
Abstract
Background:
Carpal Tunnel Syndrome (CTS) is associated with a significant personal and societal burden. Evaluating access to care can identify barriers, limitations, and disparities in the delivery of healthcare services in this population. The purpose of this study was to evaluate access to overall healthcare and healthcare utilization among patients with CTS.
Methods:
This is a retrospective cohort study conducted with the All of Us database. Patients diagnosed with CTS that completed the access to care survey were included and matched to a control group. The primary outcomes were access to care across 4 domains: (1) delayed care, (2) could not afford care, (3) skipped medications, and (4) over 1 year since seeing provider. Secondary analysis was then performed to identify patient-specific factors associated with reduced access to care.
Results:
In total, 7649 patients with CTS were included and control matched to 7649 patients without CTS. In the CTS group, 33.7% (n = 2577) had delayed care, 30.4% (n = 2323) could not afford care, 15.4% (n = 1180) skipped medications, and 1.6% (n = 123) had not seen a provider in more than 1 year. Within the CTS cohort, low-income, worse physical health, and worse mental health were associated with poor access to care.
Conclusion:
Patients experience notable challenges with delayed care, affordability of care, and medication adherence regardless of having a diagnosis of CTS. Targeted interventions on modifiable risk factors such as low income, poor mental health, and poor physical health are important opportunities to improve access to care in this population.
Introduction
Carpal tunnel syndrome (CTS) is a common nerve entrapment syndrome caused by compression of the median nerve with treatment options ranging from nonoperative splinting, physical therapy, and corticosteroid injections to surgical decompression via carpal tunnel release.1,2 Prevalence of CTS ranges anywhere between 3% and 8%.3 -5 Patients often report worse physical function and increased pain, contributing to decreased work productivity and associated economic costs exceeding $2 billion in the United States alone.6 -8 Patient-specific social factors such as race, ethnicity, occupation, and socioeconomic status have been associated with both the epidemiology of CTS and worse functional and mental health outcomes of patients with CTS.9 -11 Patients of female sex, non-white race, Hispanic ethnicity, non-private insurance status, or higher social deprivation have been found to be less likely to receive surgical treatment with carpal tunnel release.12,13 The role of social factors extends to the postoperative period, as socioeconomic deprivation has also been implicated with persistent physical symptoms and decreased functional status compared to patients of higher socioeconomic status following carpal tunnel release (CTR). 14
Considering the high prevalence, disabling symptomatology, and societal economic burden of CTS, an analysis of access to care in a cohort of CTS patients can identify barriers, limitations, and disparities in the delivery of healthcare services.6,15 There is currently little data on the association of CTS and patient-specific factors with access to care. The purpose of this study was to therefore assess the association of CTS and patient-specific factors with decreased access to overall healthcare and healthcare utilization among patients with CTS.
Materials and Methods
We conducted a retrospective review of the All of Us database from May 2018 to May 2023. This is a United States database run by the National Institutes of Health (Bethesda, Maryland, United States of America) launched in 2018 that is a large, diverse, broadly accessible dataset for advancing precision medicine research and insights into human health. The All of Us database preferentially recruits underrepresented populations in medicine such as Black or African American patients and LGBTQ+ patients and collects data including genomic variants, patient-reported outcome measure responses, and clinical health information including disease states and demographic information from the electronic health record.
Our experimental cohort encompassed all patients diagnosed with CTS that completed the “Healthcare Access and Utilization Survey” survey within the All of Us database. This survey derived questions from the National Health Interview Survey (NHIS), a validated patient reported outcome measure (PROM) that collects data on socioeconomic characteristics and health topics such as conditions, medications, and access to medical care. Any participant of the All of Us research program in the United States is able to complete this survey. Diagnosis of CTS was identified using Systematized Nomenclature of Medicine (SNOMED) clinical term 57406009 (Carpal tunnel syndrome). A control cohort of patients without a diagnosis of CTS was matched to the CTS cohort using a one-to-one ratio based on age, sex, race, PROMIS Global-10 physical health scores, and PROMIS Global-10 mental health scores. Patients with CTS who received operative treatment with CTR were identified using Current Procedural Terminology (CPT) codes 29848 and 64721.
