
Abstract
Hospital at Home (HaH) programs continue to proliferate in the United States. There are few evaluations of recently started HaH programs. We evaluated a recently started HaH program by conducting a retrospective cohort study comparing outcomes of those admitted to HaH versus those who stayed in the brick-and-mortar hospital. All participants were patients of a large southeastern health system who were invited to participate in HaH. We used electronic health record data for the evaluation, and propensity score matching to minimize effects from the non-random assignment to group. HaH is an attempt to replicate hospital care in the patient’s home. Patients are monitored remotely. They receive in-person visits by nurses, paramedics, and advanced practice providers under the supervision of a hospital medicine attending. Attending physicians conducted virtual visits daily. The primary outcome was hospital readmission at 30 days. We also evaluated mortality, length of stay, and falls. Six hundred and seventy-one patients were invited to HaH and had complete data. Median age was 76 years (IQR: 69-84 years). Fifty-two percent participated in HaH. Length of stay was similar for HaH versus non-HaH (median 5.0 vs 4.0 days, p = .067). Patients in HaH were readmitted within 30 days more frequently than non-HaH (11.9% vs 7.78%, propensity-score adjusted HR 1.78, 95% CI 1.09-2.91). Mortality at 90 days was similar for HaH versus non-HaH (10.6% vs 10.1%, propensity score adjusted HR 1.42 [95% CI, 0.68-2.97]). HaH has similar outcomes as brick-and-mortar, although this new HaH program had a higher risk of readmission.
Introduction
Disadvantages to inpatient hospitalization include expense, treatment delays, capacity constraints, and hazards to patients including sleep deprivation, functional declines, and hospital-acquired infections.1-3 Hospital-at-home (HaH) programs may offer more convenient, cost-efficient, and safer care. HaH programs have existed in the U.S. for over 25 years and generally demonstrated equivalent or better health outcomes for patients, but longer lengths of stay.4-6 Comparisons to traditional inpatient services suggest that HaH may produce greater patient satisfaction, 7 fewer readmissions, 8 lower cost, 9 and lower mortality. 10 Early studies focused on single illnesses (e.g., stroke, heart failure), and subsequent studies have included patients with multiple chronic illnesses. 11
HaH programs proliferated during the SARS-CoV2 public health emergency with payment mechanisms from the Centers for Medicare and Medicaid Services (CMS) and private payers.12,13 Continued hospital capacity constraints after the public health emergency contribute to long emergency department (ED) wait times. 14 Longer ED boarding times may contribute to worse patient outcomes including mortality, longer hospital lengths of stay, treatment delays, and elopement.9,15-17 HaH programs may help decompress an over-crowded health system.
As new programs are started and established programs develop more experience, indications for and the capability of HaHs continue to evolve. With evolution there is opportunity to see changes in the effectiveness and safety of these programs and continued evaluation of their outcomes can help to shape policies about their scope. Few studies have evaluated recently launched HaH programs that started during the pandemic.18-20 With this study, we conducted a pragmatic evaluation of a new HaH program to understand the types of patients enrolling and to estimate the effects on 30-day readmission and 90-day all-cause mortality.
Methods
Design
We conducted a retrospective cohort study comparing outcomes of patients who were treated with HaH with those who did not receive HaH. Since this was not a randomized allocation, we carefully created a control group and used statistical methods to further improve the comparability of the control group with the intervention group. Specifically, the process for enrolling patients into the HaH program starts with evaluation of numerous patients who enter the emergency department and/or hospital and meet criteria for inpatient hospitalization. After identifying appropriate candidates by reviewing the chart and discussing the HaH option with the treating physician, if patients were determined to be good candidates for HaH, they were invited to participate. Many patients decide not to participate in the program for various reasons (discomfort in transitioning to the home setting, inadequate caregiver support, unsafe housing, concern for caregiver burden as a few). 21 It is those who declined to participate after they were deemed eligible for the service that comprise our control group.
Study Sample
We studied patients invited to participate in a HAH program during an emergency room or hospital admission between April and December 29, 2022 at 4 campuses of a southeastern U.S. medical system. HaH administrators and primary treating teams assessed eligibility by reviewing patients’ home addresses, payors, diagnoses, clinical stability, social stability, and treatment requirements. Eligible patients could be uninsured or covered by Medicare Part A, select Medicare Advantage plans, or the health system’s self-insurance plan. A HaH physician determined potential participants to have adequate clinical stability if there was low perceived risk for rapid decompensation, no requirement for continuous cardiac monitoring, and no need for the continuous presence of medical personnel. Required care was limited to what could be provided through intermittent nurse or paramedic visits. Exclusion criteria included the need for continuous infusion, hemodialysis, chemotherapy, or intravenous opiates. If a patient expressed interest in HaH participation, program staff administered a screening questionnaire to further assess the appropriateness of the patient, patient’s caregiver, and home location and environment for participation. Patients passed both clinical and social screening to be eligible for HaH. Study participants consisted of those who were considered eligible for HaH on initial review and received an invitation to participate.
