
Abstract
Context:
Aging and increasing comorbidities in the population are leading to more complex care for patients and primary healthcare providers. Community organizations (COs) may play a role in the services offered to support patients with chronic diseases (PCDs) but there are currently no clear guidelines to support primary healthcare providers in linking patients to COs.
Objectives:
The aim of this study was to describe the role of primary healthcare providers regarding linking PCDs to COs by: (1) describing linking activities; and (2) identifying the main facilitators and barriers associated with these activities.
Methods:
This scoping review was based on the Arksey and O’Malley method, completed by Levac, Colquhoun, and O’Brien. Related keywords were used in 7 databases to search relevant studies. After the initial screening, 135 full texts were assessed for eligibility by 2 reviewers using inclusion/exclusion criteria. Empirical studies describing activities performed by primary healthcare providers in linking PCDs to COs or describing facilitators or barriers to linking activities were included. Studies describing activities linking to other services than COs or located in emergency departments were excluded.
Results:
In total, 28 studies were included. Information reported in the studies was classified into 8 main linking activities: capacity development, patient identification, assessment, information, planning, referral, follow-up, and collaboration. Facilitators and barriers to these activities were related to intrapersonal characteristics of providers and patients, professional practice, work environment, relationships, and external influences. Healthcare providers’ involvement was often adapted according to their field of practice.
Conclusion:
This scoping review details the role of primary healthcare providers when linking PCDs to COs in a collaborative and interdisciplinary context, which can be adapted to clinical practice by providers, experts, or stakeholders to support improvement in chronic care management.
Introduction
The prevalence of chronic diseases (CDs) has risen significantly over the last 15 years, with CDs being the leading cause of global deaths worldwide.1,2 A growing proportion of the population is diagnosed with multimorbidity and deals with 2 CDs or more.3,4 CDs include a large variety of diagnoses, ranging from cardiovascular diseases to mental health disorders and have a significant impact on the healthcare system, as they are associated with more emergency room visits, more hospitalizations, more challenging healthcare coordination, and increased healthcare services costs.5 -9 CDs increase the complexity of patient care, especially for healthcare providers working in a primary care setting since most of their consultations are with people living with CDs.6 -8,10 Furthermore, when dealing with CDs and multimorbidity, primary healthcare providers are faced with an increase in consultations and intensity of care, more referrals, and more actors involved in care coordination.6,8,11
To better meet the needs of these populations, cross-sector collaboration is increasingly encouraged, as it constitutes a pivotal element in CD management. 1 Among possible partnerships is the collaboration between healthcare teams, patients, and community partners. 1 When it comes to CD management, community organizations (COs) can offer tailored health and social services that further support patients’ needs, such as disease management and education programs, caregiver support, and social support services. 12 Primary healthcare providers practice a range of activities that help link patients to COs. 12 Although these linking activities between patients living with chronic diseases (PCDs) and COs have proven to be useful in CD management, very few studies provided a description of them.12 -14 When it comes to primary care interventions in CD management, linking patients to COs is rarely explored.13,14 There are no clear guidelines to support primary healthcare providers in their role with the patient and the CO, highlighting the need to explore what is currently known on linking activities in primary care settings.
Therefore, the aim of this scoping review was to describe the information about the role of primary healthcare providers in linking PCDs to COs by portraying the linking activities and identifying the main influencing factors associated with them.
Methods
This scoping review relied on the 6-step framework proposed by Arksey and O’Malley, and completed by the Levac, Colquhoun, and O’Brien method.15,16
Identifying the Research Question
The principal question of this study was, “What is the role of primary healthcare providers in linking PCDs to COs?” To narrow down the study topic, the main question was split into specific questions:
- What are the activities practiced by primary healthcare providers in linking PCDs to COs?
- What are the main influencing factors (facilitators or barriers) of these linking activities?
Identifying Relevant Studies
Searches were conducted in the following databases: CINAHL, MEDLINE, Academic Search Complete, SocINDEX, Scopus, Emcare, and HealthStar. Two librarians specializing in healthcare were consulted independently to develop the search strategy around 3 key terms, namely community organizations, primary care, and referral. Each keyword was broken down into synonyms. Terms in the primary care concept also included various healthcare providers known to work in this type of setting, such as physicians, nurses, social workers, and nutritionists or dietitians. To maximize the pool of eligible articles, searches did not include a publication date range. Boolean operators “AND” and “OR” were used and databases were filtered for articles written in English or French since all authors speak both languages. The complete search strategy applied in Scopus is presented in Supplemental Appendix 1.