Outcome Measures
The primary outcome was the patients’ self-reported ability to access healthcare based on survey results from the publicly accessible “Healthcare Access and Utilization Survey” of the All of Us database (Researchallufus.org). The domains of “delayed care,” “could not afford care,” and “skipped medications” represent an aggregate of multiple sub-survey questions coded by our research team. If “yes” was answered for any of the sub-questions, we created a classification of 4 domains: (1) delayed care, (2) could not afford care, (3) skipped medications, and (4) over 1 year since seeing provider. The survey questions for all 4 outcomes assessed the patient’s access to care and healthcare utilization within the past 12 months from the time the patient completed the survey. As an example, the “could not afford care” domain referred to the following question: “During the past 12 months, was there any time when you needed any of the following, but didn’t get it because you couldn’t afford it?”. The corresponding sub-survey question options were “prescription medicines, mental health care or counseling, emergency care, dental care, eyeglasses, to see a regular doctor or general health care provider, to see a specialist, follow-up care,” to which patients could respond “yes,” “no,” or “don’t know.” The corresponding survey questions are all publically available online. We then utilized these domains to compare the CTS and control cohorts to evaluate the correlation of CTS diagnosis with these healthcare utilization outcomes.
PROMIS Global Health-10 is a validated patient reported outcome measure (PROM) comprising a 10-item measure that assesses overall physical and mental health. These questions are then rated on a 5-point Likert scale from poor to excellent that are summated into a physical health raw score and a mental health raw score ranging from 4 to 20. A higher score is indicative of a healthier patient. 16
Statistical Methodology
Kruskal-Wallis H tests and Pearson’s chi-squared tests were utilized to compare continuous and categorical variable percentages. Univariate and multivariable regression analyses were to analyze the association of CTS diagnosis with poor access to care as well as to identify patient-specific factors associated with each domain of reduced access to care. Only values significant on univariate analysis (<.05) were included for multivariable regression of patient-specific factors. All statistical tests were 2-sided. A P-value less than .05 was deemed significant for all statistical tests. Analysis was conducted in the All of Us workbench online using Jupyter Notebooks (Project Jupyter).