HaH Overview
Patients could enroll in hospital at home while in the ED or after admission to a hospital bed. After enrollment, a dedicated EMS/paramedic team transported participants from the ED or hospital ward to their home, where staff set up medical supplies and an audiovisual monitoring system. A mission control team at the medical center monitored patients. HaH nurses, physicians, and advanced practice providers (APP) were continuously available to remotely assess patients as well as respond to concerns and issues. A hospitalist supervised treatment planning and conducted daily virtual visits with participants. At minimum, an APP conducted in-home assessments on the first and third days after HaH admission. Staff members could dispense and administer oral and intravenous medications, conduct point-of-care testing and phlebotomy, perform limited diagnostic studies (e.g., X-rays, ECGs, ultrasounds), and provide meals. Enrolled patients could receive ancillary services, such as physical or occupational therapy, in person. Paramedics transported patients back to the hospital for additional studies or stabilization as indicated.
Classifying Hospital at Home Status
We classified HaH participants as patients who met all HaH admission eligibility criteria and spent at least a portion of their index admission at home. We classified non-HaH participants as those who declined HaH participation or met eligibility and consented but could not participate due to logistical barriers (e.g., lack of staff availability, unreliable cell phone coverage).
Primary Study Outcomes
Analysts abstracted EHR data regarding the dates of emergency room and hospital admissions within the hospital system within 30 days of discharge and 90-day all-cause mortality. A research repository system integrated with participating hospitals EHR systems abstracted data from state vital statistics records to determine patients’ survival status up to August 2023.
Other Outcomes
Length of stay was calculated starting from the time of admission regardless of whether the admission started at brick and mortar or at the patient’s home. Data on the occurrence of falls were abstracted from standardized EHR forms completed by nurses and other providers.
Potentially Confounding Variables
We examined sociodemographic and clinical characteristics as potential confounding variables. Analysts abstracted EHR data on sex, age, race, ethnicity, and health insurance coverage. We examined MS-DRG V39 (FY2022) codes for primary admitting diagnosis and consolidated these diagnoses according to pathophysiology and organ system. We examined the Severity of Illness Index rating (i.e., minor, moderate, major, or extreme) assigned to patients at discharge based on review of medical records using a standard instrument. 22 The analysts abstracted diagnostic codes for 30 conditions present before or on admission to calculate the Elixhauser Comorbidity scores. 23
IRB Statement
This study was reviewed and approved by the University of North Carolina Institutional Review Board and determined to be of no more than minimal risk (#22-1495).
Statistical Analyses
We compared sociodemographic and clinical characteristics of HaH enrollees and non-enrollees using Wilcoxon rank-sum and Kruskal-Wallis tests for continuous variables due to the skewedness of distributions, and Pearson’s chi-squared tests for categorical variables. We used the same methods to compare events during the index admission including length of stay, occurrence of falls, mortality during index admission, discharge to skilled/assisted facilities, and discharge to hospice. We compared the percentage of patients experiencing an ED or hospital admission within 30 days of discharge, as well as 90-day all-cause mortality. We constructed Kaplan-Meier curves comparing 30-day survival free of hospital or ED admission and 90-day survival free of all-cause mortality using the log-rank test to compare HaH and non-HaH participants. To assess the relationship between HaH enrollment and rates of 30-day hospital admission, combined ED and hospital admission, and 90-day all-cause mortality we constructed univariate Cox proportional hazards models. We created an additional set of models adjusting for pre-specified demographic characteristics, and another set of models adding illness severity and Elixhauser scores. To better control for confounding due to the non-randomized nature of this study, we also constructed models using propensity score matching. 24 We calculated propensity scores using logistic regression to calculate the probability that a patient would be enrolled in the HaH according to age, race, sex, insurance status, illness severity, Elixhauser score, and comorbid conditions with prevalence greater than 5%. 25 We used one-to-many matching based on approximate propensity score. Due to a small number of outcomes, we did not perform regression analyses to assess the relationship between HaH enrollment and falls.
Results
Among the 701 initially identified patients, we excluded those with missing clinical outcomes data (n = 30), resulting in an analytic sample of 671 (95.7%). The sample median age was 76 years (IQR: 69-84 years), 55.5% were classified as female, 76.5% identified as white, and 7.9% identified as Hispanic or Latino (Table 1). They had numerous admitting diagnoses, but the top 3 were respiratory infection, sepsis, and urinary issues (Table 1).
Baseline Characteristics of Participants and Non-Participants of a Hospital at Home Program.