Study Selection
First, all titles and abstracts were reviewed using the inclusion and exclusion criteria. Then, 2 members of the research team (N.G. and E.H.) independently screened the selected full-text articles using the same criteria. Articles were included if they met the selection criteria. A third member helped to resolve disagreements, as needed. Zotero was used to remove duplicates, screen titles, and abstracts.
Inclusion and exclusion criteria
Studies describing activities performed by primary healthcare providers linking PCDs to COs or describing influencing factors were selected. Since prevention of risk factors is an important part of CDs management, studies focusing on patients with risk factors of CDs were also included. 1 Definitions of CDs included a broad range of long term diseases varying from physical diseases, cancer, neurological, and mental health disorders.1,5 Tobacco use, poor nutrition, physical inactivity, and excessive alcohol use were included in the definitions of risk factors. 1 The description of linking activities had to be sufficiently detailed to allow transferability to other primary care practices and settings. Only full-text empirical studies were included. Studies were excluded if the description of activities was restricted to a unique health condition or event or if linkage concerned emergency departments, specialized care, or services other than COs.
Charting the Data
Data were charted using Excel software. Extracted descriptive information included: authors; year of publication; study location; study design; aim of the study; referring provider; patients’ diagnosis; linking activities; and influencing factors. One team member extracted all the data from the articles and another member validated 25% of the content.
Collating, Summarizing, and Reporting the Results
Data were analyzed, summarized, and reported using inductive thematic analysis to identify key linking activities and influencing factor categories.17,18 Data were analyzed using Excel. Each sentence was examined to identify extracts of qualitative descriptive text associated with linking activities and influencing factors. The length of the extracts depended on the description provided by the authors (brief sentence to small paragraph). Relevant extracts were put in an Excel file and was then reviewed and analyzed to assign a theme. Color coding was used to differentiate the themes and organize the extracts. The extracts were then analyzed again to consolidate the emerging themes and to assure all data were correctly analyzed and sorted. This process was done inductively with multiple iterations. Once all data were classified, the relationships between the themes were identified to organize and synthesize the results. Emerging themes and their classification were reviewed and discussed by 3 other members of the research team (C.H., M.C.C., and E.E.).
Consulting Experts
