
Abstract
Introduction:
It is unclear whether the risk of suicide differs among individuals with only physical health condition, those with only mental health conditions, and those with both types of conditions (multimorbidity) and how emotional social support modifies these associations. This study aimed to examine differences in the association of suicidal ideation with the presence of only physical health conditions, only mental health conditions, and multimorbidity and the modifying role of emotional social support in these associations.
Methods:
A cross-sectional survey was conducted between August and September 2023 in a Japanese rural town to collect data. The exposure variable was the health condition, and it was classified into 4 groups: disease-free, only physical health conditions, only mental health conditions, and multimorbidity. The outcome variable was suicidal ideation. The data collected were analyzed using multivariate logistic regression analysis and stratified analysis.
Results:
Suicidal ideation was found to have a significant positive association with the presence of only mental health conditions and multimorbidity. These associations remained unchanged in the absence of emotional social support. However, the odds ratio for the only mental health conditions group decreased in the presence of emotional social support, while the odds ratio for the multimorbidity group remained significantly higher.
Conclusions:
Suicidal ideation is positively associated with the presence of only mental health conditions and multimorbidity, but emotional social support modifies only the association between suicidal ideation and the presence of only mental health conditions. These results suggest that it may be important to identify the type of social support one needs based on one’s health condition to prevent suicide.
Introduction
Suicide is one of the leading causes of death worldwide, accounting for more than 700 000 deaths annually. 1 In 2016, the global suicide rate was approximately 10.6 per 100 000 people, with variations across regions and demographics. 2 However, this rate decreased by 36% from 2000 to 2019. 1 Although Japan’s suicide rate is higher than that of other high-income countries, it also showed a decline during this period.3,4 Considering that suicide is a preventable cause of death, suicide prevention strategies are essential.
The major risk factors for suicide are a history of suicidal ideation and suicide attempts.5 -9 Given that suicidal ideation typically precedes suicide attempts and completed suicide, it is crucial to identify individuals at high risk of suicidal ideation. 5 The etiology of suicide is complex and involves multiple factors, such as mental and physical health conditions, socioeconomic status, and cultural and political factors. 10 Mental health conditions, such as depression and schizophrenia,11 -16 and physical health conditions, such as chronic diseases, cancer, and stroke,12,17 -19 have a particularly significant impact on suicidal ideation and behaviors. In fact, one study found that the population attributable risk of suicidal ideation is the highest in depression (45.7%), followed by physical health conditions (19.4%). 20 This finding indicates that the impact of mental health conditions on suicidal ideation is more than twice that of physical health conditions. Therefore, the risk of suicidal ideation may differ between individuals with only physical health conditions (hereafter, OPHC), those with only mental health conditions (hereafter, OMHC), and those with both conditions (multimorbidity). Previous studies have indicated that the risk of suicidal ideation is similar among individuals with OMHC and those with multimorbidity but higher than the risk among individuals with OPHC.21,22 Few studies have examined the association of suicidal ideation with the presence of OPHC, OMHC, and multimorbidity. Therefore, there is little knowledge of how the risk of suicidal ideation differs among individuals with OPHC, those with OMHC, and those with multimorbidity.
Social support is a multidimensional concept involving emotional, instrumental, and informational social support, and it mitigates the risk of suicidal ideation.23 -25 Emotional and informational social support play a more protective role against suicidal ideation than instrumental social support,23,26 whereas instrumental social support plays a more protective role against completed suicide. 27 This is because emotional and informational social support are more beneficial against depression than instrumental social support26,28 and modifies the association between depression and suicidal ideation.26,29,30 However, the previous study has reported that informational social support modified the risk of suicidal ideation in individuals with moderate depression but not in those with severe depression. 26 Therefore, it is important to differentiate between emotional, instrumental, and informational social support in the context of suicidal ideation. However, several systematic reviews and meta-analyses reported that most studies examining the association between social support and suicidal ideation addressed emotional social support, with few studies addressing instrumental and informational social support.23 -25 Therefore, this study focused on emotional social support, for which the evidence is sufficient.