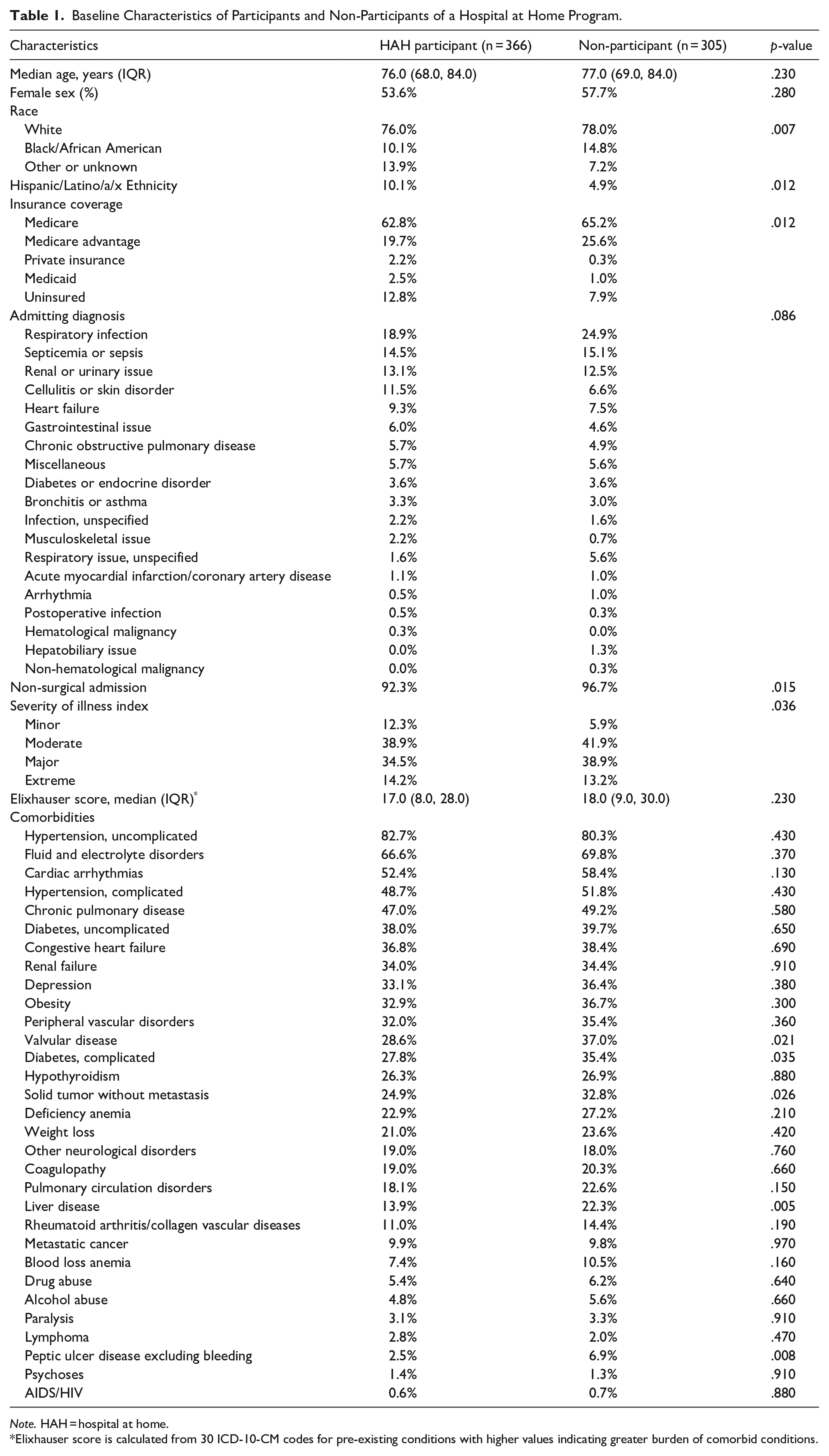
Note. HAH = hospital at home.
Elixhauser score is calculated from 30 ICD-10-CM codes for pre-existing conditions with higher values indicating greater burden of comorbid conditions.
Overall, 52.2% of eligible and invited patients participated in the HaH program. Compared with those who did not participate, those who participated in the HaH program were less likely to be Black and more likely to be Hispanic/Latino. They were more likely to have a surgical problem, but all other admitting diagnoses were similar. HaH participants were less likely to have comorbid diabetes, liver disease, solid tumor, and peptic ulcer disease. Overall, patients who chose HaH had similar comorbidity burden as measured by the Elixhauser score (HaH = 17 and non-HaH = 18, p = .23).
Table 2 shows that the length of stay was similar for HaH versus non-HaH (median 5.0 vs 4.0 days, p = .067). Overall, patients in HaH were readmitted within 30 days more frequently than non-HaH. Figure 1 shows unadjusted Kaplan-Meier Curves for hospital admission, and Table 3 shows both unadjusted and adjusted results (11.9% vs 7.78%, propensity-score adjusted HR 1.78, 95% CI: 1.09-2.91). For the combined outcome of readmission or ED visit, Figure 2 shows unadjusted Kaplan-Meier Curves and Table 3 shows the unadjusted and adjusted results (17.2% vs 14.8%, propensity score adjusted HR 1.52 95% CI: 1.03-2.25). Sensitivity analyses using traditional multivariable regression showed similar HR although they were not statistically significant. Mortality at 90 days was similar for HaH versus non-HaH (10.6% vs 10.1%, propensity score adjusted HR 1.42, 95% CI: 0.68-2.97; Table 3).
