
Abstract
Objectives:
The prevalences of hypertension and depression in sub-Saharan Africa are substantial and rising, despite limited data on their sociodemographic and behavioral risk factors and their interactions. We undertook a cross-sectional study in 4 communities in the Upper East Region of Ghana to identify persons with hypertension and depression in the setting of a pilot intervention training local nurses and health volunteers to manage these conditions.
Methods:
We quantified hypertension and depression prevalence across key sociodemographic factors (age, sex, occupation, education, religion, ethnicity, and community) and behavioral factors (tobacco use, alcohol use, and physical activity) and tested for association by multivariable logistic regression.
Results:
Hypertension prevalence was higher in older persons (7.6% among 35- to 50-year-olds vs 16.4% among 51- to 70-year-olds) and among those reporting alcohol use (18.9% vs 8.5% between users and nonusers). In multivariable models, only older age (AOR 2.39 [1.02, 5.85]) and residence in the community of Wuru (AOR 7.60 [1.81, 32.96]) were independently associated with hypertension, and residence in Wuru (AOR 23.58 [7.75-78.25]) or Navio (AOR 7.41 [2.30-24.74]) was the only factor independently associated with depression.
Conclusions:
We report a high prevalence of both diseases overall and in select communities, a trend that requires further research to inform targeted chronic disease interventions.
Introduction
Non-communicable diseases (NCDs), which primarily include cardiovascular disease, cancer, diabetes, and chronic respiratory diseases, constitute a significant and increasing proportion of morbidity and mortality worldwide.1,2 This disease burden is especially marked in low- and middle-income countries, where 86% of the premature mortality from NCDs occurs. 2 In sub-Saharan Africa (SSA), disability-adjusted life-years due to NCDs have increased by 67.0% over the last 3 decades. 3 Hypertension is a major risk factor for most NCDs, and it is associated with more deaths globally (~10.8 million) than any other cause. 4 While hypertension was previously most impactful in high-income countries, the trend has now reversed, with low- and middle-income countries experiencing both greater hypertension prevalence and worse disease outcomes than high-income ones.5,6 The reasons for this shift include urbanization, increased energy-dense and processed diets, and decreased physical activity.2,7,8
In SSA, estimates for the prevalence of hypertension range from 13.5% in Eritrea to greater than 30% in Tanzania, Central African Republic, and Sudan. 9 If pre-hypertension (or Stage I hypertension) is included as well, the prevalence is greater than 50% for most countries in SSA. 9 Despite high hypertension prevalence, levels of disease awareness, treatment, and control are poor. Among individuals with hypertension in SSA, blood pressure control is 4% to 17%. 9 In Ghana, estimated hypertension prevalence is 27.0%, with only 35.0% aware of their diagnosis, 22.0% receiving anti-hypertensive treatment, and 6.0% achieving blood pressure control. 10 Healthcare systems in Ghana are not adequately equipped to address hypertension and, in general, NCDs. 11
Global action plans for NCD control, such as the World Health Organization’s Package of Essential NCD Disease Interventions, have usually focused the 4 main NCDs above. 12 However, a growing list of advocates have demanded including mental health disorders within the global NCD agenda.13,14 The absolute global disease burden and the proportion of global disease attributable to mental disorders have risen significantly since 1990. 15 Although accurate measurement of mental health burden in SSA is difficult, depression prevalence is high and rising. 15 The most recent estimates suggest 4% of persons in Ghana are affected, though select studies have reported prevalence as high as 25.2% with very few under treatment.16-18
Moreover, increasing evidence demonstrates that living with NCDs is associated with depression and other mental illness and that mental illness exacerbates and is exacerbated by NCDs in turn. For example, hypertension and depression share similar risk factors, such as alcohol misuse, social stressors, and sedentary behavior, all of which can exacerbate both cardiovascular and mental disorders in the same individual.19,20 Additionally, the progression of hypertension and depression can influence each other by direct physiological means, such as cytokines and hormonal factors, though these remain incompletely understood. 19 In SSA, and specifically in Ghana, hypertension correlates with depression.21-23 However, the interactions between these 2 conditions are complex and differ across sociodemographic groups. For example, among women in Ghana, hypertension is more prevalent among those with depression than those without. However, among men, hypertension correlates with reported negative life events but not with depression. 24 Thus, targeted intervention on these common conditions requires further study of their risk factors—both individually and jointly—in the undertreated communities of rural SSA.