Results
Overall Patient Characteristics
For this study, 7649 patients with CTS were included and control matched to 7649 patients without CTS. Average age of patients in the CTS cohort was 64.0 (SD = 12.9) and 71.6% of patients were female (n = 5478). Average physical health raw score was 14.1 and average mental health raw score was 13.9. Age, sex at birth, physical health, and mental health did not vary between the CTS and control cohorts. The CTS cohort had a higher proportion of Black or African American patients (13.8% vs 12.5%, P < .001) and a smaller proportion of Hispanic or Latino patients (1.5% vs 1.8%, P < .001) when compared to the control group. More patients with CTS had an income below $50 000 (36.7% vs 33.6%, P < .001) and fewer patients with CTS had a college degree (50.0% vs 57.6%, P < .001) compared to controls (Table 1).
Patient Demographics of Matched Carpal Tunnel Syndrome and Control Cohorts.
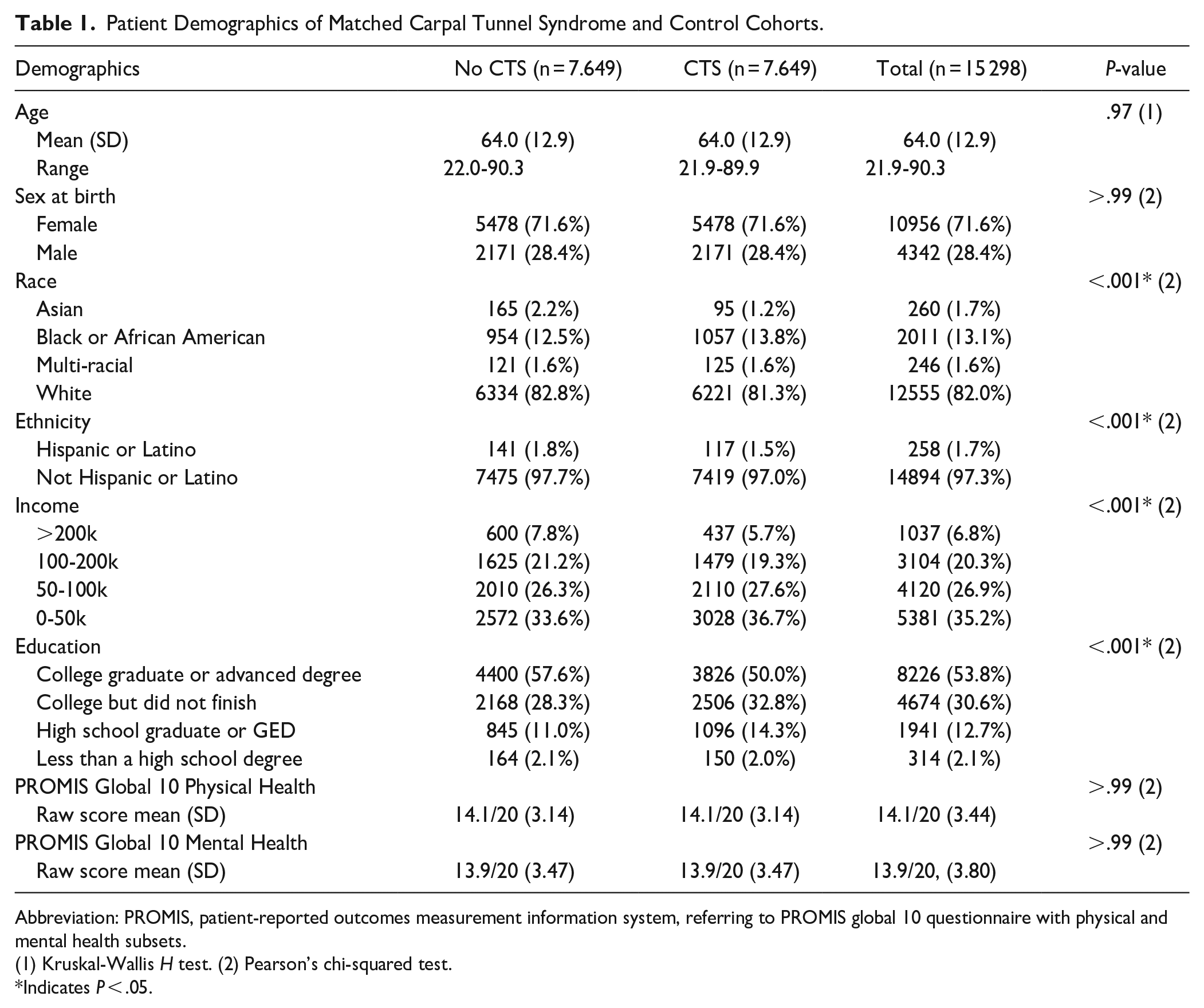
Abbreviation: PROMIS, patient-reported outcomes measurement information system, referring to PROMIS global 10 questionnaire with physical and mental health subsets.
(1) Kruskal-Wallis H test. (2) Pearson’s chi-squared test.
Indicates P < .05.
Of patients diagnosed with CTS, 33.7% (n = 2577) had delayed care, 30.4% (n = 2323) could not afford care, 15.4% (n = 1180) skipped medications, and 1.6% (n = 123) had not seen a provider in more than 1 year. On multivariable analysis, patients with CTS did not have a statistically significant difference in rates of delayed care, inability to afford care, or skipped medications compared to the control group. However, patients with CTS were less likely to go over 1 year without seeing a provider (OR = 0.50, P < .001) (Table 2).
Multivariable Analysis of Carpal Tunnel Syndrome as a Predictor of Access to Care.

Indicates P < .05.
Factors Associated With Poor Access to Care
Among patients with CTS, factors associated with increased likelihood of delayed care included moderate associations with income less than $50 000 (OR = 1.49, P < .001), having a college education (OR = 1.43, P = .02), and “single” marital status (OR = 1.12, P = .04). Protective factors associated with decreased likelihood of delayed care included a moderate association with male sex (OR = 0.72, P < .001) and minor associations with older age (OR = 0.96, P < .001), better physical health (OR = 0.94, P < .001), and better mental health (OR = 0.91, P < .001; Table 3).
Multivariable Analysis of Carpal Tunnel Release and Demographic Factors as Predictors of Access to Care in Patients With a Carpal Tunnel Syndrome.