Clinical Outcomes of Hospital at Home Participants and Non-Participants.
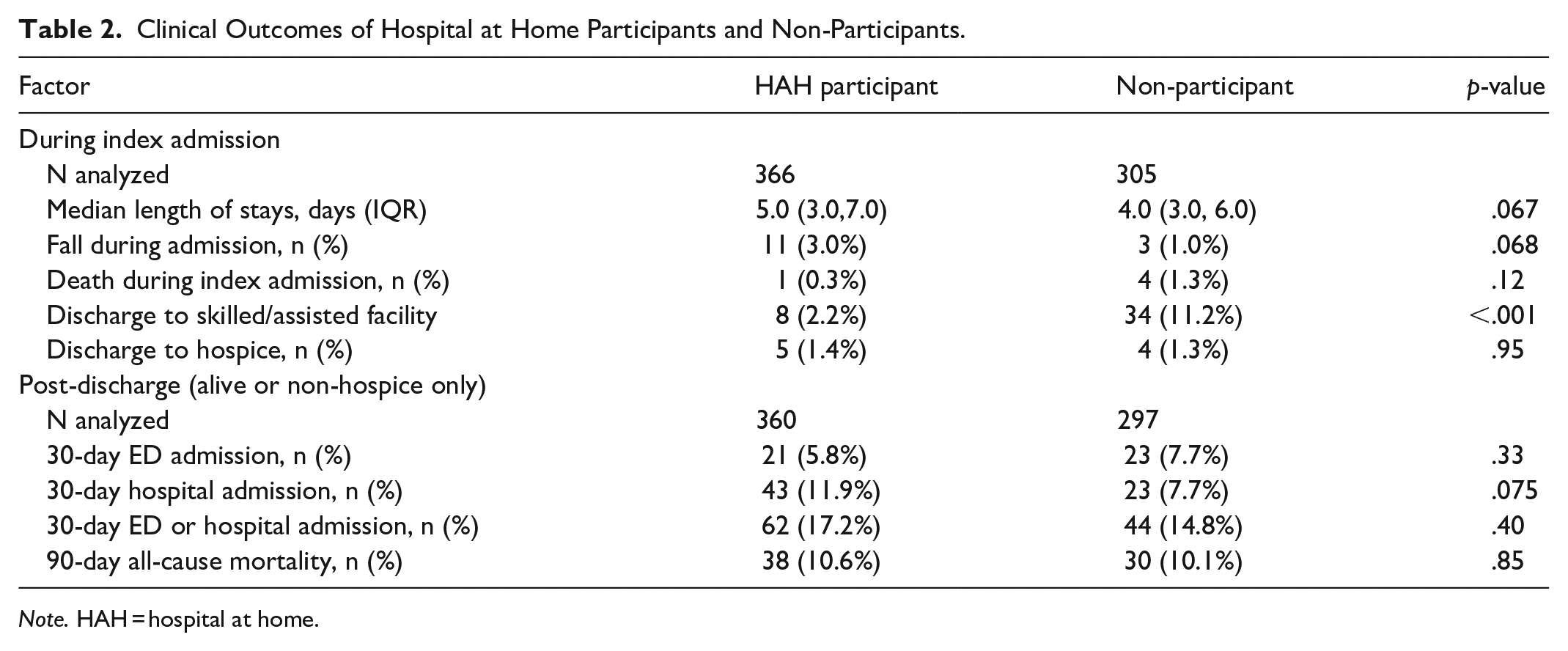
Note. HAH = hospital at home.
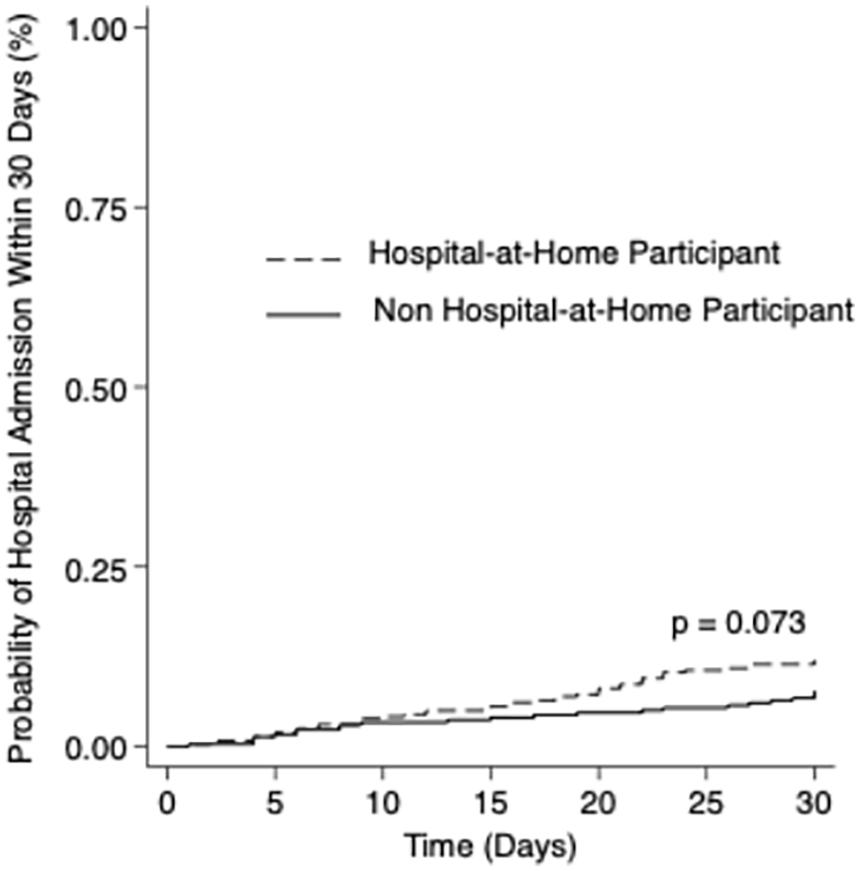
Unadjusted Kaplan-Meier curve comparing 30-day hospital admissions among participants (n = 360) and non-participants (n = 297) in a hospital-at-home program who were discharged from index admission either alive or not on hospice.