In this study, we utilize data collected during the screening process for a pilot intervention in 4 rural communities in northern Ghana, which sought to provide counseling and treatment for hypertension and depression at community-level healthcare facilities. Specifically, we analyze the distribution of hypertension and depression prevalence across sociodemographic and behavioral factors and evaluate the factors associated with both conditions using hierarchical models.
Methods
Parent Study
This study was an analysis of data collected by the Community-Based Health Planning and Service (CHPS) Opportunity for Mentally and Behaviorally Integrated NCD Engagement (COMBINE) study, which seeks to evaluate the effectiveness of community health nurses and volunteers in delivering hypertension and depression care in the 4 rural communities of Mirigu, Wuru, Navio, and Yua in northern Ghana. Community health nurses, referred to as community health officers in the Ghana health system, screened individuals in their respective catchment areas for inclusion in the COMBINE study from April to November 2021. This study utilized study screening and enrollment data from these 4 communities.
During the screening, community health officers conducted household visits and screened all present individuals in each household between 35 and 70 years old. The study also captured demographic information including age, sex, occupation, education level, religion, ethnicity, and community location. Behavioral information, including tobacco use, alcohol use, and physical activity, was collected as well. To screen for depression, we administered the Patient Health Questionnaire (PHQ), which has been validated across multiple settings. All individuals answered the 2 question screen (PHQ-2). 25 Those with a PHQ-2 score of 1 or more then completed a 9-question follow-up screen (PHQ-9). 26 To screen for hypertension, we measured blood pressure using an electronic apparatus (Omron, Kyoto, Japan) which was calibrated by the Ghana Standards Authority. All individuals had 1 household blood pressure measurement; those with a first measurement greater than or equal to 140 mm Hg systolic or 90 mm Hg diastolic had 2 additional measurements during that visit. If the average of 3 measurements during the household visit was greater than or equal to 140 mmHg systolic or 90 mmHg diastolic, then individuals were asked to visit the CHPS primary health clinic within 2 days, where they had 2 additional confirmatory blood pressure measurements to ascertain hypertension.
Outcome Variables
The 2 primary outcomes analyzed in this study were hypertension and depression. Individuals were classified as having hypertension if (1) their blood pressure (average of 3 measurements) on both the household and clinic visits was greater than or equal to 140 mm Hg systolic or 90 mmHg diastolic or (2) their average blood pressure at either visit was greater than or equal to 180 mm Hg systolic or 100 mm Hg diastolic, which warranted immediate referral to a higher-level facility for care. Individuals were classified as having depression if their PHQ-9 score was greater than or equal to 5, the diagnostic threshold for mild depression or greater. 26 Notably, the COMBINE study enrolled only persons with a PHQ-9 score of 10 to 19 (moderate to severe depression) and referred persons with PHQ-9 score of 20 or more or suicidality on PHQ-9 screen to a higher-level facility for care.
We also captured data on pre-hypertension (also called Stage 1 hypertension), defined as a blood pressure of 130 to 139 mm Hg systolic or 80 to 89 mm Hg diastolic. 27 Although the nurse screening protocol for this study only instructed second and third blood pressure measurements if the first blood pressure was greater than or equal to 140 mm Hg systolic or 90 mm Hg diastolic, we classified participants as pre-hypertensive if they were not classified as hypertensive and (1) their average blood pressure on either the household or clinic visits was 130 to 139 mm Hg systolic or 80 to 89 mmHg diastolic, or (2) their first blood pressure measurement during the household visit was 130 to 139 mm Hg systolic or 80 to 89 mm Hg diastolic.
Explanatory Variables
Explanatory variables included sociodemographic and behavioral risk factors. The sociodemographic factors include age, sex, occupation, education level, religion, ethnicity, and community of residence (among the 4 aforementioned communities). Behavioral risk factors included tobacco use (defined as present if any use of tobacco or its products within 12 months prior to screening), alcohol use (defined as present if any intake of alcoholic beverages over the past 12 months), and physical activity (defined as greater than or equal 30 min of moderate-to-vigorous physical activity per day). Dietary pattern was not included as one of the behavioral risk factors since we did not have an appropriate instrument that was sufficiently validated for the setting in order to capture diet.
