
Abstract
Background:
Congenital cytomegalovirus (cCMV) affects 1 in every 200 United States infants, at present there are 9 states which mandate newborn cCMV screening. With more infants being diagnosed, more children will need continuing care from providers who are knowledgeable about cCMV.
Objectives:
To examine pediatric provider knowledge, practices, and beliefs around cCMV.
Methods:
Primary care and newborn hospitalist pediatricians (N = 103) from Michigan, who “regularly care for infants” were invited to participate in a survey about their cCMV-related knowledge, clinical practices, and beliefs.
Results:
Respondents had low knowledge of typical cCMV presentation and sequelae, with mixed knowledge of screening and testing standards. Most (68%) reported rarely/never screening for cCMV, though 71% strongly agreed/agreed that primary care providers should test for cCMV. Most (90%) strongly agreed/agreed that infants who fail/refer on their newborn hearing screen should be tested for cCMV, yet 81% expressed not being comfortable diagnosing and managing cCMV. Most (72%) felt that cCMV was not sufficiently covered in their medical training; almost all respondents endorsed interest in learning more.
Conclusions:
Primary care and newborn hospitalists in this study expressed mixed knowledge about, infrequent practice of and low comfort with screening and caring for children with cCMV. This may present a prime opportunity for education and clinician support by professional organizations.
Introduction
Congenital cytomegalovirus (cCMV) affects 1 in 200 infants in the United States and is associated with heightened risk of sensorineural hearing loss, cerebral palsy and intellectual disability.1,2 Due to its often subtle clinical presentation, roughly 95% of cases go undiagnosed at birth. 3 Early diagnosis, audiologic interventions, therapeutic supports and treatment with antiviral medication (for those who qualify) may be associated with improved developmental, hearing and language outcomes.4,5 In response, newborn cCMV screening programs have become more widespread at the state and health system level over the last decade.6,7 Such screening programs include hearing-targeted screening programs, in which only infants who fail (eg, refer from) on their newborn hearing screening are tested for cCMV,7,8 or universal screening programs which screen all infants for cCMV.9,10 With more infants being diagnosed at birth, more children will need continuing care from health care providers who are knowledgeable about the spectrum of treatments, supports and likely long-term outcomes associated with cCMV. Comprehensive guidelines for the diagnostic evaluation, ambulatory care, and anticipatory management of infants and children with cCMV have yet to be issued by the American Academy of Pediatrics (AAP) or the American Academy of Family Physicians (AAFP). While guidelines from the AAP are anticipated to be released in the upcoming years, pediatric health care providers’ knowledge, current practices, and beliefs about cCMV remain unknown. Therefore, our objectives in this study were to examine pediatric health care providers’ knowledge, practices, and beliefs around cCMV, to inform the creation and adoption of best practice guidelines and continuing education targets.
Methods
In brief, we invited primary care and hospitalist pediatricians (N = 103) currently practicing in Michigan to complete an online survey about their “practices and beliefs surrounding congenital cytomegalovirus.” As we sought to evaluate this knowledge in pediatricians who cared for well newborns regularly, subspecialists (eg, neonatologists, infectious disease clinicians) and trainees were excluded. We recruited participants virtually through online postings at a regional pediatric conference, a state-wide physician social media group, and by emails sent to listservs of state-wide and local healthcare systems. See Supplemental Materials for additional information about survey administration. Eligible participants: (1) possessed an MD or DO, (2) were a practicing pediatrician in Michigan, (3) regularly cared for infants in primary care or in the newborn nursery, and (4) were comfortable completing the questionnaire in English. Participants were compensated $20 for survey completion. The University of Michigan Institutional Review Board reviewed the study and approved the study as being exempt human subject research (HUM00181376). At the study institution the exempt human subjects research designation is given to studies that “generally pose ‘no more than minimal’. risk, involve simple, well-understood study design, and do not involve subjects likely to be vulnerable to coercion or undue influence. Exempt status does not lessen researchers’ ethical obligations to subjects as articulated in the Belmont Report, in disciplinary codes of professional conduct, and in (university) policies.” 11
Measures
A survey instrument was created based on previous work examining healthcare provider’s knowledge about cCMV (See Supplemental Materials).12,13 We separated survey items into 3 areas, cCMV: knowledge (8 items), practices (9 items), and beliefs (16 items). Congenital CMV Knowledge measured the general construct of provider’s knowledge around cCMV prevalence, presentation, diagnosis, acute treatment, and long-term management (α = .78). Items assessing CMV knowledge had multiple choice answers. To assess provider practices, participants reported how often they screened for CMV in a clinical scenario for the first 4 items, answering on a 5-point Likert scale ranging from 1 = Always to 5 = Never, with an additional option of selecting “I don’t know.” Participants also reported their agreement with statements about practices (3 items). Finally, to measure beliefs, participants reported their agreement with statements about CMV screening, diagnosis, comfort in diagnosis, prevention education, and medical education. Items of agreement were measured on a 5-point Likert scale ranging from 1 = Strongly agree to 5 = Strongly disagree, with an additional option of selecting “I don’t know.” Constructs in provider practices and beliefs were wide ranging, and not designed to measure single quantifiable variables (eg, “high vs low practices”) therefore internal consistency was not calculated. Please see Supplemental Materials for more details about survey design and administration using the Checklist for Reporting Results of Internet E-Surveys. 14
Participants reported their age, gender, race/ethnicity, years in practice, medical degree type, and medical practice characteristics.