Survival Analysis for 30-day Hospital Admission.
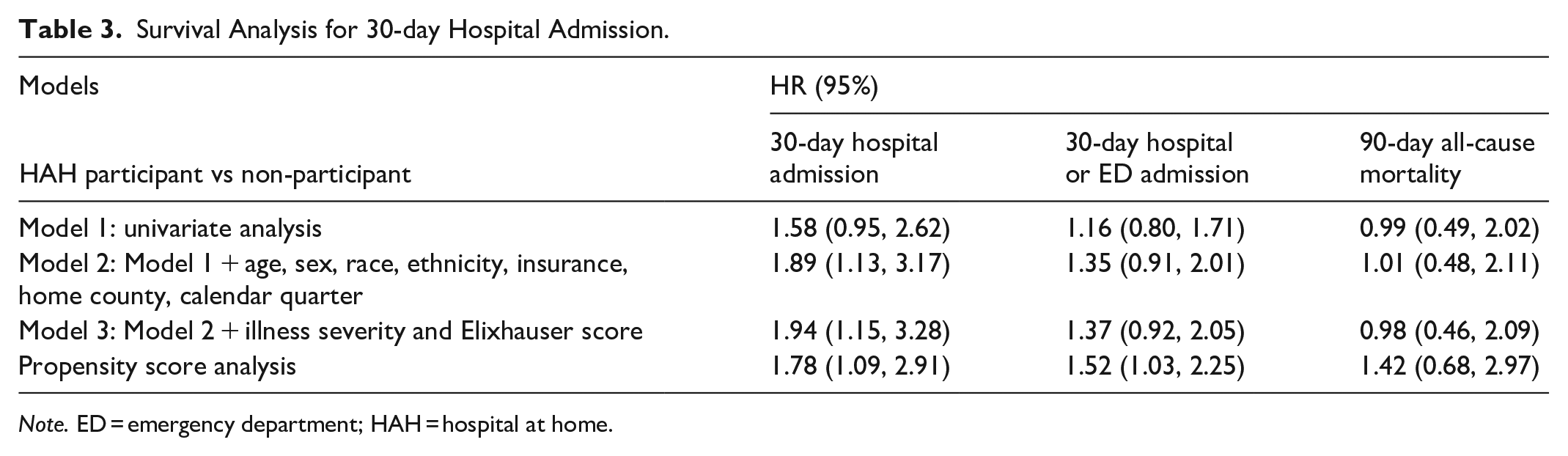
Note. ED = emergency department; HAH = hospital at home.