Analysis
We calculated and compared the prevalence of the outcome variables across each sociodemographic and behavioral factor using Chi-squared or Fisher exact tests, as appropriate. We then used 4 hierarchical multivariable logistic regression models to analyze the association of sociodemographic and behavioral factors with hypertension and depression. (The reference for variables of religion and community were set to the group with the lowest hypertension prevalence.) For each outcome, model 1 adjusted only for age and sex, model 2 adjusted all sociodemographic factors, model 3 adjusted for all sociodemographic and behavioral factors, and model 4 was adjusted for all sociodemographic and behavioral risk factors as well as hypertension (when depression was the outcome) or depression (where hypertension was the outcome). We defined statistical significance for associated variables at a 2-tailed P < .05. To avoid collinearity, variables with a variable inflation factor greater than 10 were not included in the final models. We compared the relative fit of the hierarchical models using Akaike’s information criterion (AIC) and pseudo-R squared. Models with a lower AIC had a better fit, and pseudo-R was used to define the proportion of variance explained by the model. All statistical analyses were carried out in R version 4.2.2.
Ethical Approval and Funding
The COMBINE study received institutional review board (IRB) approval from both the Mount Sinai IRB (21-01138) and the Navrongo Health Research Centre IRB. We obtained informed consent from all participants as per these approvals. Funding for this study was from Resolve to Save Lives, Teva Pharmaceutical Industries, and National Institutes of Health/Fogarty International Center (R21TW010452).
Results
Sample Distribution
We analyzed all data collected from individuals 35 to 70 years old whose data was complete (n = 342). Over one-half of the study sample was between the ages of 35 and 50 years old (55.8%; Table 1). The majority of individuals screened were female (74.3%), farmers (81.6%), Christian (63.5%), from the Nankani ethnic group (69.3%), and had received no formal education (62.6%). Across the 4 communities, Mirigu and Yua comprised a larger proportion of the sample than did Navio and Wuru. In terms of behavioral factors, most individuals reported no tobacco use (95.0%) or alcohol use (71.3%). Approximately one-half of those screened reported physical activity greater than or equal to 30 min per day (48.8%).
Distribution of Sociodemographic and Behavioral Factors Among Individuals Screened.

Sample size too small to include in further analyses.
Hypertension
The overall prevalence of hypertension across the 4 communities was 11.4% [7.9%-14.9%] (Table 2). The prevalence of hypertension did not differ across the 4 communities (P = .18) involved in this study. The prevalence of hypertension was higher among individuals who were older: 7.6% [3.7%-11.4%] among 35- to 50-year-olds versus 16.4% [10.2%-22.6%] among 51- to 70-year-olds (P = .02). However, hypertension prevalence did not differ significantly across sex, occupation, education, religion, or ethnicity. When comparing across behavioral factors, hypertension differed based on alcohol use: 18.9% [10.6%-27.1%] among those with alcohol use versus 8.5% [4.9%-12.1%] among those without any alcohol use (P = .01). There was no observed difference according to tobacco use or physical activity.
Prevalence of Hypertension and Depression Across Sociodemographic and Behavioral Factors.