As above, emotional social support plays a protective role in the association between mental health conditions and suicidal ideation. Individuals with physical health conditions can also experience mental health problem, such as depression, leading to the state of multimorbidity. Consequently, they might be affected in the same way as individuals with mental health conditions or those with multimorbidity.11,21,22 However, it remains unclear whether emotional social support plays the same role in the association of suicidal ideation with OPHC, OMHC, and multimorbidity.
Therefore, this study aimed to investigate differences in the association of suicidal ideation with the presence of OPHC, OMHC, and multimorbidity and determine whether emotional social support plays a modifying role in these associations.
Methods
We adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines in the design and conduct of this study.
Study Design and Data Collection
We conducted a cross-sectional, self-administered questionnaire survey anonymously in a rural area: the Akita Prefecture in Japan. The anonymous questionnaire survey was originally designed to develop suicide countermeasures for people living in the area based on Japan’s General Principles of Suicide Countermeasures Policy. 31 To ascertain the prevalence of suicidal ideation with an accuracy of 3.7% and a 1% margin of error, 32 the required sample size was 2028. The predicted response rate in the rural area was approximately 40%. Based on this, we set the sample size to be 5000. Employing stratified random sampling based on the sex and age distribution in the area, we sampled 5000 residents aged 20 to 84 from a population of approximately 14 000 individuals. These individuals were selected using the basic resident register managed by municipalities. This register contains information about one’s date of birth, sex, and address. We excluded individuals who were certified as support level 2 or higher (ie, those who had a functional disability) according to the Japanese Long-Term Care Insurance (LTCI) system because they could not complete the survey by themselves. The LTCI is a mandatory form of social insurance aimed at assisting frail and older adults with activities of daily living.33 -35 This system uses a nationally uniform standard for functional disabilities.
The questionnaire was delivered between August and September 2023. The questionnaire inquired about demographic data, physical and mental health conditions, health habits, emotional social support, and suicidal ideation. This study was approved by the Institutional Review Board of the Akita University Medical School (approval number: 3008). Informed consent was obtained from the participants.
Variables and Measurements
We collected data on age, sex, physical and mental health conditions, suicidal ideation, emotional social support, marital status, subjective economic status, and self-rated health status. The exposure variables were self-reported physical and mental health conditions. The participants were asked to select the health conditions that applied to them: cancer, endocrine disorders (e.g., diabetes and thyroid disorders), respiratory disorders, circulatory disorders (including high blood pressure), immune disorders, blood disorders (e.g., leukemia and hemophilia), kidney disorders, gynecological disorders, depression, and mental disorders other than depression. Following previous studies,21,22 we classified participants into 4 groups. Individuals who had not selected any health condition were considered “disease-free.” Those who had selected 1 or more physical health conditions were considered as those with OPHC. Those who had selected 1 or more mental health conditions were considered as those with OMHC. Finally, those who had selected 1 or more physical and mental health conditions were considered as those with multimorbidity.
The outcome variable was suicidal ideation during the previous month. The participants were asked, “Did you think about committing suicide in the past month?” The response options were “yes,” “no,” or “unsure.” If 1 answered “yes,” 1 was considered to have suicidal ideation. We used suicidal ideation to predict suicide risk because suicidal ideation occurs before a suicide attempt or completed suicide.36,37 Additionally, a single item—the presence or absence of suicidal ideation—was adopted as the measurement tool because we surveyed the general public and, from an ethical standpoint, this item is relatively easy to answer as opposed to items on suicide plans or suicide attempts. To determine the presence of emotional social support, the participants were asked, “Do you have someone who listens to and understands your complaints, worries, and hardships?” The response options were “yes,” “somewhat yes,” “somewhat no,” “no,” or “unsure.” The responses of “yes” or “somewhat yes” denoted the presence of emotional social support.