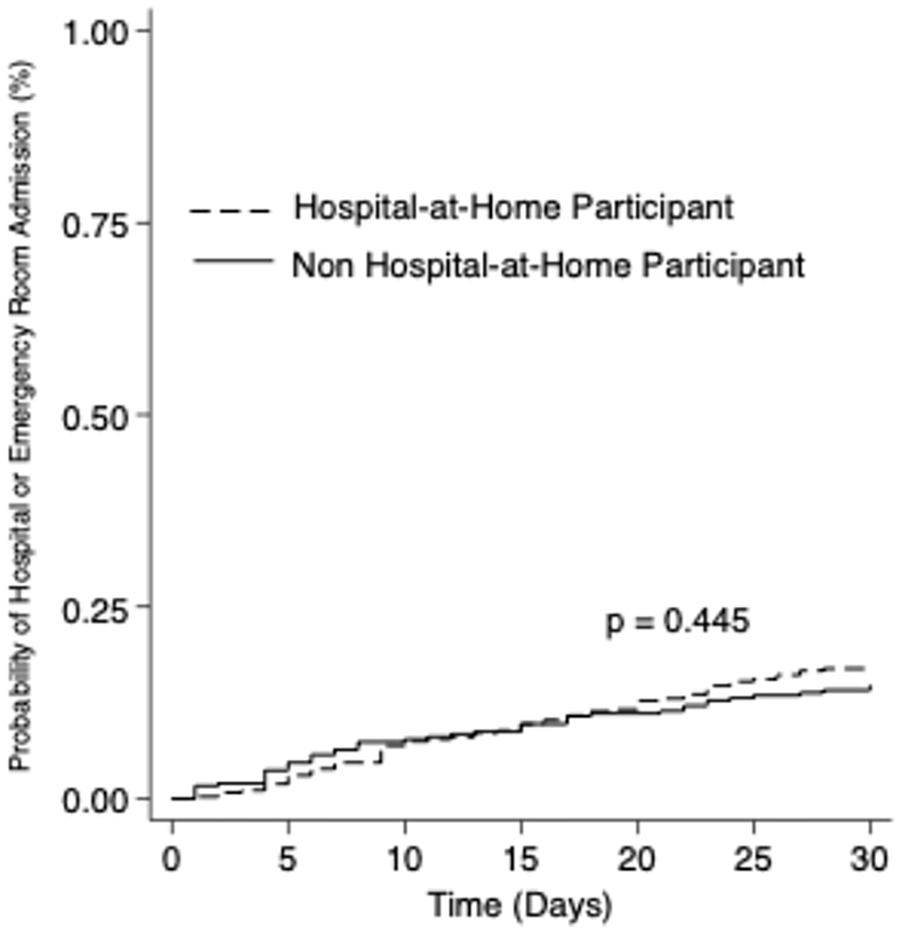
Unadjusted Kaplan-Meier curve comparing 30-day hospital or emergency room admission among participants (n = 360) and non-participants (n = 297) in a hospital-at-home program who were discharged from index admission either alive or not on hospice.
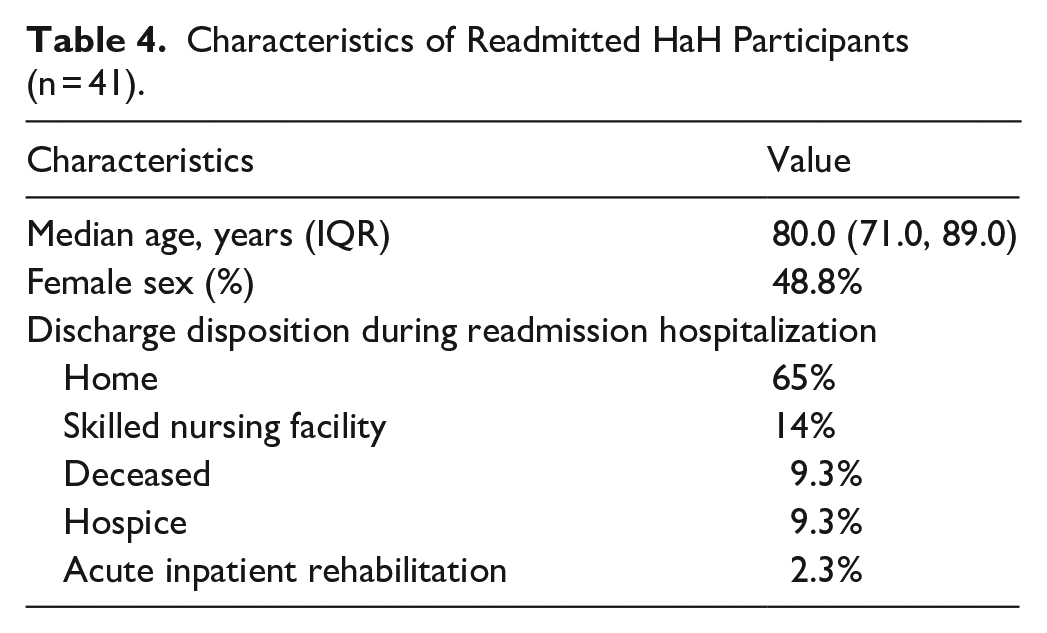
To further investigate potential causes of higher 30-day readmission rates in HaH participants, we reviewed data on the 41 participants who were readmitted within 30 days after discharge from HaH (Table 4). Readmitted patients were older than those who were not readmitted (median: 80.0 vs 76.0 years) and more likely to be male (51.2% vs 46.4%). After the readmission, 35% of readmitted patients had discharge dispositions other than home. Fourteen percent went to a skilled nursing facility, 9.3% deceased, 9.3% went to hospice care, and 2.3% went to acute inpatient rehabilitation.
Characteristics of Readmitted HaH Participants (n = 41).
Although there were more falls in HaH, only 1 fall resulted in injury, and that was minor (Table 5). The falls did not contribute to readmission. HaH participants were less likely to be discharged to a skilled nursing or assisted living facility (2.2% vs 11.2%, p < .001)
Falls Reported Among HAH and Non-HAH Enrollees.