A 1 h virtual consultation was organized to present the results of the scoping review to 6 primary care experts, identified using a snowball technique. 19 This step aimed to discuss main findings in the context of current practice in primary care and to identify which aspects should be explored further in subsequent studies. Tips and suggestions resulting from this exercise are presented in this article’s discussion.
Results
Search Strategy Results
First, 4386 articles were retrieved from the 7 databases. After removing duplicates, 2208 articles remained for the initial screening and 135 full texts were assessed for eligibility, using the inclusion and exclusion criteria. In total, 28 studies were included in this scoping review. Figure 1 shows the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart reporting the complete process of the study selection.20,21
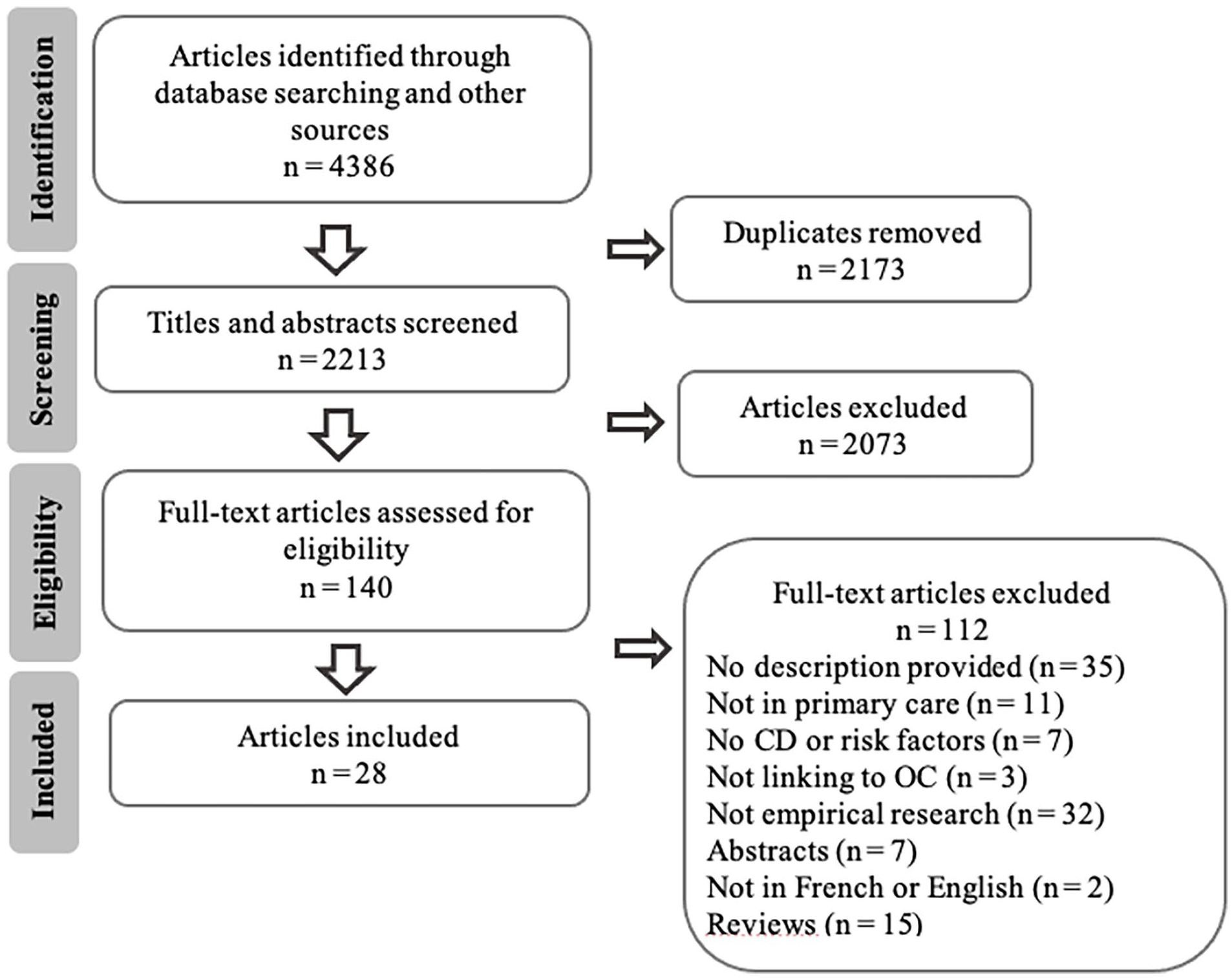
PRISMA flowchart of the study selection.
Characteristics of Included Studies
Table 1 shows the descriptive characteristics of the 28 included studies,22-49 published between 1993 and 2020. The majority (n = 15) originated in the United States.22-36 Canada37 -40 and Australia41 -44 each had 4 studies and 2 studies were conducted in the United Kingdom.45,46 Other countries include Scotland, 47 the Netherlands, 48 and Germany. 49
Descriptive Characteristics of Included Studies.

Social prescribing: range of approaches enabling healthcare providers to connect people to non-medical resources.
The included studies targeted different types of patients. Twelve of them included adults living with a variety of CDs (coronary heart diseases, cerebrovascular diseases, hypertension, diabetes, and chronic kidney diseases),28,32 -35,40 -42,44 -46 4 of which also focused on patients’ unmet needs.28,33,34,46 Three studies targeted patients presenting risk factors associated with CDs, such as tobacco use, poor diet, or sedentarity.25,29,43 Patients with a mental health condition, namely depression or associated psychosocial problems, were included in 4 studies,36,37,47,48 while 6 studies focused on patients living with dementia.23,26,30,31,38,49 Two of these also targeted patients’ caregivers38,49 and 3 others focused solely on caregivers.22,24,27
Many primary healthcare providers were identified as carrying out linking activities, including physicians, nurses, social workers, care or service coordinators with various social or health backgrounds, community link practitioners employed in primary care, physical therapists, psychologists, healthcare assistants, pharmacists, dietitians or nutritionists, and occupational therapists.22 -49 Physicians were included in 23 studies.23 -34,36 -38,40 -42,44,45,47 -49 Nurses and social workers were included in 1622,27,29,30,32,34 -36,38 -41,43,45,47,48 and 10 studies28,29,32,34 -36,38 -40,48, respectively. Seven studies included various available primary care providers.29,32,34,36,38,40,48
Linking Activities
Eight linking activity categories emerged: Capacity development, Patient identification, Assessment, Information, Planning, Referral, Follow-up, and Collaboration. These categories are not mutually exclusive.