Sample Size Calculation
According to the US Department of Labor, there are roughly 990 practicing general pediatricians (including ~250 trainees, and some subspecialists such as Developmental and Behavioral Pediatricians (~15) and Emergency Medicine Pediatricians (~72)) in Michigan. Based on these numbers, we estimate that there are roughly 660 practicing primary care and newborn hospitalist pediatricians in Michigan. A sample of 243 would provide a margin of error of 5% with a 95% confidence interval for the population proportion; a balance between margin of error and financial limitations and feasibility limitations was achieved at recruiting 103 participants (margin of error of ±8.3 with a 95% confidence level). As such, results are interpreted with caution as is common in pilot studies.
Analysis
We calculated descriptive statistics for all variables. An Overall cCMV Knowledge Score was created by summing the correct (1), incorrect (−1), and “I don’t know” (0) answers for each question in the knowledge section of the survey with a possible range of −20 to +20. For multiple-select multiple-choice questions, the total score was calculated based on the sum of correct, incorrect, and “I don’t know” responses. Due to low response numbers for some ordinal response questions, we merged some response categories (eg, Rarely and Never were merged into Rarely/Never). Bivariate analyses examined between participant responses by practice type. Correlations between participant responses and Overall cCMV Knowledge Score, years in practice, and number of children with cCMV participants had cared for were examined. Using a Bonferoni correction, statistical significance was set at <.01. 15
Results
Characteristics of the sample are provided in Table 1. Most respondents identified as being primary care providers (71%) versus hospitalists (29%). The average age of respondents was 42.3 years (median 39.0, SD 10.5, range 27-68), the majority of whom were female (79%). Most respondents were white (84%), and of non-Hispanic ethnicity (94%). Respondents had been practicing medicine on average 12.2 years (median 10.0, SD 10.0, range 1-39), and most were affiliated with a hospital/healthcare system (62%). There were no statistically significant differences in gender, race, number of years in practice, or number of children with cCMV cared for between primary care providers and hospitalists (See Supplemental Materials).
Participant Characteristics (N = 103).

Abbreviations: CMV, cytomegalovirus; DO, Doctor of Osteopathic Medicine; MD, Doctor of Medicine; SD, standard deviation.
Participant responses to cCMV knowledge questions are shown as a group and by practice type in Table 2. Less than a quarter (23%) of all respondents reported the correct prevalence of cCMV, and only 40% selected the correct timing window to test for cCMV in infancy. Most respondents correctly selected the appropriate diagnostic test (88%), pharmacologic treatment (77%), and the recommended follow-up for infants with cCMV (89%). Just over a quarter (26%) of respondents correctly answered that cCMV could present with no signs at birth. The mean Overall cCMV Knowledge Score was 10.0, (SD 4.1, range −2 to 19) out of a possible range of −20 to +20 points. There were no statistically significant differences between cCMV knowledge item responses based on provider practice type.
Participant Responses to Congenital CMV Knowledge Items (n = 103).

See Supplemental Materials for the survey instrument and answer key.
Only data for correct response options are presented, data regarding responses to incorrect response options (eg, hirsutism) are available from the authors upon request.
Possible range of correct answers = −20 to +20.
Possible range = −6 to +6.
