
Abstract
Introduction:
Venous thromboembolism (VTE) is a multifactorial condition and one of the leading causes of mortality and disability. The present study explores the factors associated with hospitalization duration among different types of venous thromboembolism diagnoses, such as deep vein thrombosis (DVT), pulmonary embolism (PE), and other forms of thrombosis.
Methods:
The data included participants with VTE admitted to 13 hospitals within pan-India from June 2022 to December 2023 to the i-RegVed registry, where socio-demographic data, clinical history, and various factors associated with hospital length of stay (LOS) were included for analyses. Multilinear regression was performed to explore the factors associated with hospital LOS among VTE conditions such as DVT, PE, forms of thrombosis other than PE and DVT, and all VTE diagnoses.
Results:
A total of 633 participants were included in the study, with 55% being males, and 28.9% being homemakers. Longer hospital LOS was significantly associated with age (β = −.09, P < .05), sex (β = 3.21, P < .05), and non-communicable diseases (β = 3.51, P < .05) among participants with DVT and among participants with at least one of the VTE diagnoses, age (β = −.12, P < .001) and anticoagulant use (β = −2.49, P < .05) was significantly associated.
Conclusion:
The findings provide insights into the factors influencing hospital outcomes among participants with different types of VTE, highlighting the importance of age and comorbidities in predicting the hospital LOS.
Introduction
Venous thromboembolism (VTE) is a multifactorial condition that primarily includes deep vein thrombosis (DVT) and pulmonary embolism (PE). Still, thrombosis can affect other veins, including upper extremities, cerebral venous sinuses, and splanchnic veins, and is estimated to be the third most frequent cardiovascular mortality in Western countries. 1 In Asian countries, the disease burden of VTE has always been considered lower. 2 However, the incidence rates of VTE are increasing,3 -5 making it a major health concern in many Asian countries, including India. 6
The earliest known case of VTE was reported in the right leg of a 20-year-old man in the 13th century. 7 Several hypotheses to understand the mechanism of VTE have been postulated,8,9 of which Virchow’s triad is often discussed and provides the basis for thrombosis-related research today. Virchow’s triad describes hypercoagulability, stasis, and endothelial injury as factors contributing to the development of venous thrombosis. 10 However, it does not fully explain the increased risk of recurrent VTE and the need for an extended duration of anticoagulant use, and the underlying mechanism leading to the reoccurrence remains unclear. 11
The clinical presentation of DVT varies with the location and extent of occlusion of the thrombus. 12 Common symptoms include swelling and pain in the lower extremities, blue-red or cyanotic discoloration, tenderness, and thermoregulatory changes such as increased temperature.13,14 DVT also varies between provoked and unprovoked. As such, provoked DVTs result from risk factors such as surgery and injury, however unprovoked DVT occurs without any apparent risk factors. 15 On the other hand, PE is associated with dyspnea, chest pain, cough, hemoptysis, and hemodynamic instability in the form of hypotension and hypoxia.14,16 Although the symptoms are common in most VTE patients, all do not experience these symptoms, making it difficult for earlier VTE diagnoses.
The risk factors of VTE include age, obesity, immobility, previous history of VTE, cancer, major trauma, autoimmune diseases, chemotherapy, hormone replacement therapy, postpartum period, long-haul travel, major surgery, blood transfusions, smoking, diabetes, genetics, and medications such as antipsychotics, antidepressants, diuretics, or analgestics.16 -28 Studies have also noted that after the initial occurrence of VTE among unprovoked patients, they remain at a higher risk of developing recurrent thrombosis.29,30 Notably, there is an increased risk of medical complications and functional decline with longer hospital lengths of stay (LOS), which in turn, may increase the risk of VTE. 31 For instance, a population-based study in Norway on 530 cancer-free VTE patients indicated that hospitalization was a major trigger associated with a 9-fold higher risk of VTE, which was mainly dependent on the hospital LOS but not the frequency of hospital admissions. 32
In response to the growing incidences of hospital-acquired VTE as a preventable healthcare-associated complication, healthcare organizations have initiated targeted interventions and quality improvement initiatives. For example, the American Heart Association called to action in 2017 to reduce hospital-acquired VTE by 20% by the year 2030. 33 The National Institute for Health and Care Excellence (NICE) also published guidance for reducing the risk of hospital-acquired VTE. 34 The guideline includes recommendations such as risk assessment, giving information and planning for discharge, and interventions for different conditions (eg, renal impairment, cancer, major trauma, etc.) Despite these initiatives, data on the hospital LOS among VTE patients are limited, 35 causing a significant gap in understanding the factors influencing hospitalization among VTE patients in India. Moreover, the differences in hospital duration among other types of VTE such as Budd-Chiari are unavailable.