Before undertaking linking activities, healthcare providers must prioritize capacity development and be aware of available COs’ services or linking partners.25,27,29,31 -33,49 Then, patient identification should be done to target those who could potentially benefit from COs’ services, based on pre-established eligibility criteria. 28 This process should be quick and systematic.25,30 Assessment, on the other hand, is a more comprehensive process carried out during an appointment with the patient.26,34,43 The goal is to address and understand patients’ needs30,36 and to gather as much relevant information as possible. 30 Then, sharing of information is carried out by a healthcare provider or linking partner through discussion of the potential services with the patient.27,38,39,48 Once the potential services have been narrowed down, needs are discussed more specifically during the planning phase in order to establish and coordinate a specific service plan.22,24,25,28,30,33 -36,38,41,42,47 -49 A referral is then made to facilitate patients’ access to COs.28,38,45,46 Following implementation of services, follow-up can be done with the patient and their network to validate whether initial needs have been met or new needs have emerged.22,24,26,27,34,43,46 Fostering ongoing collaboration between all actors remains important to promote linking activities.24,26 -28,31,33,35,36,38,40,41,46 Table 2 summarizes each linking activity.
Summary of Linking Activities.

Linking Activities and Influencing Factors
As presented above, linking activities are structured as categories that depend on and influence each other. Linking activities can also be impacted by the presence of various influencing factors, acting as barriers or facilitators. This relationship is illustrated in Figure 2.
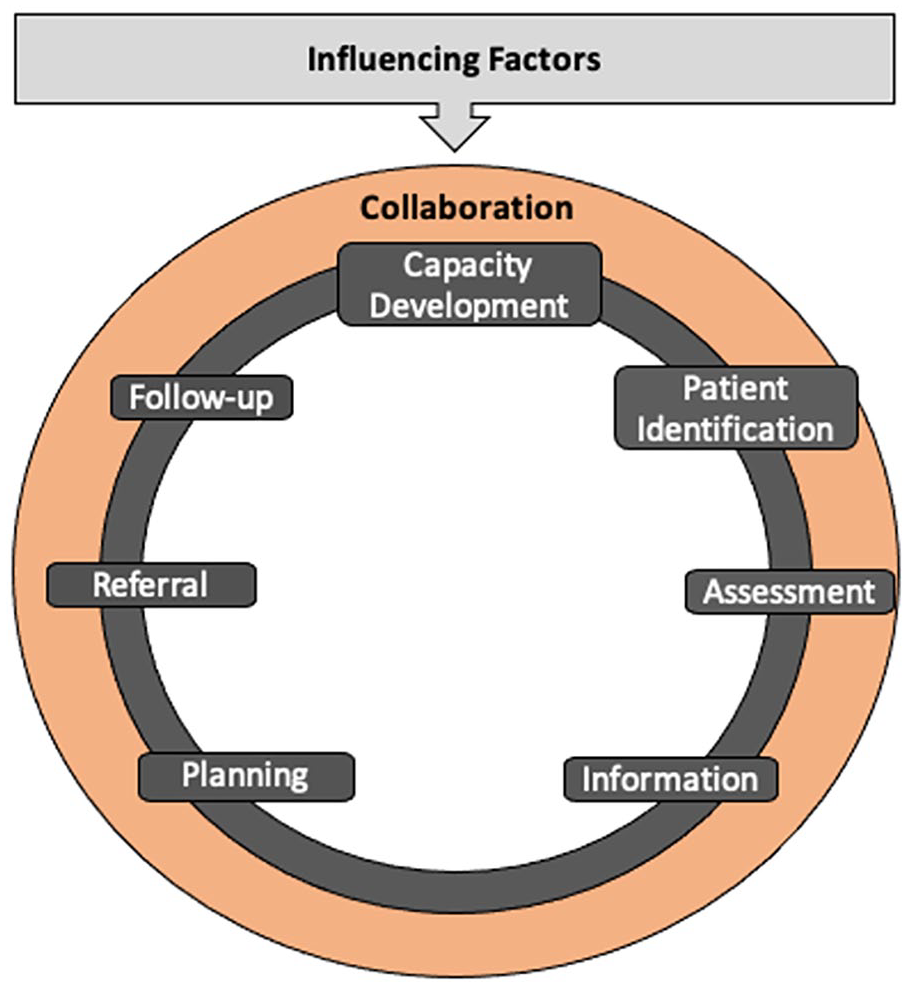
Figure presenting primary healthcare providers’ activities in linking patients with chronic diseases to community organizations.
