
Abstract
Aims:
To assess the prevalence and risk factors for chronic kidney disease (CKD) among adults with type 2 diabetes within primary care.
Methods:
This cross-sectional study evaluated 1319 individuals receiving standard care across 26 primary units from July 2017 to January 2023. The estimated glomerular filtration rate (eGFR) and albuminuria were used for the diagnosis of CKD. CKD was defined by eGFR values of <60 mL/min/1.73 m2 and/or albumin-to-creatine ratio ≥30 mg/g. Logistic regression was applied to identify factors associated with CKD and study variables.
Results:
The median age of participants (60.6% females) was 55 years and the median diabetes duration was 10 years. The overall CKD prevalence in the study population was 39.2%. Within the CKD group, the prevalence rates of albuminuria, albuminuria coupled with low eGFR and isolated low eGFR were 72.1%, 19%, and 8.9%, respectively. The prevalence of CKD was 30.6% among participants under 40 years old and a higher value was observed in middle-aged adults with early-onset diabetes (at age <40 years) compared with the later-onset group. Multivariable analyses identified associations between CKD and factors such as age, the male sex, diabetes duration, hypertension, retinopathy, and metformin use.
Conclusion:
A relatively high prevalence of CKD, especially in non-elderly adults, was revealed in this primary care study. Early recognition strategies for CKD are crucial for timely prevention within primary care.
Keywords
Introduction
Type 2 diabetes (T2D) is a global public health challenge with its increasing prevalence and wide range of associated complications. 1 Chronic kidney disease (CKD) stands out as one of the most prevalent of these complications affects approximately 30% to 40% of individuals with T2D during their lifetime. 2 People living with diabetes-related CKD face an elevated risk of progressing to end-stage renal disease, cardiovascular complications, and reduced life expectancy. 3 In addition, advanced CKD significantly reduces a patient’s quality of life and increases healthcare expenditures. 4
The burden of diabetes is particularly pronounced in low- and middle-income countries (LMICs), where approximately 80% of diabetes cases are concentrated and access to care (including renal replacement therapies for patients with kidney failure) is limited.5 -7 Due to the current trend of CKD burden attributable to T2D, it is anticipated that diabetes complications will increase the demand for healthcare services globally. 8 In response to the escalating burden of diabetes, the World Health Organization launched the Global Diabetes Compact in 2021, aiming to mitigate disparities in access to diagnosis and treatment, ensuring universal care through primary health care centers. 9
The most effective strategy to reduce the burden of diabetes-related CKD among those already diagnosed with T2D is to achieve diabetes care goals through comprehensive care and to diagnose and treat CKD in its early stages.2,10,11 Despite the noninvasive and cost-effective nature of CKD testing, rates of testing, and diagnosing in primary care settings remain low.12 -14 As early-stage CKD is asymptomatic in most patients, poor performance of screening tests and incomplete screening results in missed opportunities for early intervention. Moreover, there is a lack of data on diabetes-related complications in LMICs, including diabetes-related CKD in primary care settings, where the majority of patients are diagnosed with the condition during its late stages.14,15 Data scarcity impedes healthcare systems from accurately identifying and characterizing the population at the highest risk for preventive interventions and efficient resource allocation.
Notably, some subgroups of T2D individuals experience early and rapid CKD progression.16,17 However, potential explanations for associated factors and the magnitude of their effect still need to be fully understood. Despite reported epidemiological variations among populations and the magnitude of the public health impact of CKD, there is still a paucity of research on the clinical characterization of CKD in LMICs, which harbor additional unique risk factors. This study aims to determine the prevalence of CKD and its associated factors in patients with T2D receiving conventional care in primary care settings who were participating in a quality improvement initiative.
Materials and Methods
Study Design and Participants
This cross-sectional study was conducted among adult T2D patients receiving conventional care at primary care centers within the public healthcare system in Mexico City. Participants were invited to participate in the healthcare service program known as DIABEMPIC (DIABetes EMPowerment and Improvement of Care), a quality improvement initiative aimed at accelerating evidence-based interventions to achieve diabetes care goals achievement, achieving the early identification of diabetes-related complications and enhancing health-related quality of life in participants. A detailed description of procedures and recruitment has been provided previously. 18 Briefly, this multi-component intervention, which is provided free of charge and supported by the Mexico City government health ministry, includes an interdisciplinary care model approach, a diabetes self-management education program, screening and diagnosis of complications, on-site services, and pharmacological treatment. Previous reports have documented the achievement of diabetes care goals, factors associated with better outcomes and the prevalence of certain diabetes-related complications within this program.18 -20
Participants were enrolled between July 2017 and January 2023. They were referred from primary care units to the Clinic Specialized in Diabetes Management in Mexico City, which is part of the primary care stewardship and where the comprehensive care program is administered. Our exclusion criteria were acute or chronic conditions necessitating immediate hospital care, pregnancy, and diagnoses of diabetes other than T2D. Ethical approval was obtained from Mexico City Ministry of Health ethics committee (609-01-01-18). All participants gave their verbal and written informed consent.