Given the complications of VTE associated with hospitalization,36,37 there is a need for further research to elucidate the impact of hospitalization duration on the types of VTE. By highlighting factors that might prolong hospitalization among participants with different VTE types, healthcare providers can identify high-risk patients and help implement targeted interventions to mitigate adverse outcomes. Moreover, an improved understanding of the factors influencing hospital duration among different VTE types could help patients and their care providers reduce their elevated risks. The present study seeks to investigate the relationship between hospitalization duration and VTE types such as PE, DVT, PE and DVT, other single forms of thrombosis (eg, Budd-Chiari), and other multiple forms of thrombosis, focusing on identifying the determinants of hospital LOS.
Methods
Study Setting
This prospective hospital-based study was conducted across India from June 2022 to December 2023. Participating sites included 13 hospitals, where VTE patient data was collected with the help of a structured questionnaire, and data collected was uploaded to the National VTE Registry, the i-RegVeD registry.38,39
Study Data Variables
Inclusion Criteria
All participants who experienced one or more events of objectively confirmed VTE, including other sites of venous thrombosis, through X-rays, CT scans, MRI, and/or ultrasound, were included in this study. Moreover, we included only those participants whose outcome was recovered and were discharged to observe the factors associated with the hospital LOS in our population. Thus, out of 1006 participants, 633 were included in this study (Figure 1).

Flow chart showing participant selection.
Exclusion Criteria
Participants were excluded if they were diagnosed with arterial thrombosis and those with either missing hospital LOS or without VTE outcomes from diagnostic imaging were excluded. Moreover, we excluded participants who were either referred from a different hospital at the time of admission, referred from the hospital to another facility, left against medical advice, or died.
Data Collection
Data on age, sex, occupation, locality, family history of VTE, duration of hospital stays, medical procedures, and chronic diseases were included. Hospital LOS was calculated based on the date of admission to the hospital and the date of discharge from the hospital. The VTE status objectively confirmed through diagnostic techniques was divided into (a) DVT, (b) PE, (c) DVT with PE, (d) forms of thrombosis other than PE and DVT (single), and (e) other multiple VTE diagnoses. Other thrombosis events included cerebral sinus venous thrombosis, jugular venous thrombosis, portal venous thrombosis, superficial venous thrombosis, Budd Chiari syndrome, and extrahepatic portal vein obstruction.
Statistical Analysis
Participant data was downloaded from the registry site 38 as an Excel file for use in RStudio. 40 Continuous variables were presented as mean, standard deviation, and categorical variables as frequencies and percentages. LOS was categorized based on age and gender. Based on earlier studies, age was classified as >13, 13 to 17, 18 to 30, 31 to 50, and >50. 41 A line graph and student t-test were used to find the mean difference between gender and hospital LOS. Age, sex, previous history of VTE, communicable diseases, non-communicable diseases, anticoagulant use, injury, and surgeries were included as covariates based on a priori studies.16 -28 Multilinear regression was performed to understand whether the hospital LOS was associated with different VTE conditions such as DVT, PE, forms of thrombosis other than PE and DVT, and all VTE diagnoses. The regression model did not include other VTE diagnoses and PE + DVT due to lack of power. All independent variables, such as age, sex, previous history of VTE, communicable diseases, non-communicable diseases, anticoagulant use, injury, and surgeries, were mutually adjusted. A 2-sided P-value of <.05 was considered statistically significant.