Influencing Factors
Multiple intrinsic and extrinsic factors were listed in the studies as influencing linking activities. These factors can stem from personal characteristics of the providers and patients, providers’ professional practice, work environments, partnerships, and contextual influences. They may have a positive or negative impact on the practice of these linking activities, depending on whether they can be adapted to local circumstances. Table 3 lists examples of factors for each category.
Summary of Factors Influencing Linking Activities.

Discussion
To our knowledge, this study presents a first literature synthesis detailing linking activities practiced by primary healthcare providers with COs in a CD management context, and their influencing factors.
Adapting Interprofessional Collaboration
Beyond the linking activities of each provider, interprofessional collaboration allows to extend beyond the scope of the primary healthcare provider’s expertise to provide more comprehensive linking activities. This interdisciplinary approach aligns with the positive impacts that collaboration in primary care settings can have on patients’ well-being and clinical outcomes in a CD management context.51 -54 During the consultation phase, experts highlighted that the complexity associated with the patient’s needs and care management influences the level of interprofessional collaboration required. Thus, for each category of linking activities, barriers may arise as the complexity of the clinical situation increases, requiring more interprofessional concertation to ensure an effective implementation of activities. Although linking activities were generally similar across studies, the level of detail, operationalization, and which healthcare provider practiced which activity varied and was not always explicit. This understanding would be useful for better organizing linking activities from a teamwork perspective.
Prioritizing Local Influencing Factors
Significant variability was also observed in influencing factors. The diverse needs of patients and the preferences of healthcare providers can influence linking activities. 50 The consulted experts proposed that the local context is directly linked to these influencing factors. Leach et al 55 noted that several factors can act as facilitators or barriers in an interdisciplinary context. However, factors internal to the practice can often become facilitators since they can be more easily managed than external contextual factors. Therefore, it might be relevant for primary healthcare providers and managers to first focus on managing influencing factors that are specific to their local practices.
Strengths and Limitations
The study was conducted rigorously, following the 6 steps of the scoping review methodology including the consultation step, which enriched the synthesis. Despite the strengths of this study, some limitations should be considered. Firstly, only articles accessible in the selected databases and languages were consulted, with no search conducted in gray literature. Finally, the description of linking activities and influencing factors is based on the information presented in the selected studies. Some concise or absent information may have affected our interpretation.
Future Research
Future studies on primary care linking activities between PCDs and COs should explicitly describe interventions and the role of each provider, as well as explore solutions to overcome barriers in practice. Additionally, gaining a better understanding of the phenomenon from the perspective of COs would allow a better understanding of the current issues and their expectations for this intersectoral collaboration.
Conclusion
The description of primary care providers’ linking activities between PCDs and COs shows an holistic practice that includes patients in the decision making process and that can potentially overcome chronic care complexity by fostering collaboration and constant involvement of all actors at the primary care and community levels. While expected involvement from each primary care provider and strategies to address barriers could be more detailed to facilitate liaison, practices and governments should also be more involved to support collaboration between various providers and adapt policies to local circumstances.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241257374 – Supplemental material for Primary Healthcare Providers’ Activities in Linking Patients With Chronic Diseases to Community Organizations: A Scoping Review
Supplemental material, sj-docx-1-jpc-10.1177_21501319241257374 for Primary Healthcare Providers’ Activities in Linking Patients With Chronic Diseases to Community Organizations: A Scoping Review by Nevena Grgurevic, Maud-Christine Chouinard, Édith Ellefsen, Émilie Hudon and Catherine Hudon in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We thank the Université de Sherbrooke’s Library and Archive Department for its help in developing the search strategy and Bonita Van Doorn for the editorial revision. A special thank you also to the V1SAGES research team members and colleagues for their input during the consultation exercise.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author was financially supported through her master scholarship by the Institut universitaire de première ligne en santé et services sociaux (IUPLSSS), Ministère de l’Éducation et Ministère de l’Enseignement supérieur (MEES), Université de Sherbrooke, and Ordre des infirmières et infirmiers du Québec (OIIQ). The views expressed in this article do not necessarily represent the views of the IUPLSSS, MEES, Université de Sherbrooke or OIIQ.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.