The sample size was calculated using the formula for estimating prevalence in cross-sectional studies, considering a 95% confidence level, desired margin of error of 0.05, with an assumed prevalence of CKD from previous studies (30-40%) 2 additionally to risk factors associated with CKD to be included in the logistic regression model. The estimated sample size was 1010 patients including an additional 10% for possible missing data.
Measurements and Data Collection
Demographic characteristics, time since diagnosis, comorbidities, current pharmacological treatment and physical examination findings were retrieved from medical records and confirmed during medical interviews. The status of diabetes-related complications, including the comprehensive assessment of retinopathy and diabetic neuropathy, was updated. Biochemical data, including serum creatinine and the urinary albumin-to-creatine ratio (ACR), were collected from each participant upon enrollment.
The prevalence of CKD was determined based on the presence of reduced estimated glomerular filtration rate (eGFR) and albuminuria in the absence of clinical indicators of other causes of kidney disease. 21 The 2021 CKD-EPI equation was employed to estimate eGFR from the serum creatinine, age, and sex of participants per current guidelines. Albuminuria was assessed using the urinary ACR. CKD was defined by eGFR values of <60 mL/min/1.73 = m2 and/or albuminuria as indicated by ACR ≥30 mg/g. Sample collection for biochemical tests was postponed in participants reporting exercise within 24 h, infection, fever, or menstruation.
Risk categories of CKD, according to the Kidney Disease Improving Global Outcomes (KDIGO) classification, were used to define the risk of progressive CKD, cardiovascular events, and mortality. This staging system combines the severity of albuminuria and decreased eGFR to categorize individuals based on risk. 21
Statistical Analysis
The Kolmogorov-Smirnov test was employed to test the null hypothesis that continuous data adhere to a normal distribution. Data are reported as the mean ± standard deviation for normally distributed variables or as the median and interquartile range for non-normally distributed variables. Categorical variables are expressed as frequencies and percentages. Differences between participants with and without CKD were evaluated using Student’s t-test or the Mann-Whitney U test, as appropriate, for continuous variables and Pearson’s chi-square test or Fisher’s exact test, as appropriate, for categorical variables.
The prevalence of rates of albuminuria, eGFR <60 mL/min/1.73 m2 and overall CKD were estimated with 95% confidence intervals (CIs) through bootstrap resampling of 1000 resamples. CKD’s prevalence was further stratified according to the KDIGO severity classification, early- or later-onset diabetes diagnosis and current adulthood stage. Early-onset diabetes (EOD) and later-onset diabetes (LOD) were defined as diagnoses made before and after the age of 40 years, respectively. 22 Logistic regression analyses were conducted on variables with a P value ≤.20 in univariate analyses using the Wald test to determine CKD associated factors, presented as odds ratios (ORs) with corresponding 95% CIs. Statistical model building was guided by the minimization of variables method to obtain the most parsimonious model evaluated by the Akaike information criterion and results generalizability. 23 A P-value of <.05 was considered statistically significant. Statistical analyses were performed using SPSS (version 25, IBM Corp, Armonk, NY) and Jamovi (version 2.3).
Results
A total of 1453 patients with T2D were assessed between July 2017 and January 2023. Among them, 133 were excluded due to missing data on eGFR, albuminuria, or other CKD-related causes unrelated to T2D, leaving 1319 participants for the analysis (516 with and 803 without CKD).