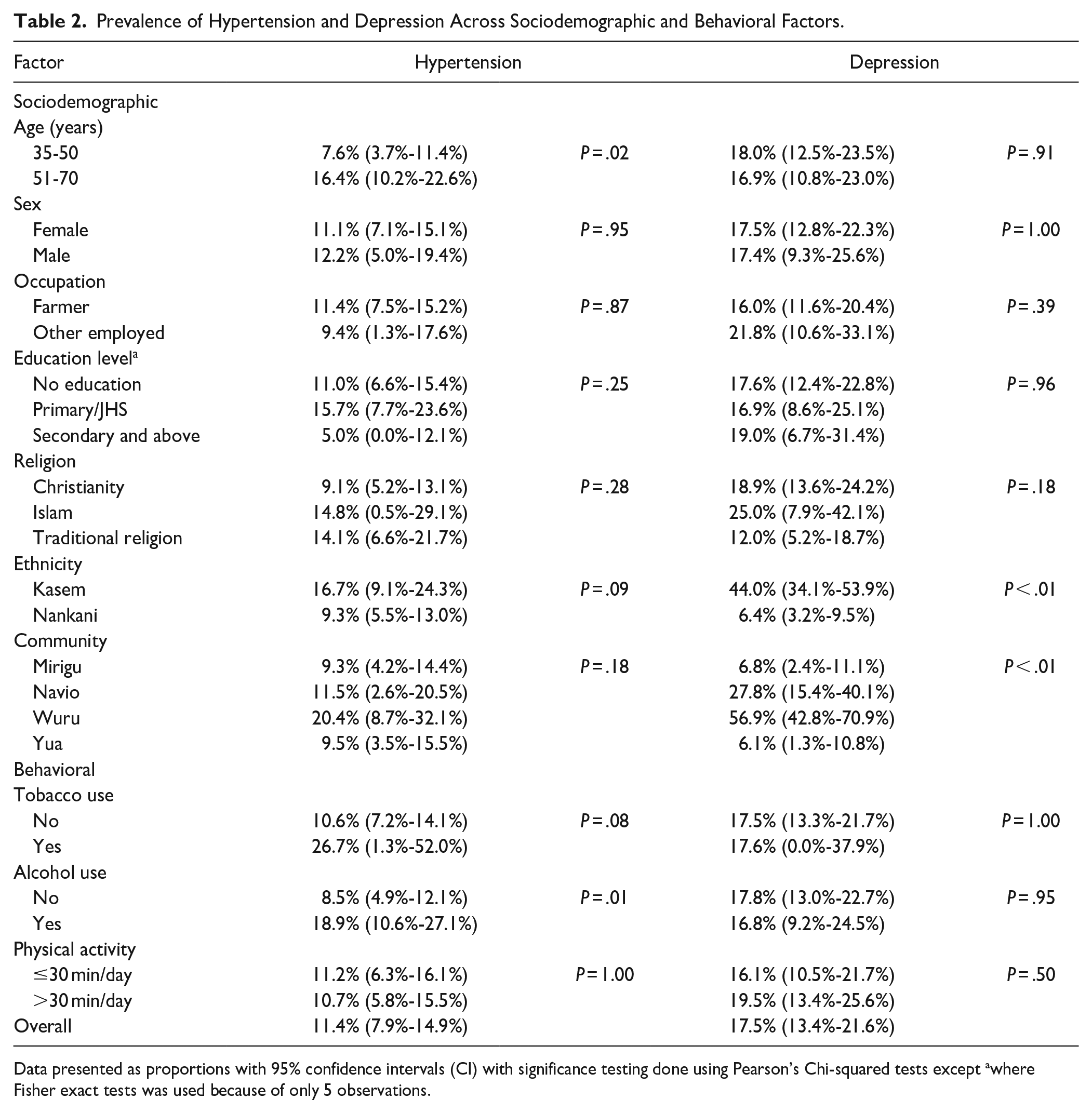
Data presented as proportions with 95% confidence intervals (CI) with significance testing done using Pearson’s Chi-squared tests except awhere Fisher exact tests was used because of only 5 observations.
When considering individuals only with pre-hypertension, the overall prevalence of pre-hypertension was 23.1% [18.5%-27.7%], with the prevalence higher among older individuals. (Supplemental Table 1). Additionally, individuals of Nankani ethnicity had higher prevalence of pre-hypertension than those of Kasem ethnicity, and Yua had the highest pre-hypertension prevalence of all 4 communities.
In a multivariable logistic model adjusted only for age and sex (model 1), individuals 51 to 70 years old had higher odds of hypertension than those 35 to 50 years old (odds ratio, OR 2.40 [1.19, 4.97] (Figure 1). After adjusting for other sociodemographic factors as well (model 2), age remained significantly associated with hypertension in addition to residence in Wuru compared to Mirigu (adjusted odds ratio, AOR 4.48 [1.56, 13.24]). This community effect was not explained by behavioral factors (model 3). In the final model, adjusted for all sociodemographic and behavioral factors as well as depression (model 4), older individuals (AOR 2.39 [1.02, 5.85]) and those living in Wuru (AOR 7.60 [1.81, 32.96]) had significantly higher odds of hypertension compared to younger individuals and those living in Mirigu, respectively. Presence of depression was not associated with a statistically significant higher odds of hypertension (AOR 1.21 [0.39, 3.57]). AIC for model 4 was lower than that for models 1, 2, and 3, suggesting a better fit model when including sociodemographic and behavioral factors as well as depression as model predictors. The variance (pseudo-R squared) explained by model 4 was 12% compared to 3% for model 1, 9% for model 2 and 11% for model 3.