Reported cCMV practices and beliefs for the entire sample are presented in Table 3. More than half of respondents (59%) reported never or rarely testing a newborn who failed their newborn hearing screening for cCMV. Most pediatricians (62%) reported often or sometimes testing for cCMV when an infant is born small for gestational age, and/or microcephalic and just under half (48%) reported always testing an infant with the combination of petechiae, hepatosplenomegaly, and jaundice for cCMV. Most respondents reported rarely or never screening for cCMV in their practice (68%), though most (70.9%) strongly agreed or agreed that primary care pediatricians should test for cCMV. Most (90%) strongly agreed or agreed that all infants who fail their newborn hearing screen should be tested for cCMV, and just over half (53%) disagreed or strongly disagreed that all infants should be tested for cCMV. Only 19% strongly agreed or agreed that they had good overall knowledge about the diagnosis, treatment, and follow up of children with cCMV. The majority strongly disagreed or disagreed that cCMV diagnosis and management was sufficiently covered in their medical education and training in primary care (72%) and in the newborn nursery (64%). Nearly all respondents strongly agreed or agreed that they would be open to learning more about cCMV testing (98%), management and long term follow up (99%) in primary care. There were no statistically significant differences in reported cCMV beliefs and practices by provider practice type (data provided in the supplemental materials).
Participant Reported Practices and Beliefs About Congenital Cytomegalovirus (% Participants Reporting, N = 103).
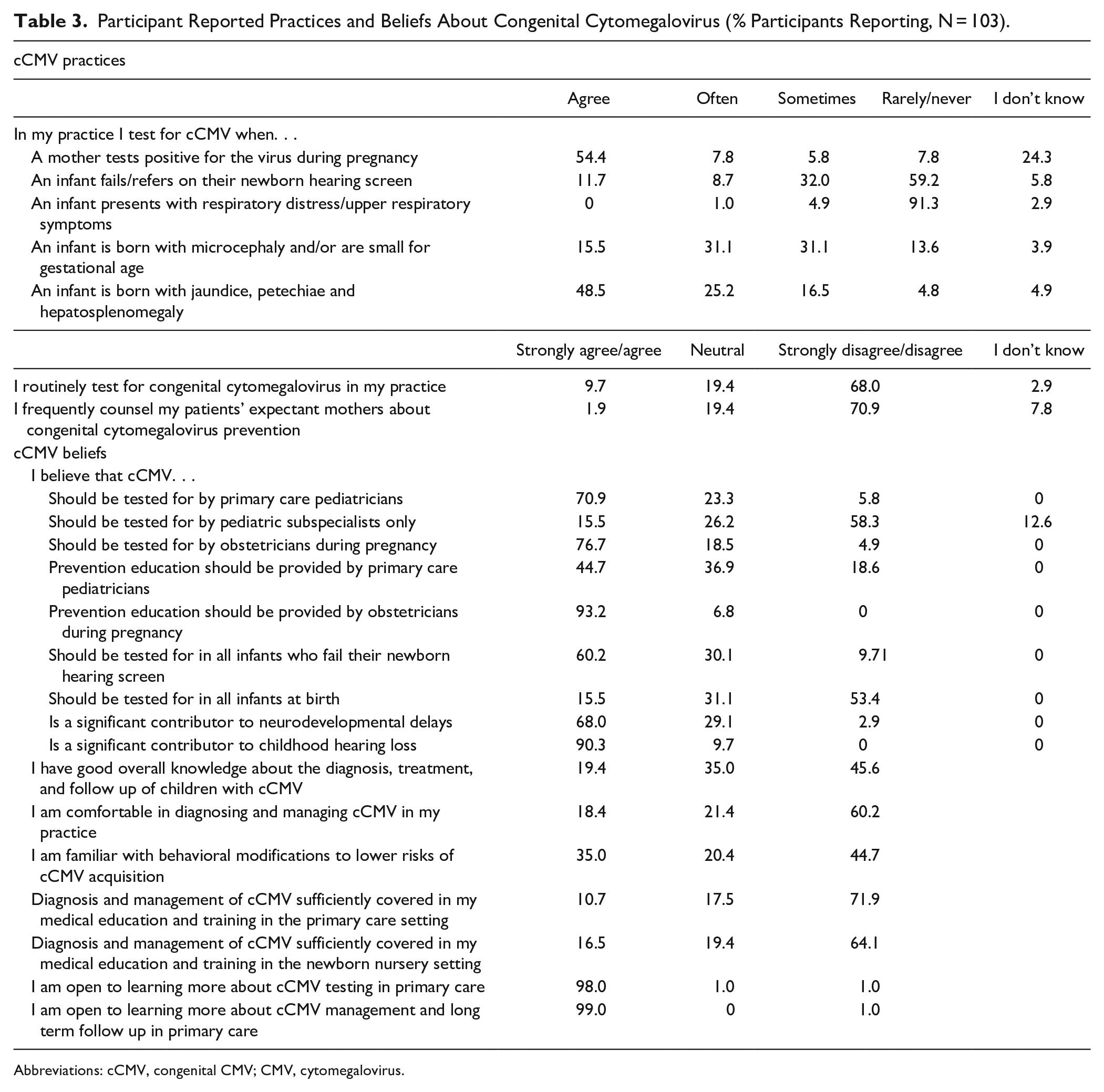
Abbreviations: cCMV, congenital CMV; CMV, cytomegalovirus.