The prevalence of CKD (eGFR <60 mL/min/1.73 m2 and/or albuminuria) was 39.2% (95% CI: 36.8%-41.6%). Specifically, a reduced eGFR (<60 mL/min/1.73 m2) was observed in 10.9% (9.2%-12.4%) of participants, while albuminuria was present in 37.6% (34.9%-40.2%) of them. Among those with CKD, 72.1% had isolated albuminuria, 19% had albuminuria coupled with low eGFR and 8.9% had isolated low eGFR (Figure 1). According to the KDIGO classification, the reported risk of CKD was categorized as follows: 61.2% low risk, 23.4% moderately increased risk, 10.1% high-risk, and 5.4% highest risk (Supplemental Figure 1).

Prevalence of chronic kidney disease and its components in the entire cohort.
The sociodemographic and clinical characteristics of the study population and comparisons between patients with and without CKD are presented in Table 1. Patients with CKD were older and more frequently male, had lower education attainment, were more likely to have a sedentary lifestyle and had higher rates of hypertension, ischemic heart disease, diabetic neuropathy, and uncontrolled hypertension. They were also diagnosed with T2D at a younger age, had a longer duration of T2D and exhibited higher blood glucose concentrations. Furthermore, participants with CKD reported greater usage of insulin, metformin, loop diuretics, inhibitors of angiotensin-converting enzyme inhibitors (ACEi), angiotensin receptor blockers (ARB), beta-blockers, and calcium antagonists. Supplemental Tables 1 to 3 compare sociodemographic and clinical characteristics of patients with and without albuminuria, reduced glomerular filtration rate, and albuminuria with reduced glomerular filtration rate.
Sociodemographic and Clinical Characteristics According to CKD Status.
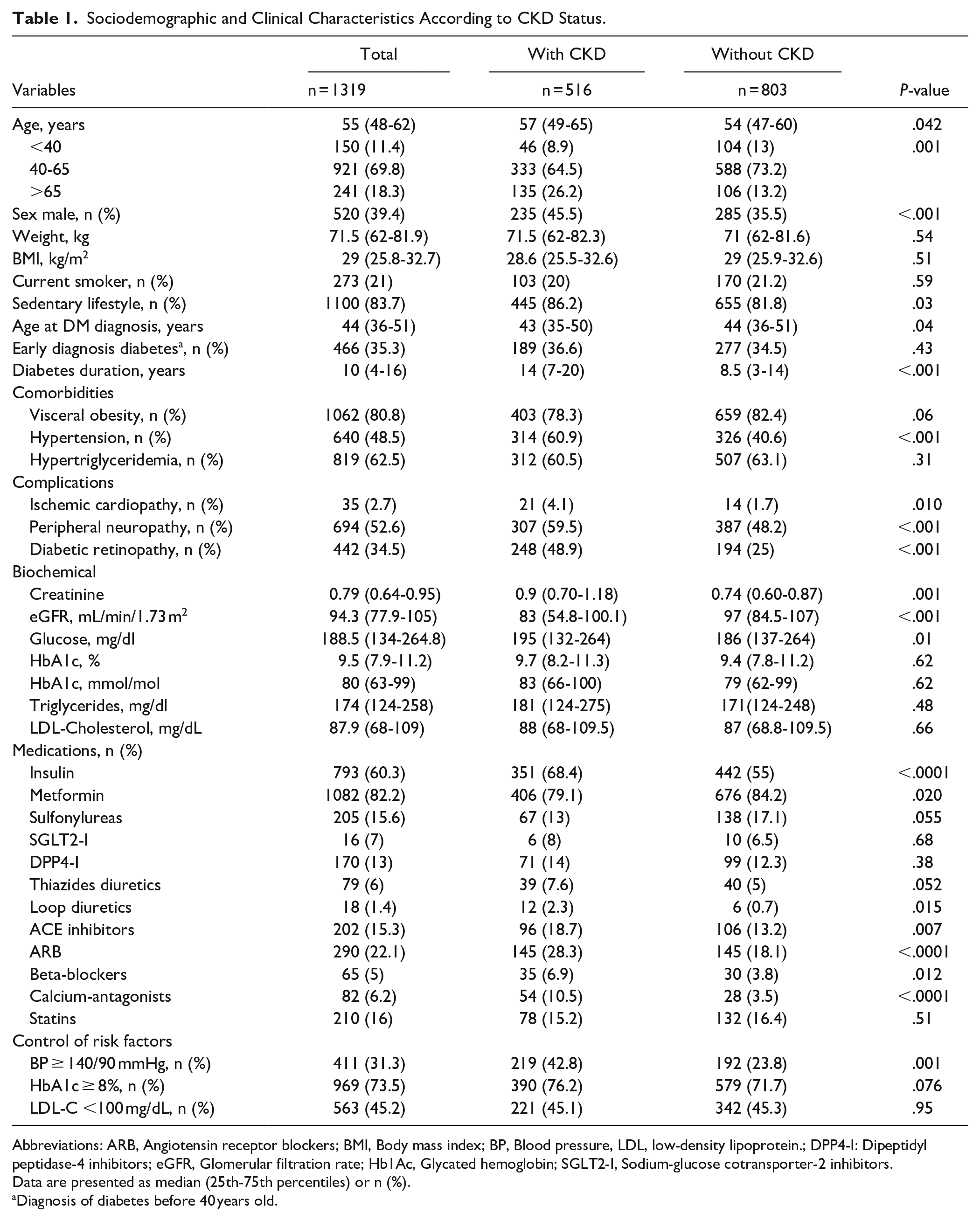
Abbreviations: ARB, Angiotensin receptor blockers; BMI, Body mass index; BP, Blood pressure, LDL, low-density lipoprotein.; DPP4-I: Dipeptidyl peptidase-4 inhibitors; eGFR, Glomerular filtration rate; Hb1Ac, Glycated hemoglobin; SGLT2-I, Sodium-glucose cotransporter-2 inhibitors.