Results of hierarchical logistic regression models showing association of sociodemographic and behavioral risk factors with hypertension. Model 1 = age + sex; Model 2 = Model 1 + other sociodemographic factors; Model 3 = Model 2 + behavioral factors (tobacco, alcohol, and physical activity); Model 4 = Model 3 + depression. Ethnicity not included as covariate due to high collinearity with community (VIF > 10). Results reported as odds ratio (95% confidence interval).
Depression
The overall prevalence of depression across the 4 communities was 17.5% [13.4%-21.6%] (Table 2). However, across the 4 different communities, depression prevalence varied (P < .01), with the communities of Navio (27.8% [CI 15.4%-40.1%]) and Wuru (56.9% [CI 42.8%-70.9%]) having the highest prevalence. Similarly, depression prevalence differed between ethnicities: 44.0% [34.1%-53.9%] among Kasem versus 6.4% [3.2%-9.5%] among Nankani ethnic groups (P < .01). Depression prevalence did not significantly vary across age, sex, occupation, education, or any of the behavioral explanatory variables.
In a multivariable logistic regression model, adjusting for age, sex, and other sociodemographic variables (model 2), the odds of having depression were significantly higher in Wuru and Navio compared to Mirigu. Compared to Mirigu, individuals in Navio had 5 times higher odds of depression (AOR 4.75 [1.86-12.68]), while individuals in Wuru had almost 17 times higher odds of depression (AOR 16.95 [6.92-45.17]; Figure 2). Adjusting additionally for behavioral variables (model 3) and hypertension (model 4) further increased the association between community and depression (AOR 7.41 [2.30-24.74] in Navio and AOR 23.58 [7.75-78.25] in Wuru relative to Mirigu). When adjusted for sociodemographic and behavioral factors and hypertension (model 4), the odds of depression for individuals were 3 times greater among persons identifying as Muslim than in the reference group (AOR 3.41 [0.93, 12.29] compared to those identifying as Christian), though this difference was not statistically significant. Hypertension status was not significantly associated with odds of depression (AOR 1.23 [0.40, 3.57]). AIC for model 4 was lower than that for models 1, 2, and 3, suggesting a better fit model when including sociodemographic and behavioral factors as well as hypertension as model predictors. The variance (pseudo-R squared) explained by model 4 was 25% compared to 0% for model 1, 23% for model 2 and 23% for model 3.
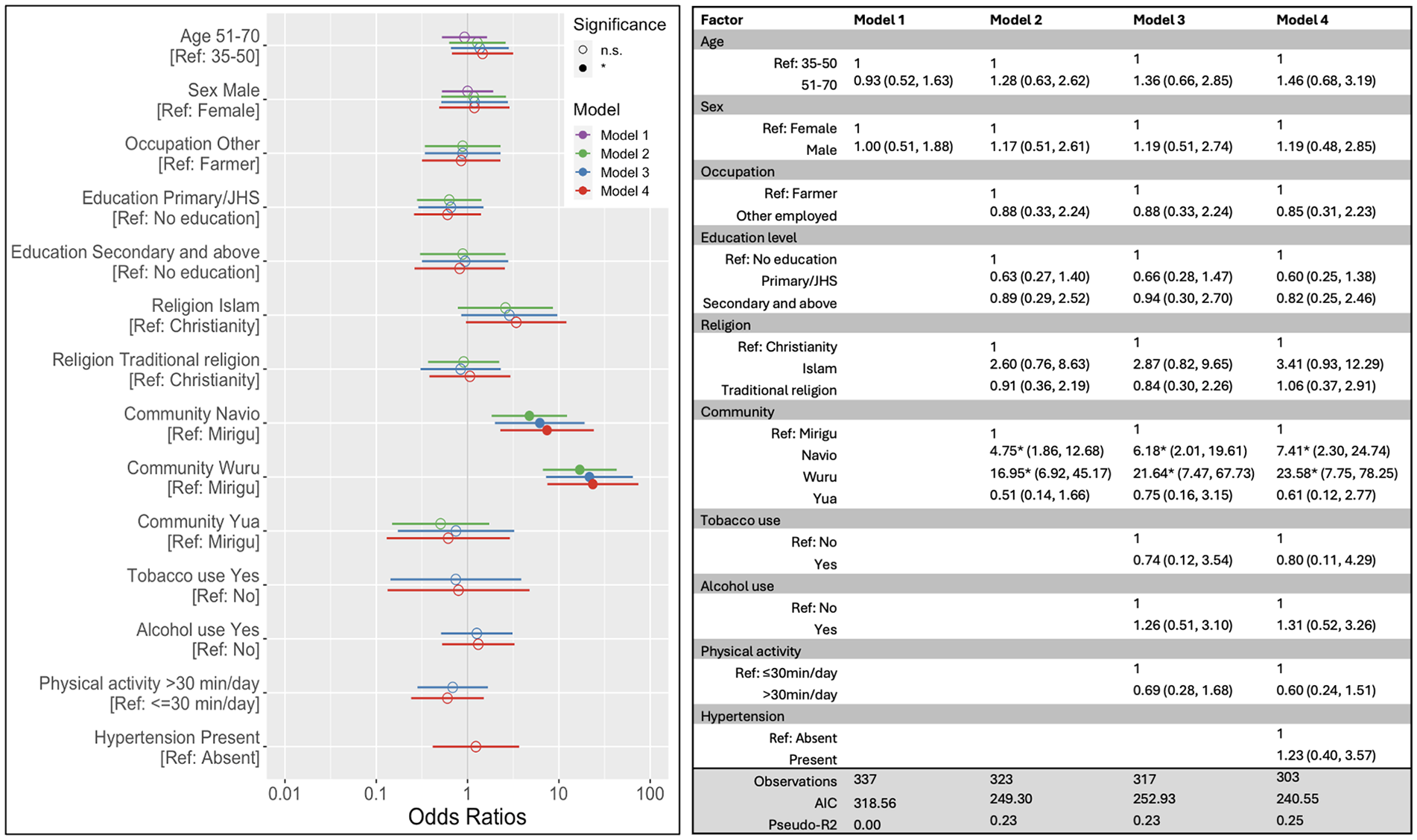
Results of hierarchical logistic regression models showing association of sociodemographic and behavioral risk factors with depression. Model 1 = age + sex; Model 2 = Model 1 + other sociodemographic factors; Model 3 = Model 2 + behavioral factors (tobacco, alcohol, and physical activity); Model 4 = Model 3 + hypertension. Ethnicity not included as covariate due to high collinearity with community (VIF > 10). Results reported as odds ratio (95% confidence interval).