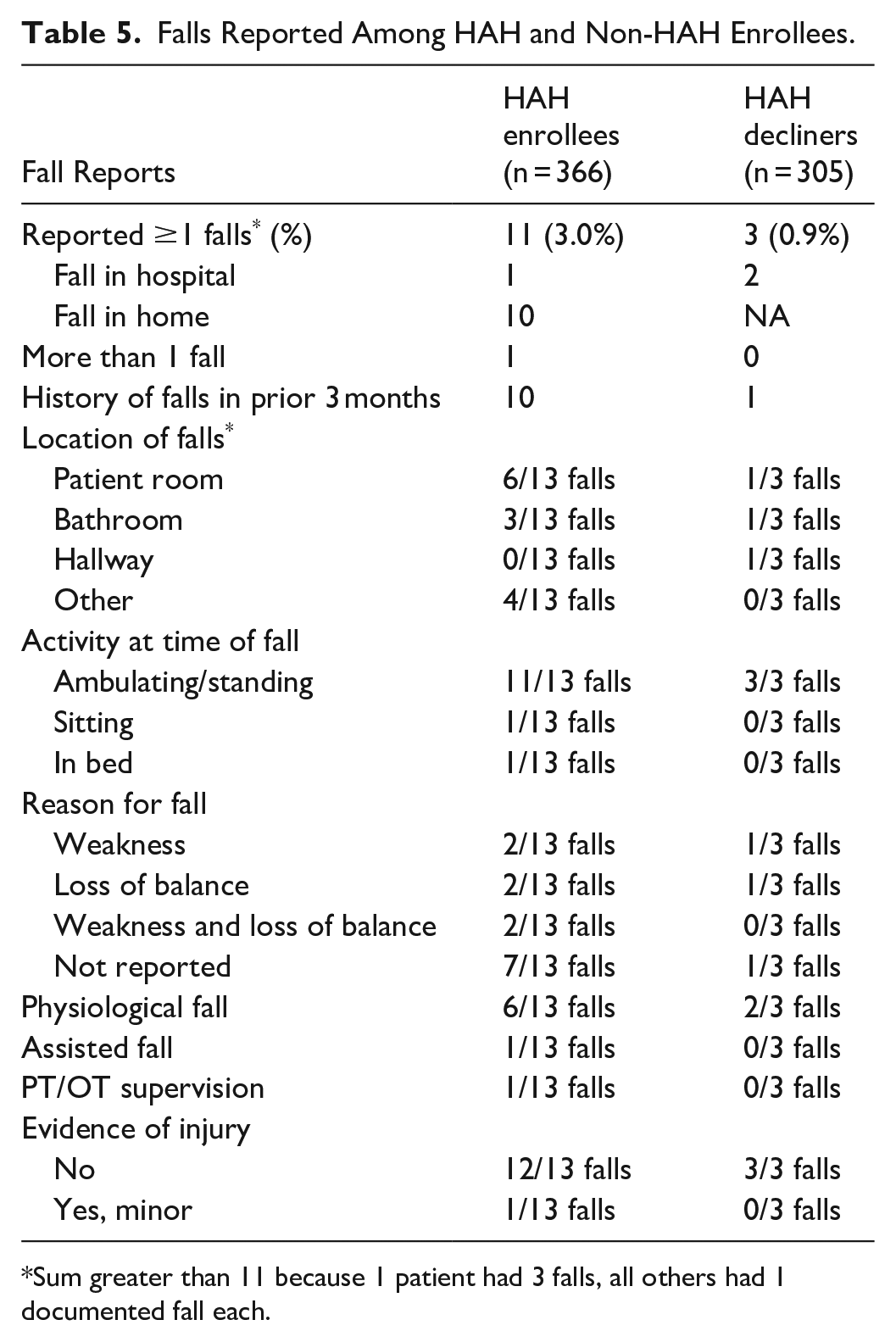
Sum greater than 11 because 1 patient had 3 falls, all others had 1 documented fall each.
Discussion
In this non-randomized comparison between an emerging HaH and brick-and-mortar hospitalization, we used propensity score matching to minimize confounding between the groups. We demonstrated that patients admitted to HaH had a greater risk of readmission within 30 days of discharge, but no difference in mortality. Although length of stay differences did not meet statistical significance, there was a trend toward longer length of stay at HaH. Although we were not powered to detect a difference in falls, there is a signal that falls were more common with HaH.
Our findings are largely consistent with a recent meta-analysis of HaH programs, but with some important differences. 6 We found no difference in 90-day mortality which seems consistent across studies. On average, length of stay was 1 day longer for HaH participants although it did not reach statistical significance. In a meta-analysis, length of stay for patients in HaH was substantially longer than brick and mortar. 6 Our study differed from most randomized controlled trials in finding a greater risk for readmission within 30 days for patients admitted to HaH. However, our readmission rate for patients in HaH (11.9%) was similar to an uncontrolled evaluation of a similarly designed and relatively new HaH program (9.7%). 18 The newer HaH programs have an expanded range of eligible patients (more diagnoses) and are also implementing protocols that are new to them. It would stand to reason that readmissions may be higher earlier in the tenure of the program.