Data are presented as median (25th-75th percentiles) or n (%).
Diagnosis of diabetes before 40 years old.
Prevalence rates of albuminuria, reduced eGFR, and overall CKD (albuminuria or reduced GFR) differed according to diabetes duration (Figure 2), with the highest prevalence observed in individuals with diabetes durations of >10 years (50.2%). The prevalence rates of microalbuminuria (ACR ≥30 and ≤300 mg/g) and macroalbuminuria (ACR ≥300 mg/g) were 25.2% and 10.1%, respectively. The prevalence rates of microalbuminuria and macroalbuminuria stratified by the eGFR category according to KDIGO classification are shown in Supplemental Figure 2.
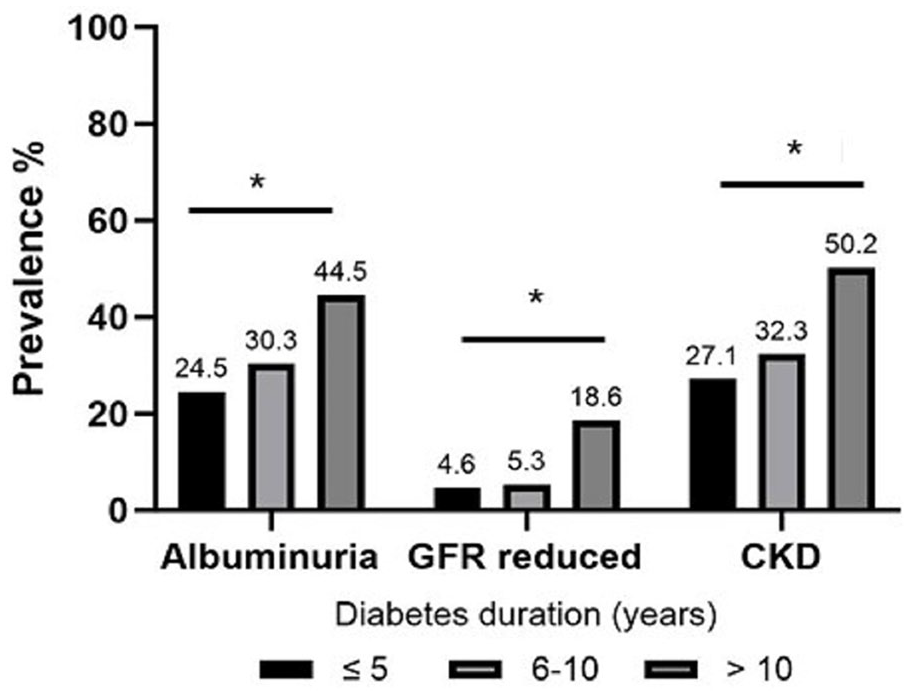
Prevalence of albuminuria, reduced glomerular filtration rate, and chronic kidney disease according to diabetes duration intervals.
According to the current stage of adulthood, the prevalence rates of CKD in early adulthood participants (<40 years), middle-aged adults (40-65 years), and the elderly (>65 years) were 30.6%, 36.5%, and 45.2%, respectively.