Bivariate analyses revealed a positive correlation with moderate effect sizes between Overall CMV Knowledge score with being comfortable with and having self-perceived good overall knowledge about the diagnosis and treatment of cCMV (ρ = .34, P ≤ .001, and ρ = .36, P ≤ .001, respectively). Number of years in practice was positively correlated with agreement that cCMV should be tested for by subspecialists only (ρ = .27, P = .006, moderate effect size). Caring for more children with cCMV was correlated with less frequent counseling of expectant mothers about cCMV, feeling more comfortable with and knowledgeable about diagnosing and treating children with cCMV(ρ = .34, ρ = .37, and ρ = .43, all P’s ≤ .001, moderate to relatively strong effect sizes).
Discussion
This study identified knowledge, practices, and beliefs surrounding cCMV in a cohort of Michigan pediatricians. Overall, participants’ knowledge about the disease was stronger in some areas (eg, how to test for cCMV) and weaker in others (eg, the presentation and possible sequelae of cCMV). Most participants reported rarely or never testing infants who fail/refer on their newborn hearing screen for cCMV and that they did not routinely screen for cCMV in their practices. Most respondents believed that cCMV should be tested for by primary care providers, yet also reported that the diagnosis and management of cCMV was not sufficiently covered in their medical education and that they were not comfortable with doing so in their present practice. Almost all respondents endorsed an interest in learning more about cCMV testing and management in primary care. While studies of cCMV knowledge and practices of obstetric providers, family medicine providers in Iran, pediatric specialists, and therapists have been conducted, this study is the first to examine cCMV knowledge, practices, and beliefs among US pediatric primary care providers and newborn hospitalists.12,13,16 -20
Our findings regarding low knowledge of neonatal presentations of cCMV as well as lower levels of comfort in caring for infants with cCMV may point to opportunities for education and clarification from professional organizations. Most participants reported that the diagnosis and management were not sufficiently covered in their medical education. With more US states and health systems implementing cCMV newborn screening policies,8,21 -23 it is imperative that clinicians who care for these neonates have appropriate resources and guidance. We believe that individual pediatricians are not “at fault” for these knowledge gaps. Unlike some other countries,24 -27 US medical professional organizations such as the American Academy of Obstetrics and Gynecology and the AAP have not yet prioritized cCMV prevention, diagnosis, and management in practice guidelines. 28 Without the AAP emphasizing the importance of cCMV diagnosis and management, outside of the most severe presentations, 29 pediatricians will continue to experience gaps in their cCMV knowledge and practices which may result in missed opportunities to diagnose and treat cCMV. For example, three-quarters of participants were unaware that cCMV could present with “no signs” at birth, and 39% were unaware that asymptomatic infants were at elevated risk of sensorineural hearing loss. Our study found that almost all respondents were receptive to learning more about cCMV diagnosis and management in the ambulatory care setting. Continuing medical educational opportunities, and practice guidance from professional organizations may help increase provider cCMV awareness, and confidence in management. Future studies should examine whether such opportunities and guidance result in improved quality of care and ultimately child outcomes.
Participants in our study expressed a lack of enthusiasm for universal cCMV screening (routine screening of all infants) and preference for hearing-targeted cCMV screening (screening those who fail/refer on their newborn hearing screen only). We are left to infer why participants felt this way—it may be due to personal experiences, lack of knowledge, or other underlying concerns. The successful implementation of any newborn screening initiative is reliant on the investment and partnership of the clinicians caring for that infant in the newborn nursery and ultimately in the primary care setting. 30 Participants in our study welcomed more opportunities to learn more about cCMV—it is important that pediatricians not only understand the rationale behind a screening program, but also feel comfortable in and empowered to care for their patients and families affected by cCMV. A deeper understanding of pediatric healthcare provider’s insights about cCMV through qualitative interviews will help inform the design, implementation, and acceptance of cCMV screening programs in states and health systems. Congenital CMV screening programs should consider not only the importance of an early cCMV diagnosis, but also whether pediatric healthcare providers are sufficiently supported to order the necessary tests, referrals, and coordinate care in a timely manner.