Results
Baseline Characteristics
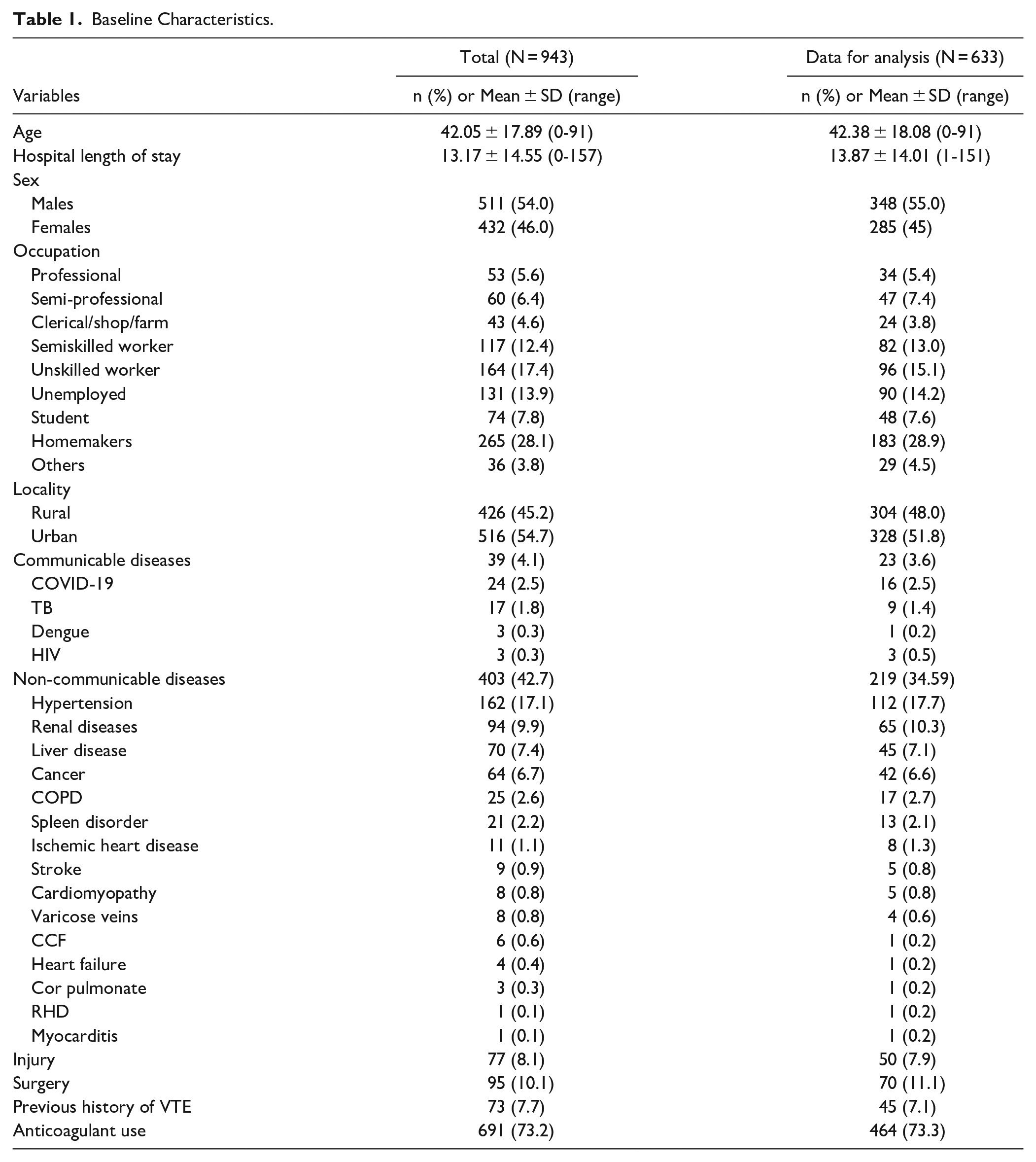
The mean age of the participants from the total registry data and subgroup included in this study was about 42 years. The median age of the selected group was ~41 years. Out of 633 participants diagnosed with VTE, 43.1% were older than 50 years, 37.1% were 31 to 50 years old, 22.2% were 18 to 30 years old, 5.3% were less than 13 years of age, and 1.1% were aged 13 to 17 years old. The mean hospital LOS was also similar in both total registry data and a subgroup of participants (~14 days) ranging from 1 to 151 days. Out of the subset of participants included in this study (n = 633), 55% were males, 45% were females, most of the participants were homemakers (28.9%), and about 51% were from the urban locality. Regarding comorbidity, 3.6%, and 34.5% responded to having at least one of the communicable and non-communicable diseases, respectively. As such, 2.5% responded to having COVID-19, 1.4% had TB, 0.5% had HIV, and 0.2% had dengue fever. For non-communicable diseases, 17.7% responded to having hypertension, 10.3% had renal diseases, 7.1% had liver disease, 6.6% had cancer, 2.1% had spleen disorder, 0.8% each had stroke and cardiomyopathy, 0.6% had varicose veins, and 0.2% each had congestive cardiac failure, heart failure, cor pulmonated, rheumatic heart disease, and myocarditis. In terms of other factors that might be associated with hospital LOS, 73.3% were administered anticoagulants during hospitalization, 7.9% had an injury, and 11.1% of the participants responded to having had major surgery (Table 1).
Baseline Characteristics.