As shown in Figure 3, the prevalence of CKD among middle-aged participants was higher in individuals with EOD compared with the LOD group (44.4% vs. 32.2%, P < .001). Additionally, the overall prevalence of CKD was higher in men (45.5%, [95% CI: 40-48]) compared with women (35%, [95% CI: 32-38]) as shown in Supplemental Figure 3.

Prevalence of CKD according to age intervals in participants with early-onset diabetes (EOD) and later-onset diabetes (LOD).
Multivariable analyses identified several factors significantly associated with the risk of CKD (Figure 4), including age (OR = 1.01; 95% CI: 1.0-1.02), the male sex (OR = 1.7; 95% CI: 1.133-2.18), diabetes duration exceeding 10 years (OR = 1.78; 95% CI: 1.35-2.34), hypertension diagnosis (OR = 1.95; 95% CI: 1.51-2.51), diabetic retinopathy (OR = 1.97; 95% CI: 1.50-2.58), and metformin use (OR = 0.65; 95%CI: 0.47-0.89), with an area under the curve of 0.70. Factors associated with albuminuria, reduced eGFR, and the co-occurrence of both were also identified. Factors related to albuminuria included the male sex, diabetes durations of >10 years, hypertension, diabetic retinopathy, and metformin use. Factors associated with reduced eGFR were age, diabetes durations of >10 years, hypertension, diabetic retinopathy, and ARB use.

Associated factors to chronic kidney disease and their components by binominal logistic regression in the study population.
Discussion
This study reveals a relatively high prevalence of diabetes-related CKD and associated risk factors among patients with T2D receiving conventional care in primary care settings of a middle-income country. Only a few previous investigations had addressed the prevalence of CKD in particular subgroups of patients with T2D. Particularly notable is the elevated prevalence observed among young adults and middle-aged individuals, as well as those with early-onset diabetes. The significance of quantifying albuminuria, an element of renal assessment with poor execution in clinical practice, is underscored, revealing that the non-evaluation of albuminuria could hide the majority of individuals affected with CKD. Conducted in real-world primary care settings, our findings emphasize the imperative of healthcare pathways that facilitate the timely diagnosis and treatment of CKD in the early stages of the disease to prevent its progression.
The prevalence of CKD varies significantly depending on the definition employed (low eGFR, albuminuria, or both) and the clinical setting where the study is carried out (primary care or hospital care). Notably, our study focused on patients in primary care, excluding those with advanced CKD requiring second or third-level care. Nevertheless, we observed a CKD prevalence of 39.2%, which is relatively high compared with rates reported in similar primary care studies conducted in Finland and Greece (34.7% and 45%, respectively).24,25 It is noteworthy that, compared with participants in these studies, participants in our study were approximately a decade younger, making the prevalence obtained in this study relatively high, given that the study participants were younger.
Our findings suggest that CKD may be occurring prematurely in our population, as evidenced by the high prevalence rates among individuals aged 6 to 10 years and over 10 years of diabetes duration, compared to data from the UKPDS study indicating CKD development in 29% to 38% of patients with T2D after a median follow-up period of 15 years. 26
Per our findings, the eGFR evaluation identified only 3 of the 10 cases of CKD, which underscores the importance of albuminuria measurements in clinical practice. Unfortunately, albuminuria measurement is often unavailable in the public primary healthcare system of many countries, including Mexico. 14 The dipstick test for urinary protein, which is the most frequently used test in LMICs due to its accessibility, correlates poorly with higher-sensitivity tests, particularly in microalbuminuria-range concentrations. 27 Despite albuminuria being a clinically relevant tool for determining the prognoses of renal and cardiovascular conditions and monitoring therapeutic response, it remains underutilized even in high-income countries.12,28 Screening for CKD is recommended yearly after T2D diagnosis.10,21 In this work, we demonstrate how the underutilization of albuminuria testing hampers the diagnosis and treatment of the majority of CKD cases (particularly those in the initial stages), which represents a missed opportunity for risk mitigation.