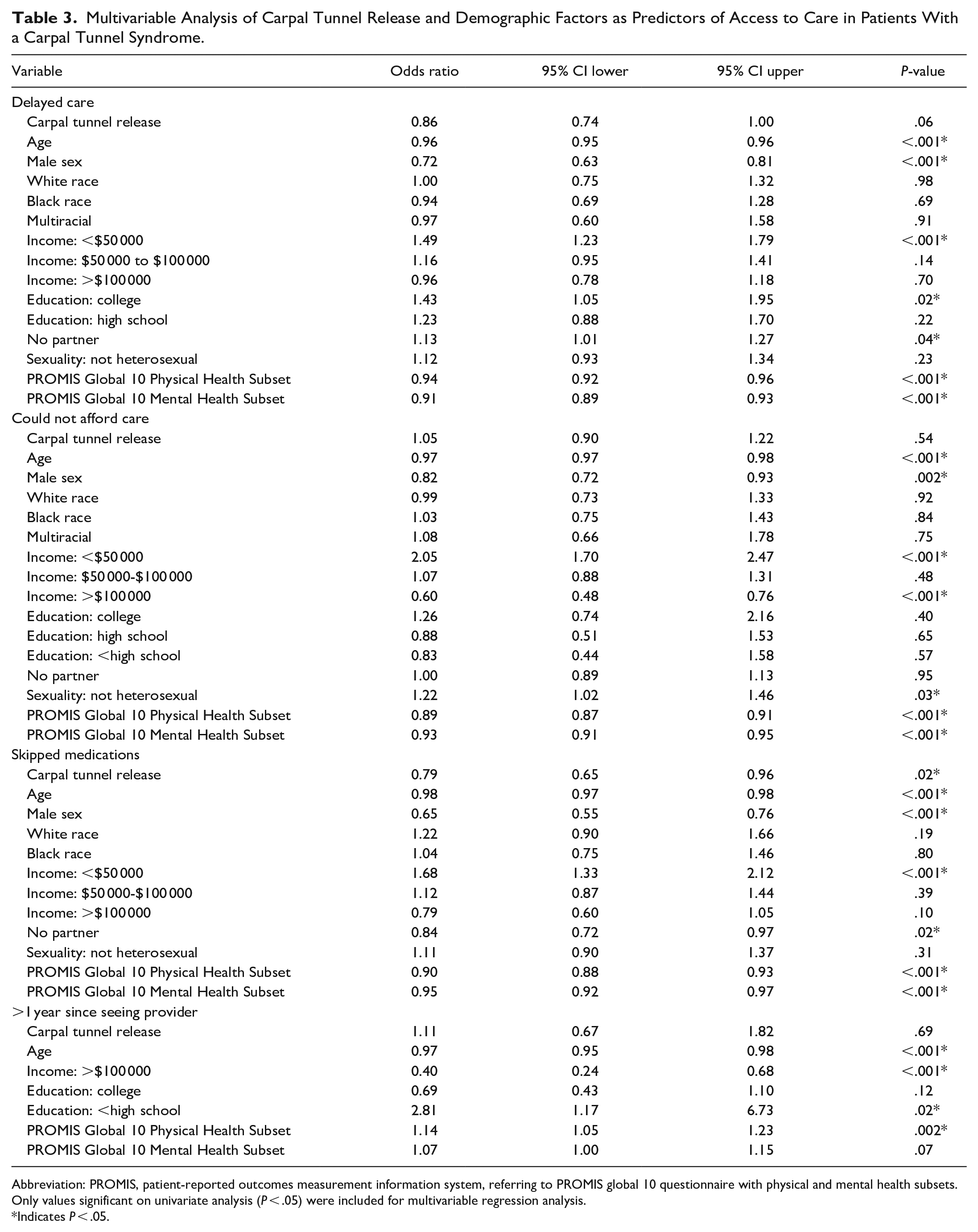
Abbreviation: PROMIS, patient-reported outcomes measurement information system, referring to PROMIS global 10 questionnaire with physical and mental health subsets.
Only values significant on univariate analysis (P < .05) were included for multivariable regression analysis.
Indicates P < .05.
Factors associated with an increased likelihood of inability to afford healthcare included a strong association with income less than $50 000 (OR = 2.05, P < .001) and a moderate association with non-heterosexual orientation (OR = 1.22, P = .03). Protective factors associated with decreased likelihood of inability to afford care included moderate associations with male sex (OR = 0.82, P = .002), income greater than $100 000 (OR = 0.60, P < 0.001), and better physical health (OR = 0.89, P < .001), as well as a minor association with older age (OR = 0.97, P < .001) and better mental health (OR = 0.93, P < 0.001; Table 3).