Discussion
Our analysis revealed notable trends in the distribution of hypertension and depression prevalence across sociodemographic and behavioral factors in 4 rural communities in northern Ghana. Specifically, we estimated hypertension prevalence to be 11.4%, which was lower than the pooled prevalence of hypertension from previous studies in Ghana (27%) but consistent with the estimate of previous studies limited to the northern part of the country (13%). 10 We also found that hypertension prevalence was higher among older individuals and those who reported alcohol use. However, multivariable associations adjusting for multiple sociodemographic and behavioral variables found that the age was the only one of those factors independently associated with odds of hypertension. This association of hypertension with age and the lack of an association between hypertension and sex align with previous analyses in Ghana.28,29 While previous analyses reported an association of hypertension with socioeconomic status, we did not find hypertension to be correlated with occupation, which was the measure of socioeconomic status used in our study. 29 However, this could be due to the presence of influential socioeconomic factors outside occupation or the relatively limited variation in socioeconomic status among individuals in the 4 rural communities in this study. Alternatively, the lack of association between hypertension prevalence and socioeconomic status in this analysis may show that hypertension affects all socioeconomic strata in Ghana given the increasing prevalence of NCDs even among individuals of the lowest socioeconomic status. 30
In addition to age, residence in the community of Wuru was the only other variable found to be associated with higher odds of hypertension, and this relationship remained even after adjusting for behavioral variables including alcohol use, tobacco use, and physical activity. We hypothesize multiple possible reasons for the seemingly high concentration of hypertension in this community. While Wuru is still a rural community, it was the closest out of the 4 to the peri-urban centers of Navrongo and Paga. Given the increased prevalence of hypertension reported in urban versus rural areas in Ghana, this proximity to the urban center could contribute to the increased hypertension in Wuru through mechanisms outside of the 3 aforementioned behavioral factors.8,31 Specifically, differences in dietary environment between communities could influence NCD prevalence, as Wuru includes more fast food eateries which serve indomie and other processed, energy-dense foods. Other mediating factors could include environmental pollutants, which have been shown to increase hypertension. 32 Further research is needed to identify how to address the relatively large hypertension burden in the community of Wuru.