Our study also highlighted the disproportionately high prevalence of CKD among young and middle-aged adults with EOD. Compared with those diagnosed later in life, an earlier-onset diagnosis is associated with a higher risk of diabetes-related complications and earlier death in affected individuals, most of them middle-aged adults, magnifying the diabetes disease burden.22,29 Recently, in a prospective cohort study, it was reported that the risk of CKD-associated with the duration of diabetes is higher when diabetes is diagnosed at a younger age. 30 Some world regions and ethnic groups may be facing a particularly increased incidence of diabetes-related complications derived from the early-onset of the disease. Mexico has one of the highest rates of diabetes diagnosis in the 20- to 39-year age range, which may contribute to explaining one of the highest burdens of the disease worldwide, including the CKD burden.22,31 -33 Thus, this work adds key inputs to guide decision-making and focus efforts on the timely diagnosis and management of the condition in this high-risk population.
It is essential to understand differences in risk factor profiles and specific features of diabetes across populations to design effective strategies to identify and control the risk factors for diabetes. In this regard, our study identifies clinical characteristics associated with early CKD stages easily identifiable by healthcare providers in routine practice, increasing diagnosis awareness and facilitating early interventions. Some of these characteristics have been reported to be associated with end-stage CKD. 34 In this study, we identified significant risk factors in the early stages of CKD, including hypertension, diabetic retinopathy, the male sex, and longer diabetes durations. Although this study does not establish causality, the association of metformin with a lower risk of CKD aligns with previous reports, suggesting its potential benefits in mild-to-moderate CKD stages. 35
To mitigate the burden of diabetes-related kidney disease, public policies must be implemented to reduce the incidence of new diabetes cases, especially in early adulthood. Additionally, there are also essential opportunities for people already diagnosed with diabetes. Disease management with the attainment of diabetes care goals (control of glycemia, blood pressure, and lipid levels) can be reached within comprehensive care schemes, reducing the risk of CKD onset or progression.11,18,36 Furthermore, the timely identification of kidney damage or dysfunction is critical for identifying high-risk patients for a diversity of diabetes-related complications and offering therapeutic interventions to modify the disease’s aggressive behavior that is characteristic of this population. 21 The identification and treatment of most patients in the early stages of diabetes-related CKD must occur in primary care settings since most patients are being managed in such settings. Therefore, our work helps to appreciate the magnitude of a hidden healthcare need and proposes the recognition of specific risk groups precisely in primary care settings. Compliance with the screening and diagnosis of CKD recommendations must be guaranteed, for which the care schemes and pathways must include renal assessment and the prompt referral of individuals who require specialized care.
The strengths of our study include the prospective collection of clinical data using standardized methods, data quality enhancement, and the inclusion of participants from a large number of primary healthcare centers, making our findings reasonably representative of the T2D population in primary care settings in Mexico and the Latin America region. Nevertheless, the study also had a few limitations. First, our findings were based on the observational, cross-sectional nature of the analyses, which means causal inferences cannot be established. Second, the generalizability of our findings to other populations is uncertain and warrants further studies. Nevertheless, this cohort sample fairly represents the T2D population in primary care settings in Mexico and Latin America, with potential similarities to other populations. Third, interactions effects analysis was not performed as it was beyond the scope of the current study.
In conclusion, diabetes-related CKD is frequent (39.3%) in this contemporary primary care prevalence study, with retinopathy, hypertension, diabetes duration, the male sex, and age being the major risk factors. Our results contribute to the identification and characterization of people who are most predisposed to this condition. This work also reveals that a relevant proportion of patients with T2D in primary care are highly predisposed to CKD; however, healthcare providers and healthcare systems have not identified this risk.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241259325 – Supplemental material for Prevalence of Chronic Kidney Disease in Individuals With Type 2 Diabetes Within Primary Care: A Cross-Sectional Study
Supplemental material, sj-docx-1-jpc-10.1177_21501319241259325 for Prevalence of Chronic Kidney Disease in Individuals With Type 2 Diabetes Within Primary Care: A Cross-Sectional Study by Ruben Silva-Tinoco, Teresa Cuatecontzi-Xochitiotzi, Luis E. Morales-Buenrostro, Abraham Edgar Gracia-Ramos, Carlos A. Aguilar-Salinas and Lilia Castillo-Martínez in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We want to acknowledge Eileen Guzman and Viridiana de la Torre for their support and contribution to the interdisciplinary team care process.
Author Contributions
RST and TCX conceptualized and designed the study. TCX and AEGR acquired the data. RST and LCM made the statistical analysis. RST, LEMB, AEGR, CAAS, and LCM wrote the manuscript. All authors provided critical reviews on multiple iterations and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
The study was approved by Mexico City Ministry of Health Ethics Committee (609-01-01-18). All participants provided verbal and written informed consent.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.