Hospital LOS
Mean duration of hospital LOS among participants with different VTE diagnoses indicated that males with other forms of thrombosis other than PE and DVT had a higher hospital LOS at about 17 days. In contrast, among females, those with PE diagnosis had a longer hospital stay with an average of ~17 days. A significant difference (P < .01) between males and females was observed among participants with DVT but not others (Figure 2).

Mean length of hospital stay between different VTE status and gender.
The duration of hospital LOS among different age groups indicated that ages less than 13 years had the longest mean LOS of 22 days ranging from 1 to 64 days, followed by 13 to 17 years (18 days ranging from 3 to 68 days), 18 to 30 years (~16 days ranging from 1 to 85 days), 31 to 50 years (~14 days ranging from 1 to 151 days), and older than 50 years (~12 days ranging from 1 to 62 days) (Table 2). We did not analyze the association between age categories and hospital LOS due to a lack of power with ages less than 18.
Frequency of Ages and Mean Hospital Length Among Different Age Groups (N = 633).

Multilinear regression was used to analyze hospital LOS (Table 3). After controlling for independent variables such as previous history of VTE, communicable diseases, non-communicable diseases, anticoagulant use, injury, and surgery, the model indicated that among participants who were diagnosed with DVT, age (β = −.09, P < .05) was negatively associated with hospital LOS. In addition, sex (β = 3.21, P < .05) and non-communicable disease (β = 3.51, P < .05) were significantly associated with hospital LOS among DVT participants. Interestingly, participants with longer LOS and with at least one of the VTE diagnoses were significantly associated with age (β = −.12, P < .001) and anticoagulant use (β = −2.49, P < .05). We also included the most common non-communicable disease (ie, hypertension) in a separate model controlling for all the independent variables. We found that hypertension (β = 4.16, P < .05) was independently associated with hospital LOS among DVT cases.
Multilinear Regression of LOS Among VTE Diagnosis.

Abbreviations: DVT, deep vein thrombosis; LOS, length of hospital stay; PE, pulmonary embolism; VTE, venous thromboembolism.
Reference male; Bold values indicate significant values at p<0.05; All variables are mutually adjusted.
Discussion
It is important to highlight hospital LOS among VTE as multiple studies indicate that patients with longer hospital LOS have an increased risk of medical complications and functional decline.31,32 In the present study, after controlling for hospital characteristics, among DVT participants, younger age was independently and significantly associated with longer hospital stays. In addition, female participants and those who responded to having at least one non-communicable disease were significantly and positively associated with longer hospital LOS. Anticoagulant use was independently associated with prolonged hospital LOS among overall VTE diagnoses. Other VTE diagnoses such as PE and forms of thrombosis other than PE and DVT, were not associated with hospital LOS.
Our study indicated that the mean age of the population was approximately 42 years, with the median age being 41 years, and the mean hospital LOS was about 14 days. Interestingly, the mean age was lower than in most studies focused on the adult population, which typically has mean ages over 60 years.35,42 -45 Contrary to studies that indicate an increase in the risk of VTE with age,46 -48 the present study found a different age distribution with VTE commonly diagnosed among younger age groups, particularly ages 19 to 38. This pattern aligns with studies on trauma patients in Houston (USA), which indicated that the median age of the study population was 34 years, and the greatest risk of VTE and highest likelihood of hypercoagulable maximal amplitude was among adults 31 to 50 years (P = .009 and P < .001, respectively). 41 Regarding gender, a balanced distribution was observed with 55% males and 45% females, consistent with existing literature.31,35,42,43 In terms of comorbidities, hypertension was the most reported comorbidity, followed by cancer, liver disease, renal disease, and chronic respiratory disease. This trend was consistent with findings from other studies. For instance, in a study from the Alberta-Venous Thromboembolism (AB-VTE) database, hypertension (admitted: 32.5% vs non-admitted: 14.8%; P < .001) was the most common comorbidity among venous thromboembolism patients, followed by malignancy (24.7% vs and 13.4%; P < .001) and chronic obstructive pulmonary disease (19.1% vs 8.3%; P < .001). 35 Other studies from the ESPHERIA registry and Jordan also indicate a similar trend.42,44 This finding highlights the complex clinical profile of VTE patients, characterized by a diverse range of underlying health conditions.