Separately from hypertension, there was double the prevalence of pre-hypertension in the 4 communities, with the highest prevalence in a community (Yua) that did not have the highest prevalence of hypertension. This may predict a future surge of hypertension in Yua in the absence of any intervention. Given that pre-hypertension is more amenable to behavioral changes than hypertension, this may suggest an optimal window of opportunity to target individual- and community-level counseling to prevent the progression to a high hypertension burden in Yua. 33 However, regardless of the relatively higher concentration of pre-hypertension and hypertension in some communities, hypertension care throughout Ghana is very limited—with only 35% of those with hypertension being aware, 22% on treatment, and 6% with blood pressure control. 10 Therefore, a comprehensive approach that offers both behavioral and pharmacological interventions for hypertension needs to be integrated into the healthcare system.
Meanwhile, we estimated 17.5% prevalence of depression in the 4 communities. Epidemiological data on mood disorders in SSA is very limited, but the most recent estimate for depression prevalence in Ghana nationally is 4.2%. 18 Prevalence as high as 25% has been reported in certain communities in Ghana, suggesting high variability across regions. 17 Previous studies have also reported more prevalent depression among women, in contrast with findings of our analysis.16,17 This difference may also be dependent on the region as gender roles can generally differ based on the social and economic context of the community. Notably, we also did not find an association between depression and behavioral factors, such as alcohol use, which aligns with the findings of a large cross-sectional study in the Volta region of Ghana. 17 It may be possible that the the threshold of alcohol use (any alcohol intake in last 12 months in our study and any current alcohol use in aforementioned study) does not capture the association between alcohol use and depression which may be present only at higher levels of alcohol use. However, another cross-sectional analysis of the WHO SAGE study of individuals in Ghana over 50 years old also did not find any association between higher levels of alcohol use and depression after adjusting for other socio-demographic factors. 34 While this lack of association seemingly contradicts previous literature highlighting the overlap of alcohol use and depression, the lack of association may be a result of the older age distribution of this sample and the WHO study. 35 Moderate alcohol drinking is not associated with depression risk in older adults. 36 Nevertheless, the link between behavioral factors, including alcohol use, and depression requires further study that more precisely quantifies drinking patterns and type of alcohol.
The only factor that was found to be independently associated with depression in multivariable analyses was residence in the community of Wuru or Navio. Wuru and Navio are closer to peri-urban centers than Mirigu and Yua. Therefore, analogous to the trend of hypertension, it is possible that residence in these 2 communities is associated with higher prevalence of depression due to lifestyle factors associated with proximity to an urban center. However, a previous analysis did not find a difference in depression prevalence between urban and rural settings among individuals over 50 years of age across Ghana. 16 A meta-analysis of previous literature found higher odds of depression in urban settings in developed countries; however, there was no clear difference between odds of depression comparing urban and rural settings in developing countries, with different studies reporting opposing findings. 37 This evidence suggests that the urban-rural distribution of depression is likely variable based on context. It is still possible that factors specific to the Upper East region in Ghana contribute to increased depression prevalence among communities closer to urban centers. More research is urgently needed to address community level stressors that may be acting on this specific population.
Finally, we did not find a significant interaction between hypertension and depression. In multivariable analyses, depression was not an independent predictor of hypertension, and hypertension was not an independent predictor of depression. Some previous analyses in Ghana have shown such an interaction, including 1 study from the Ashanti region which found that hypertension was more likely among women with depression than those without. 24 The interaction of these 2 conditions is very likely given that both share similar behavioral and structural drivers.19,20 Therefore, interventions that target those shared drivers are likely to help address the burden of both conditions.