Data Analysis
To derive baseline characteristics, we determined the distribution of respondents based on age (20-29, 30-39, 40-49, 50-59, 60-69, ≥70), sex (male, female), marital status (married, unmarried, widowed or divorced, other or data missing), subjective economic status (good, poor, data missing), self-rated health status (good, average, poor), and emotional social support (present, absent) in all health condition groups: those who were disease-free, those with OPHC, those with OMHC, and those with multimorbidity.
To examine the association of suicidal ideation with the health condition groups, we conducted a multivariate logistic regression analysis and estimated odds ratios (ORs) and 95% confidence intervals (CIs). The following 3 models were employed. Model 1 was a crude model. In Model 2, adjustments were made for age and sex. In Model 3, adjustments were made for marital status, subjective economic status, and emotional social support in addition to age and sex. In each model, the disease-free group was set as the reference group (OR = 1.00).
To test whether emotional social support modifies the association of suicidal ideation with the health condition groups, we conducted a stratified analysis based on the presence and absence of emotional social support. All statistical analyses were performed using the IBM SPSS Statistics version 28 (IBM SPSS Software Group, Chicago, IL, USA). All statistical tests were two-sided analyses, and differences were considered significant at P < .05.
Results
We received 2213 responses, making the response rate 44.3%. Among these responses, we excluded those that had no data on suicidal ideation (n = 118), health conditions (n = 57), emotional social support (n = 107), sex (n = 16), or age (n = 2). Finally, the responses of 1913 individuals were included in the analysis (Figure 1).

Flowchart of selecting the study sample.
The baseline characteristics of the participants are detailed in Table 1. Among 1913 respondents, 45 (2.4%) reported suicidal ideation. The number of participants in the disease-free, OPHC, OMHC, and multimorbidity groups was 1016, 802, 53, and 42, respectively. Individuals with OMHC were likely to be younger than those with OPHC and multimorbidity. Individuals with multimorbidity were more likely to be female, while those with OMHC were more likely to be married. The