Factors associated with increased likelihood of skipped medications included a moderate association with income less than $50 000 (OR = 1.68, P < .001). Protective factors associated with decreased likelihood of skipped medications include moderate associations with previous carpal tunnel release (OR = 0.79, P = .02), male sex (OR = 0.63, P < .001), and “single” marital status (OR = 0.84, P = .02), as well as minor associations with older age (OR = 0.98, P < .001), better physical health (OR = 0.90, P < .001), and better mental health (OR = 0.95, P < .001; Table 3).
Factors associated with increased likelihood of going over 1 year since seeing a health care provider included a strong association with not finishing a high school education (OR = 2.81, P = .02), and a moderate association with better physical health (OR = 1.14, P = .002). Protective factors associated with decreased likelihood of going over 1 year since seeing a healthcare provider included a strong association with income greater than $100 000 (OR = 0.40, P = .002) and a minor association with older age (OR = 0.97, P < .001; Table 3).
Discussion
We found that patients experience notable challenges with delayed care, affordability of care, and medication adherence, regardless of having a diagnosis of CTS. However, 1 key difference was that CTS patients are more likely to see their provider within a 1-year time frame. Within the CTS cohort, patients of younger age, female sex, low-income, “single” marital status, non-heterosexual orientation, worse physical health, and worse mental health are particularly at risk of poor access to care.
There are several limitations to our study. First, the use of an observational and retrospective database has inherent limitations including completeness of data based on diagnosis and procedure codes and ability to determine causality and temporal relationships between variables. Second, the All of Us database is reliant on volunteer participation and self-reported survey data, introducing selection bias with findings that may not be representative of all populations even within the United States. This is underscored by possible geographic bias with certain urban regions benefitting from large-scale outreach for recruitment for the database and other geographic areas relying on direct volunteer participation. The All of Us database is also specific to the United States population and findings may not translate to other countries. Third, there were no differences in age, sex, physical health, or mental health, but slight differences in race, ethnicity, income, and education persisted which may present a small confounding bias. This is likely a result of attempting to control-match the CTS cohort using the nearest approximation with multiple demographic factors, preventing a true one to one match. We used a large and comprehensive database that focuses on underrepresented minorities in medicine. This improves representation, as the 13.1% of Black or African American patients in our cohort is equivalent to the proportion in the national population. Nevertheless, other cohort demographics may not be completely representative of the general population, limiting the generalizability to some extent. Lastly, the domains of access to care assessed in this study are surrogate measures for healthcare delivery, and may not capture the complexity of unmet needs, access to care, and utilization. While we cannot infer that these health and social factors have a causal relationship with their respective associations with access to care, these factors serve as proxy measures for other unmeasured aspects of access to care. Despite this, examining the intersections of these factors is vital to the health outcomes of our patients. Policy changes at the local, state, and federal level to mitigate the discrepancies in access to care are imperative to providing equitable care.
Our main finding is that patients, regardless of having a diagnosis of CTS, experience notable challenges with access to care, including with delayed care, affordability of care, and medication adherence. One third of patients within the CTS cohort and the non-CTS cohort experienced delayed care, and in both cohorts 30% of patients noted inability to afford care. Despite the disabling symptomatology and high economic burden of the CTS cohort, the challenges in access to care are thus not specific to 1 diagnosis. Rather, our study highlights a pattern of low access to care across diagnoses. Delays in care are particularly relevant for severe CTS, as earlier surgical care has been associated with improved outcomes.17,18 Improving access to care is also an integral component to improving overall health. With such high rates of poor access to care across cohorts, interventions to improve access to care should be a priority. To start, expanding healthcare coverage has been a national factor identified with improving access to care, and expanding community resources and community health centers have been found to be a valuable supplement.19,20 While insurance status can play a vital role in the affordability of care, community resources can target common reasons for delayed care such as transportation. 21
Our study also found patients of younger age, female sex, low-income, “single” marital status, non-heterosexual orientation, worse physical health, and worse mental health are particularly at risk of poor access to care. Similarly, studies done by Brodeur et al 12 and Hooper et al 13 previously identified patients of female sex and higher social deprivation to be less likely to receive surgical treatment with carpal tunnel release. Distinct from our findings, they additionally found non-white race, Hispanic ethnicity, and non-private insurance status to be associated with lower likelihood to receive surgical treatment with carpal tunnel release. While female sex and overall socioeconomic deprivation are identified as a common risk factors in our study, we did not find race to be specifically associated with decreased access to care. Brodeur et al utilized a New York statewide database, whereas Hooper et al utilized the MarketScan Truven Database Medicaid supplement with particular emphasis on African American and White Medicaid patients; these differences in cohorts could contribute to the contrasting findings. Additionally, our study analyzed patient reported survey data as proxies for access to care, providing a varied scope to the lens of access to carpal tunnel care. As we further develop our understanding of social determinants of health, it is clear that these factors are entwined in their relationships to each other and their effects on patient health outcomes. 22 As such, income and socioeconomic deprivation may be a more direct driver than race alone. There is currently a paucity of literature analyzing access to care in this manner for the CTS patient population, and further research is necessary to better delineate the relationship of race and access to care. Addressing such risk factors offers an important avenue for increasing access to care.