Responses in our study did not differ between primary care and hospitalist pediatric providers, which may be due to the small sample size, or because cCMV awareness is equally low among pediatric specialists in this region. Future studies should investigate the possible differences in knowledge, practices, and beliefs through qualitative interviews—it is likely that pediatric providers caring for newborns in different settings would have varying views. For instance, a newborn hospitalist may perceive different barriers to newborn cCMV screening than a primary care provider, given the timing of screening after the birth. Or a primary care provider may have unique insights about the barriers and facilitators of care within the medical home than a hospitalist.
Participants in our study were limited to primary care and hospitalist pediatricians caring for newborns from a single state, as such our results may not be generalizable to subspecialists or providers of other specialties or other geographic areas. Due to feasibility, our study was underpowered to generalize results to all pediatricians in Michigan. Studies in larger national cohorts including family practitioners are needed to understand national trends in pediatric education about cCMV. Results from this study were based on participant self-report, which is subject to the social desirability bias.13,31
Conclusions
Pediatric healthcare providers in this study had low knowledge of cCMV presentation at birth and later possible sequelae, and mixed knowledge of screening and testing practices based on common possible signs of cCMV. Many respondents expressed not being comfortable with the diagnosis and management of cCMV in their practice, and that this was not sufficiently covered in their medical training. Almost all respondents endorsed being open to learn more about cCMV diagnosis and management, which represents a prime opportunity for education and support by professional organizations. Future work should investigate whether the publication of clinical guidelines for the diagnosis and management of cCMV result in improved healthcare provider knowledge, quality of care, and ultimately, child outcomes.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319221106880 – Supplemental material for Congenital Cytomegalovirus Knowledge, Practices, and Beliefs Among Primary Care Physicians and Newborn Hospitalists
Supplemental material, sj-docx-1-jpc-10.1177_21501319221106880 for Congenital Cytomegalovirus Knowledge, Practices, and Beliefs Among Primary Care Physicians and Newborn Hospitalists by Megan H. Pesch and Kathleen M. Muldoon in Journal of Primary Care & Community Health
Supplemental Material
sj-docx-2-jpc-10.1177_21501319221106880 – Supplemental material for Congenital Cytomegalovirus Knowledge, Practices, and Beliefs Among Primary Care Physicians and Newborn Hospitalists
Supplemental material, sj-docx-2-jpc-10.1177_21501319221106880 for Congenital Cytomegalovirus Knowledge, Practices, and Beliefs Among Primary Care Physicians and Newborn Hospitalists by Megan H. Pesch and Kathleen M. Muldoon in Journal of Primary Care & Community Health
Supplemental Material
sj-docx-3-jpc-10.1177_21501319221106880 – Supplemental material for Congenital Cytomegalovirus Knowledge, Practices, and Beliefs Among Primary Care Physicians and Newborn Hospitalists
Supplemental material, sj-docx-3-jpc-10.1177_21501319221106880 for Congenital Cytomegalovirus Knowledge, Practices, and Beliefs Among Primary Care Physicians and Newborn Hospitalists by Megan H. Pesch and Kathleen M. Muldoon in Journal of Primary Care & Community Health
Supplemental Material
sj-pdf-4-jpc-10.1177_21501319221106880 – Supplemental material for Congenital Cytomegalovirus Knowledge, Practices, and Beliefs Among Primary Care Physicians and Newborn Hospitalists
Supplemental material, sj-pdf-4-jpc-10.1177_21501319221106880 for Congenital Cytomegalovirus Knowledge, Practices, and Beliefs Among Primary Care Physicians and Newborn Hospitalists by Megan H. Pesch and Kathleen M. Muldoon in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The authors would like to thank Clare Lauer for her assistance proofreading, and Danielle Appugliese (Appugliese Advisors) for assistance with data analysis. Our data coding was informed by discussions with Seth Dobson (Artful Analytics, LLC) as part of collaboration on a separate report (Muldoon et al in review).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MP serves on the Executive Committee of the National CMV Foundation (unpaid), KM serves as the Chair of the Scientific Advisory Committee of the National CMV Foundation (unpaid). MP serves as an ad hoc consultant to DiaSorin Molecular and MedScape. These entities did not have any input into the conceptualization, data collection, data analysis of this study, or creation of this manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.