proportion of individuals with a poor subjective economic status was higher in the OMHC and multimorbidity groups than in the other groups. The proportion of individuals with a poor self-rated health status was the highest in the multimorbidity group, followed by the OMHC and OPHC groups. The proportion of individuals who had emotional social support was the highest in the OMHC group, followed by the multimorbidity and OPHC groups.
Characteristics of the Respondents Based on the Health Condition Group (n = 1913).
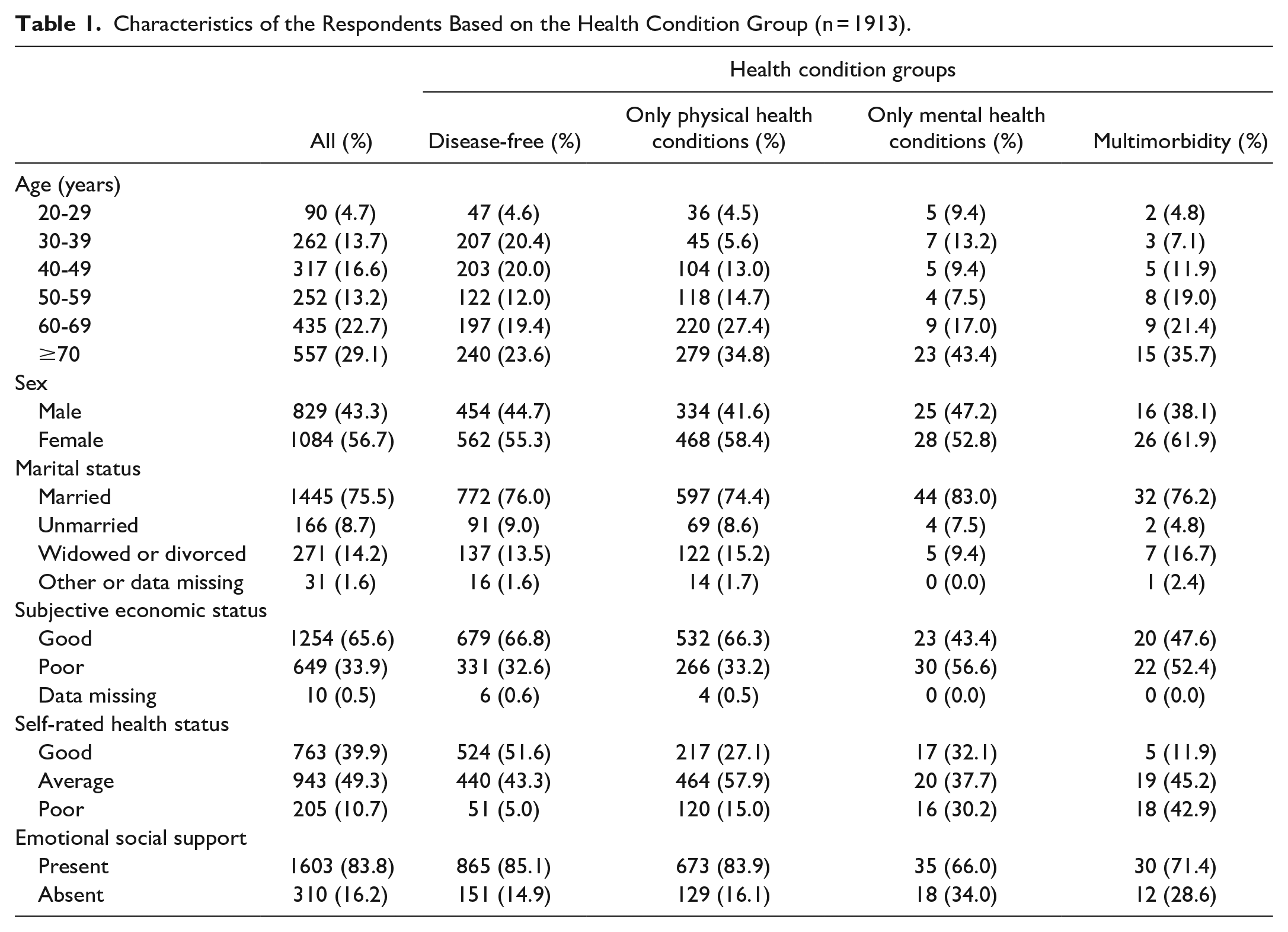
Table 2 shows the results of examining the association of suicidal ideation with different health condition groups. In the crude model (Model 1), suicidal ideation showed a significant positive association with the OMHC (OR = 6.88, 95% CI = 2.79-16.92, P < .05) and multimorbidity groups (OR = 9.04; 95% CI = 3.62-22.56, P < .05). These significant positive associations remained unchanged even after adjusting for age and sex (Model 2; OMHC group: OR = 7.06, 95% CI = 2.85-17.48, P < .05; multimorbidity group: OR = 9.56, 95% CI = 3.79-24.12, P < .05). These associations remained significant even after all confounders were adjusted for (Model 3; OMHC group: OR = 4.73, 95% CI = 1.79-12.54, P < .05; multimorbidity group: OR = 6.95, 95% CI = 2.58-18.68, P < .05).
Association of Suicidal Ideation with Different Health Condition Groups (n = 1913).

Abbreviations: CI, confidence interval; OR, odds ratio.
Model 1: crude model. Model 2: adjustments made for age and sex. Model 3: adjustments made for marital status, subjective economic status, and emotional social support in addition to the adjustment variables in Model 2.
Table 3 shows the results of the stratified analysis. After stratification, the ORs (95% CIs) for the multimorbidity group remained significantly higher compared with the disease-free group (reference) in both the presence (OR = 7.68, 95% CI = 1.90-31.07; P < .05) and absence of emotional social support (OR = 6.44, 95% CI = 1.61-25.79, P < .05). In contrast, the OR (95% CI) for the OMHC group decreased in the presence of emotional social support (OR = 1.94, 95% CI = 0.24-15.78, P < .05) but remained significantly higher in the absence of emotional social support (OR = 8.04, 95% CI = 2.21-29.29, P < .05).
Stratified Analysis Based on the Presence and Absence of Emotional Social Support.