We found that lower income was found to have a strong association with delayed care, inability to afford care, and challenges with medication adherence. Having a low income presents as a likely driving factor for poor access in patients with CTS. This is not unexpected, as low income families face a multitude of barriers in utilizing healthcare including insurance coverage, additional healthcare costs not covered by insurance, reduced access to healthcare services, lack of education, and distrust of healthcare providers.23 -26 Many of these patients are not insured, underinsured, or may rely on Medicaid, leading to poor access to subspecialty surgeons. Only a fraction of orthopedic surgeons specializing in hand or sports medicine have been shown to schedule appointments with such patients.27,28 Poor access to subspecialty care in turn delays or halts access to a provider for their conditions, further propagating the disabling symptomatology and economic burden of CTS.27,28 Low-income and associated uninsured or underinsured status ultimately add to the multifactorial barriers that limit patients’ access to care. With regard to improving CTR access specifically, Wide-awake Local Anesthesia No Tourniquet (WALANT) CTR in the clinical setting may be part of the solution. Studies have shown similar outcomes, complications, and patient satisfaction with this variant of CTR compared to other variants performed in hospital operating rooms or outpatient surgery centers.29,30 In addition, WALANT CTR has been shown to be more cost-effective with a myriad of direct saved costs.31 -33 By increasing usage and availability of this variant of CTR, low-income patients may have improved access to definitive treatment for CTS.
Our study identifies both mental health and physical health as key modifiable factors that are opportunities for improving access to care. We found that patients with better physical health and mental health were independently associated with ease of accessing healthcare. In contrast, poor mental health has been associated with poor surgical outcomes relating to complications, length of stay, and functional outcome.34 -36 Poor mental health has also been associated with increased symptom severity and decreased patient capability in musculoskeletal conditions.37,38 Current orthopedic literature underscores avenues for physician improvement in addressing mental health including improved screening and interdisciplinary collaboration.39 -41 A concerted effort by orthopedic surgeons and musculoskeletal care providers to be aware of and address mental and physical health during visits has the potential to improve both patient access to care and ultimately patient outcomes.
Conclusion
Patients experience notable challenges with delayed care, affordability of care, and medication adherence regardless of having a diagnosis of CTS. Among patients with CTS, low income is associated with a large effect on reduced access to care. Targeted interventions for modifiable risk factors such as low income, poor mental health, and poor physical health are important opportunities to improve access to care in musculoskeletal medicine. Specific areas for intervention may include expanded insurance coverage, community resources assisting with transportation to and from clinic visits, and increased usage of WALANT CTR.
Footnotes
Acknowledgements
The All of Us Research Program is supported by the National Institutes of Health, Office of the Director: Regional Medical Centers: 1 OT2 OD026549; 1 OT2 OD026554; 1 OT2 OD026557; 1 OT2 OD026556; 1 OT2 OD026550; 1 OT2 OD 026552; 1 OT2 OD026553; 1 OT2 OD026548; 1 OT2 OD026551; 1 OT2 OD026555; IAA #: AOD 16037; Federally Qualified Health Centers: HHSN 263201600085U; Data and Research Center: 5 U2C OD023196; Biobank: 1 U24 OD023121; The Participant Center: U24 OD023176; Participant Technology Systems Center: 1 U24 OD023163; Communications and Engagement: 3 OT2 OD023205; 3 OT2 OD023206; and Community Partners: 1 OT2 OD025277; 3 OT2 OD025315; 1 OT2 OD025337; 1 OT2 OD025276. In addition, the All of Us Research Program would not be possible without the partnership of its participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Approval from our local Institutional Review Board (IRB) was deemed exempt for this study given the public nature of this data.