decided to narrow their population of interest to patients with type 2 diabetes or pre-diabetes, the evaluation design will employ shared outcome metrics from similar populations across sites (pre- and post-intervention food security, F/V and fiber intake, A1c and other health outcomes). Implementation evaluation will draw from a combination of qualitative (provider, staff, and patient interviews) as well as quantitative data sources to ensure full assessment of the barriers and facilitators to project effectiveness and sustainability.
Strengths and Limitations
A major strength of this community case study is that it describes processes used in a real-world setting, which will hopefully offer primary care and other health providers with tangible examples of how the pre-implementation process might be achieved within their practice. One potential key limitation is the self-selection bias of the FQHCs that participated in the pre-implementation planning stage. The funder invited clinics based on several factors, including a clinic’s demonstrated ability to innovate and take risks; thus, results cannot be easily extrapolated to all other clinics. It also speaks to the limitations of philanthropic funding, which tends to mitigate risk by selecting grantees with the highest potential for success. Future studies could randomly assign clinics to receive pre-implementation planning or to immediately proceed with implementation to determine whether this additional step is associated with better outcomes, including patient and healthcare provider satisfaction with the FIM program. Another important limitation is that we did not conduct a separate pre-implementation planning series for FIM stakeholders within the food system. While key food bank collaborators were invited to attend and participated in the pre-implementation planning sessions, they did not complete any food system-specific planning assignments or participate in the evaluation of the training series. The pre-implementation planning worksheets produced through this project could and should be expanded in future projects to more explicitly incorporate food systems planning simultaneously alongside clinics.
Conclusion
In the midst of a nationwide FIM groundswell, we recommend that funders, clinic stakeholders, and evaluators work together to devise and support appropriate pre-implementation planning activities prior to the launch new FIM initiatives. Regardless of the healthcare setting or patient population, we recommend that clinics considering FIM programs first invest 6 months to 1 year for this planning process. Minimum planning components during this time should accomplish: (1) understanding FIM needs and preferences from the patient perspective; (2) confirming clinic/provider buy in and program feasibility within clinical workflows and healthcare team capacity; (3) verifying community capacity through mapping the landscape of food sources and food procurement ability of nutrition prescription suppliers. These initiatives can help stakeholders to better articulate the FIM problem, make informed decisions around FIM activities, and decide whether it is in the best interest of patients and providers to proceed with implementation. Funders should consider the potential benefits of pre-implementation planning grants, including the opportunities they can provide to engage with patient stakeholders to ensure planned activities are responsive to community needs. Federal funding programs should also consider the importance of pre-implementation training and planning for produce prescription and other FIM projects, and incentivize process and planning outcomes as much as effectiveness outcomes.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241241465 – Supplemental material for Planting Seeds for Food Is Medicine: Pre-Implementation Planning Methods and Formative Evaluation Findings From a Multi-Clinic Initiative in the Midwest
Supplemental material, sj-docx-1-jpc-10.1177_21501319241241465 for Planting Seeds for Food Is Medicine: Pre-Implementation Planning Methods and Formative Evaluation Findings From a Multi-Clinic Initiative in the Midwest by Marianna S. Wetherill, Kristina M. Bridges, Gabrielle E. Talavera, Susan P. Harvey, Brandon Skidmore and Elizabeth Stewart Burger in Journal of Primary Care & Community Health
Supplemental Material
sj-docx-2-jpc-10.1177_21501319241241465 – Supplemental material for Planting Seeds for Food Is Medicine: Pre-Implementation Planning Methods and Formative Evaluation Findings From a Multi-Clinic Initiative in the Midwest
Supplemental material, sj-docx-2-jpc-10.1177_21501319241241465 for Planting Seeds for Food Is Medicine: Pre-Implementation Planning Methods and Formative Evaluation Findings From a Multi-Clinic Initiative in the Midwest by Marianna S. Wetherill, Kristina M. Bridges, Gabrielle E. Talavera, Susan P. Harvey, Brandon Skidmore and Elizabeth Stewart Burger in Journal of Primary Care & Community Health
Supplemental Material
sj-pdf-3-jpc-10.1177_21501319241241465 – Supplemental material for Planting Seeds for Food Is Medicine: Pre-Implementation Planning Methods and Formative Evaluation Findings From a Multi-Clinic Initiative in the Midwest
Supplemental material, sj-pdf-3-jpc-10.1177_21501319241241465 for Planting Seeds for Food Is Medicine: Pre-Implementation Planning Methods and Formative Evaluation Findings From a Multi-Clinic Initiative in the Midwest by Marianna S. Wetherill, Kristina M. Bridges, Gabrielle E. Talavera, Susan P. Harvey, Brandon Skidmore and Elizabeth Stewart Burger in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The authors recognize the significant time and energy put forth into the planning of food is medicine initiatives by leadership at Hoxie Medical Clinic, Heartland Community Health Center, Genesis Family Health, Community Health Center of Southeast Kansas, HealthCore Clinic, Health Ministries Clinic, and Vibrant Health. The authors thank those who shared their wisdom and expertise during the intial learning event and preimplementation planning workshops, including Sarah Downer, JD, Trina Ragain, MSPH, of Eccentricity Consulting, LLC, and Michelle Axe, MS, CHES, of ChristianaCare. We also acknowledge staff at the Kansas Food Bank and Harvesters for co-exploring how charitable food systems can support food is medicine initiatives. We also thank K-State Research & Extension SNAP-Ed for identifying community collaboration opportunities and Tandy Rundus, MS, RD/LD, for her thoughtful review of the manuscript. Finally, the authors thank Micah Hartwell, PhD, for creating ![]() .
.
List of Abbreviations
Food is Medicine (FIM); Federally-qualified health centers (FQHCs)
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Marianna S. Wetherill, Dr. Kristina M. Bridges, and Dr. Susan P. Harvey received financial support from the Sunflower Foundation for their work as advisors for the initiative described in this manuscript. There are no other competing interests to report.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Sunflower Foundation.
Ethical Standards Disclosure
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the University of Oklahoma Health Sciences Center Institutional Review Board.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.