We conducted a more detailed analysis of the patients who were readmitted and found that one-third of them did not get discharged home after their readmission. This, combined with the non-significant increase in falls for HaH participants, suggests that HaH participants were inadequately screened by physical therapists (PTs) or occupational therapists (OTs) prior to enrollment and that a subset of these patients would have been identified as requiring a discharge disposition other than home (e.g., skilled nursing facility). Like other HaH programs, ours did not have a standard protocol for ordering PT/OT evaluations for patients prior to enrollment. PT/OT evaluations were ordered on an as-needed basis, guided by clinical judgment.
In our review of the literature, there are no standardized guidelines regarding PT/OT services evaluation prior to admission to these programs. Current literature demonstrates significant variability in the timing and engagement of these services within HaH models, with some programs involving PT/OT evaluation as part of the initial care plan, while others evaluate their needs on a case-by-case basis.26-28 Common barriers of receiving HaH care includes functional disability and limited social support; however, the decision to involve PT/OT services are typically made after ongoing assessment of patient’s needs throughout the hospitalization.29,30 Guidelines from the American Heart Association and the American College of Surgeons report that a comprehensive evaluation of functional abilities are useful prior to acute hospital discharge, however they emphasize individualized assessments, and multidisciplinary involvement should guide these decisions during the transition to post-acute care.31,32 Further research regarding the timing and approach to standardized protocols for rehabilitation services may help to identify those patients at risk for readmission under HaH programs.
We have not seen documentation of falls in HaH programs and our evaluation suggested higher falls among HaH patients, but it was not statistically significant. Patients enrolled in HaH may be more likely to get out of bed without assistance or not have ready access to assistance. Additionally, the home environment may have other risks such as steps that can increase the risk of falls. We believe that most of these factors can be mitigated but will require special attention by HaH programs. The evaluated program has already implemented several safeguards to prevent falls in the home including training physicians on medicines that increase falls, having a lower threshold for physical therapy, and improving patient education about falls risk.
This study has several limitations that influence the strength of our assertions. The intervention and control groups were not randomly assigned. People in the control group were offered HaH but declined. Baseline characteristics between the groups were different by race/ethnicity and in the severity of illness index. Patients who declined HaH had greater severity. Our measure of complexity, Elixhauser Comorbidity Index, was similar between the groups. Moreover, patients who declined may have had other social reasons for declining participation that were not measured by our processes. These other social barriers would likely bias results toward worse outcomes among brick-and-mortar patients. In uncontrolled analyses, we would expect greater severity to augur poorer outcomes with regard to length of stay and readmissions. However, in our uncontrolled analyses, we did not see a statistical difference and the point estimate was in favor of brick-and-mortar. When we tried to account for the lack of randomization by controlling for confounders and using propensity score matching, the difference in readmissions became statistically significant in favor of brick-and-mortar. This study was also conducted early in the tenure of a HaH program when new protocols were being implemented by new teams. A subsequent analysis, once the program is more mature, could indicate whether a HaH program can improve with more experience. Lastly, because this was a pragmatic and retrospective evaluation, we did not have measures for other outcomes of interest such as pressure-related injuries, iatrogenic infections, delirium, or patient satisfaction. Clearer documentation and validation of these items in the EHR could facilitate more complete pragmatic evaluations.
This report has several implications. Although the prevailing evidence around HaH suggests fewer readmissions, that may not always be true, particularly early in the development of a program and with broader indications for the use of HaH. That said, readmissions are not the full picture of the benefit of the program, and evaluation of a program can identify opportunities for improvements. This program has already identified ways to reduce falls and has been working on readmission reduction. Secondly, overall, HaH outcomes in this study were not substantially different from brick-and-mortar. As such, we confirm that it represents a reasonable approach to acute care, particularly when access to brick-and-mortar is limited.
In this study, we document the experience of 1 HaH program early in its development and confirm safety and similar outcomes. This evaluation allowed us to identify specific areas for possible improvement including falls and readmissions. Other HaH programs can benefit from internal evaluation as a way to identify opportunities for improvement. Moreover, HaH remains a viable alternative to brick-and-mortar and may be preferred by many patients.
Footnotes
Author Contributions
NAKE, ED, JK, BB, MU, and DAD contributed to the study conception and design. Data collection and analysis were performed by NAKE, ED, BB, and DAD. All authors contributed to the interpretation of the analyses. The first draft of the manuscript was written by NAKE and DAD and all authors revised it critically for important intellectual content. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors were employed by UNC Health or UNC School of Medicine during the conduct of this research. The program evaluated in this manuscript is operated by UNC Health.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Compliance with Ethical Standards
This study was reviewed by the UNC Institutional Review Board (Study #22-1495) which determined that the risk involved in this research is no more than minimal. There was no requirement for consent.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Data Availability Statement
Analysis was conducted using private electronic health record data. It may be made available for appropriate use by request.