Abbreviations: CI, confidence interval; OR, odds ratio.
Adjustment variables: age, sex, marital status, and subjective economic status.
Discussion
Our results revealed that the presence of OMHC and multimorbidity, but not OPHC, is associated with suicidal ideation. The OR for the multimorbidity group was higher than that for the OMHC group. Furthermore, emotional social support modified the OR for suicidal ideation in individuals with OMHC but not in individuals with multimorbidity.
The finding that the presence of OMHC and multimorbidity is associated with suicidal ideation is consistent with previous research.21,22 However, in previous studies, the point estimates for suicidal ideation did not differ between individuals with OMHC and those with multimorbidity. In this study, the OR for the multimorbidity group was higher than that for the OMHC group. One reason for this result could be that individuals were misclassified owing to self-reported data. Another reason could be that the health condition of individuals with multimorbidity may have been more severe and required continuous medical care, considering that there were a higher number of individuals who considered their health status poor among individuals with multimorbidity (42.9%) than among those with OMHC (30.2%). In this study, the severity of health conditions was not considered. Therefore, this aspect should be considered in future studies.
In this study, emotional social support reduced the OR of only the association between suicidal ideation and the presence of OMHC. This finding is consistent with that of previous research. 29 Emotional social support did not modify the association between suicidal ideation and the presence of multimorbidity in this study. Şengül et al 38 conducted a study targeting patients with cancer and found that as the cancer stage progresses, individuals feel less emotional social support, which increases the risk of suicidal ideation and suicide attempts. Considering the higher prevalence of poor perceived health among individuals with multimorbidity in this study, such individuals may have felt less emotional social support, and it may have resulted in no decrease in the OR for suicidal ideation. For these individuals, a different type of social support may help prevent suicidal ideation. One study found that emotional social support does not contribute to preventing complete suicide; only instrumental social support is a protective factor against it. 39 It has also been found that only instrumental social support moderates the association between high psychological stress and completed suicide; emotional social support does not have a significant effect. 27 Completed suicide occurs in more severe situations than suicidal ideation. Similar to individuals who have completed suicide, those with multimorbidity might require direct support, such as instrumental social support. Future research should examine how different types of social support impact the association of suicidal ideation with the presence of OPHC, OMHC, and multimorbidity.
This study is salient because it not only examines the association of suicidal ideation with the presence of OPHC, OMHC, and multimorbidity but also investigates the modifying role of emotional social support in these associations. However, this study has some limitations. First, it was cross-sectional and thus could not establish causality. However, it provides valuable insights for future longitudinal and interventional studies. Second, this study was conducted in a single rural area of Japan. Given the reported differences in suicide rates and backgrounds between urban and suburban areas,40,41 the generalizability of our results may be limited. Third, data on health conditions was self-reported, and there was no data available on the severity of the health conditions. This may have led to the misclassification of respondents. Fewer individuals reported poor subjective health in the OPHC group than in the OMHC and multimorbidity groups. Therefore, the OPHC group may have had a higher proportion of individuals with less severe health conditions. Additionally, there was no information available on the treatments for the respective physical and mental health conditions these participants were going through. This could be a confounding factor to the conclusion derived. Fourth, emotional social support was measured using only 1 item. This may reduce the validity of the measurement. For future research, validated scales will be used to ensure validity. Additionally, this study focused only on emotional social support and did not obtain data on instrumental or informational social support. Future research should obtain data on the different types of social support to examine their distinct impacts on the association of suicidal ideation with the presence of OPHC, OMHC, and multimorbidity. Fifth, this study asked about suicidal ideation only in the past 30 days. This makes it difficult to assess the long-term risk of suicidality in the rural population and identify the type of social support one requires based on one’s health condition.
Conclusion
Suicidal ideation is positively associated with the presence of OMHC and multimorbidity, but emotional social support modifies only the association between suicidal ideation and the presence of OMHC. For suicide prevention, it may be important to identify the type of social support one requires based on one’s health condition.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI Grant Numbers JP23K10383, JP24K13853.