In exploring the factors associated with hospital LOS, gender and age differences were evident. As such, a significantly longer duration of hospital stay was observed among females with DVT and among DVT participants who were less than 18 years old. Interestingly, the youngest age group in our population (0-18) exhibited the longest mean hospital stay across different VTE diagnoses such as DVT, PE, forms of thrombosis other than PE or DVT, and overall VTE diagnosis. Findings from the National Inpatient Sample in the US indicated that among adult VTE patients when stratified by type of VTE event, women with lower extremity DVT and PE had a significantly longer hospital LOS (mean ratio 1.04, P < .001) in the unadjusted model however when the model was adjusted for age, race, insurance status, hospital division, and medical comorbidities, the findings was no longer significant. 49
Multilinear regression analysis further elucidated the factors influencing hospital LOS among participants with VTE. Younger age was independently associated with longer hospital LOS among participants with VTE diagnoses, particularly among participants with DVT. This finding is interesting as most studies indicate a reverse trend with longer hospital LOS among older patients.27,50,51 Interestingly, studies from the RIETE registry database observed that the hospital LOS was slightly lower in elderly patients despite their comorbidities and poorer prognosis. However, the age group included in the study was ≥70 years and <70 years, which is a wide age range. 52 Many factors might influence longer hospital stays among younger patients such as underlying medical conditions, difficulty or delays in diagnosis, treatment challenges, and access to care. 53 Moreover, there has been less research focused on pediatric VTE compared to adult VTE as it is less common in pediatric patients leading to a lack of evidence-based guidelines for management in this population. The management of VTE in pediatric patients also differs in terms of weight-based dosing of anticoagulants and the need for careful monitoring may lengthen the hospital stay.54,55 Future studies, including follow-up data, would be important to find the association between longer hospital LOS and younger age.
The presence of non-communicable disease was also positively associated with hospital LOS among participants with DVT, which is in line with other studies. 42 For instance, a study from the United States reported hypertension (r = .27, P = .037) to be associated with longer hospital LOS among VTE patients. 56 Our study also reiterated these findings, as hypertension was found to be significantly and positively associated with hospital LOS. The association between hypertension and hospital LOS among participants with DVT could be partially explained by the complex interplay between renin-angiotensin and kallikrein-kinin systems interacting at several levels to modulate coagulation, fibrinolysis, and vasodilatation influencing the occurrence of thrombotic complications. 57
Our study has several limitations, such as the presence of confounding factors that could affect the external validity and the inability to stratify the age group to assess the association between different VTE diagnoses with hospital LOS due to the lack of power. Causation could not be established here as this was a cross-sectional study. Despite these limitations, our findings are of interest. It is one of the first real-time ongoing VTE national registries in India that collects hospital-based data on VTE patients, including socio-demographic, diagnostic, treatment and management, and participants’ outcomes. Moreover, our study included other forms of VTE including cerebral sinus venous thrombosis, jugular venous thrombosis, portal venous thrombosis, superficial venous thrombosis, Budd Chiari syndrome, and extrahepatic portal vein obstruction which are important VTE diagnosis but often not presented in studies. The registry also includes follow-up studies, which are not included in our study due to limited data but would be an important addition to future studies.
Conclusion
The findings provide insights into the factors influencing hospital LOS among participants with different types of VTE, highlighting the importance of age and comorbidities in predicting the hospital LOS. In our study, most of the VTE cases were males. However, the gender distribution was not very different; it was most common among homemakers, those older than 50 years, and those who lived in urban areas. The study demonstrated that the mean hospital LOS was about 14 days. The most common comorbidity was hypertension, which has been associated with longer hospital LOS in multiple studies. More interestingly, among DVT cases, longer hospital LOS was associated with younger participants, being female, and those with non-communicable diseases. Future studies with follow-up data on the younger population would be beneficial in ascertaining whether there is a causal relationship between these identified factors. Moreover, additional studies about factors associated with longer hospital stays among younger patients with VTE can help come up with age appropriate health education policies and guidelines.
Footnotes
Acknowledgements
The authors would like to thank all the respondents for participating in this study, and the Indian Council of Medical Research, New Delhi for providing the necessary financial assistance.
Ethics
Written informed consent was obtained from all participants. The study protocol was approved by the Institutional Ethics Committee (IEC), Indian Council of Medical Research - Central Ethics Committee on Human Research (File No. NCDIR/BEU/ICMR-CECHR/75/2020). Each participating site obtained ethical approval from their respective IECs.
Contributors
PR, HT, and SA conceived and designed the idea. HT and SA overall supervision, resource acquisition, project administration, review, editing, and proofreading of the manuscript. i-RegVed Team data collection and reviewing the manuscript. PR was involved in writing the original draft of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Indian Council of Medical Research, New Delhi (Grant No. i-RegVed/Site10/BMS-2022).