Strengths and Limitations
This analysis is one of few studies that analyzes hypertension and depression in this region of Ghana. Additionally, participants were surveyed regarding a comprehensive set of sociodemographic and behavioral variables, allowing characterization of the distribution of these chronic conditions across multiple factors. We defined and measured hypertension and depression using globally validated guidelines and repeated blood pressure measurements to improve the specificity of diagnosis. Further, we conducted multivariate analyses adjusting for each of these factors, including analyses of variance. However, this analysis was a secondary analysis of cross-sectional data collected during the screening process for a pilot intervention to treat hypertension and depression. Further, the study was not designed with statistical power to detect a difference between 2 or more groups (eg, depression among those with and without hypertension) of any given size and, therefore, may have failed to find a true correlation in these cases. This study also did not capture data on dietary patterns, which can significantly affect hypertension, given that we did not have an instrument that was sufficiently validated for the setting to capture this variable. Additionally, some communities comprise a larger proportion of the sample based on their fulfillment of enrollment targets. Lastly, our study approach may have limited our accuracy in detecting all cases of disease. For example, the requirement for 2 different averages of blood pressure readings to both be elevated on separate days may have falsely excluded some cases of hypertension; conversely, failure to further screen persons with 1 blood pressure reading in the pre-hypertension range may have falsely raised the prevalence of pre-hypertension. Regardless, our analysis provides an initial characterization of the distribution and risk factors for these 2 conditions in an area with limited data to guide interventions and reports novel findings with respect to location and other socio-demographic factors as potential risk factors for these 2 common diseases. Ultimately, these findings can offer insights into how best to target new interventions to address the growing prevalence of hypertension and depression in this setting.
Conclusion
Overall, we characterize the distribution of hypertension and depression, most notably finding the concentration of both conditions in specific communities irrespective of various sociodemographic and behavioral factors. Further research is needed to confirm this trend, and a comprehensive program providing behavioral and pharmacological interventions needs to be implemented into the healthcare system.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241242965 – Supplemental material for Sociodemographic and Behavioral Factors Associated With Hypertension and Depression in 4 Rural Communities in Northern Ghana: A Cross-Sectional Study
Supplemental material, sj-docx-1-jpc-10.1177_21501319241242965 for Sociodemographic and Behavioral Factors Associated With Hypertension and Depression in 4 Rural Communities in Northern Ghana: A Cross-Sectional Study by Masih A. Babagoli, Dorothy Adu-Amankwah, Engelbert A. Nonterah, Raymond A. Aborigo, Irene Kuwolamo, Khadija R. Jones, Evan E. Alvarez, Carol R. Horowitz, Benedict Weobong and David J. Heller in Journal of Primary Care & Community Health
Footnotes
Author Contributions
MAB, DA, DJH, and RAA led the conceptualization of the study design and manuscript. EAN, RAA, and IK led the acquisition of the data. KRJ, CRH, and BW contributed to study design and analysis. MAB and DA led the analysis, interpretation and writing of the manuscript. Critical reviews and edits of the manuscript were led by DJH, EA, and KRJ. All authors approved of the manuscript content.
Data,Material,and Code Availability
De-identified data underlying this manuscript for reproduction of findings is available upon request to the corresponding author.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DJH reports support from Hess Corporation, who was not involved in any way in the creation of this manuscript or the conduct of this research, as a potential competing interest. DJH and RAA report funding from Teva Pharmaceutical Industries, who funded this research but were not involved in any way in the creation of this manuscript or the conduct of this research. No other author has any potential conflict to state or disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge funding from Resolve to Save Lives, Teva Pharmaceutical Industries, and National Institutes of Health/Fogarty International Center (R21TW010452) and research support from the Arnhold Institute for Global Health and the Navrongo Health Research Centre. We also thank all research participants for their time and engagement.
Ethical Approval and Informed Consent
The COMBINE study received institutional review board (IRB) approval from both the Mount Sinai IRB (21-01138) and the Navrongo Health Research Centre IRB, as detailed above. Informed consent forms for participation, as approved by both IRBs, are available upon request to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.