
Abstract
Background
Carpal tunnel syndrome is a common condition, but some controversies remain regarding diagnostics and the most effective treatments. As a result, patients often experience decisional conflicts, especially when considering carpal tunnel release surgery. Understanding factors that influence decision-making in surgery can help clinicians better grasp patient treatment preferences and priorities, reducing decisional conflicts, and enabling patients to make informed, value-aligned choices through shared decision-making. This qualitative evidence synthesis aims to explore patient perceptions of carpal tunnel release, examine the decision-making factors, and critically appraise and synthesise the existing evidence.
Methods
A systematic search was conducted across four electronic databases (MEDLINE, EMBASE, CINAHL Ultimate, PsycINFO) from inception to August 2023, supplemented by referencing and citation searching to identify eligible qualitative studies. Thematic synthesis was adopted as synthesis methodology, involving a line-by-line coding of the primary study findings, and the development of descriptive and analytical themes. Quality appraisal was conducted using the modified Critical Appraisal Skills Programme checklist, supplemented with the COnsolidated criteria for REporting Qualitative research checklist.
Results
Synthesis of six qualitative studies encompassing 66 participants generated five analytical themes: (1) Journey to normalcy, (2) Patient-centred care, (3) Work and life considerations, (4) Weighing up alternatives, and (5) Shaping the expectations, highlighting the complexity of patient decision-making in carpal tunnel release.
Discussion
In the management of carpal tunnel syndrome, therapists should consider various decision-making factors, prioritising communication and shared decision-making. This, along with personalised interactions, achieves patient-centred care and enhances patient care quality and therapeutic alliance.
Keywords
Introduction
Carpal tunnel syndrome (CTS) is a common peripheral nerve entrapment condition, affecting approximately one in 10 individuals during their lifetime. 1 Despite its prevalence, managing CTS is marked by significant debate, leading to uncertainty about the most appropriate course of action. Ambiguity persists regarding the need for and interpretation of electrodiagnostic testing, the effectiveness of various conservative treatments, and the role of surgery in the absence of definitive symptoms and electrodiagnostic test results. 1 Consequently, uncertainties remain regarding the optimal timing and choice of treatment.
In situations where diagnosing and managing CTS lacks a consensus, patients often experience decisional conflict, stemming from unclear preferences, biases, limited support, and knowledge. 2 Hageman et al. 3 highlighted a disparity between patient and hand surgeon preferences for CTS treatment, with patients preferring non-operative, painless treatments while surgeons prioritise options with minimal risks. Subsequently, Hageman et al. 4 revealed that hand surgeons generally perceive CTS as having straightforward treatment options, resulting in less decisional conflict compared to patients. These differences highlight the importance of acknowledging patients’ preferences, especially their inclination to avoid surgery, which may be underestimated by clinicians.
Carpal tunnel release (CTR) surgery is a widely recognised and effective treatment for CTS. Nevertheless, some patients may be hesitant to undergo surgery due to concerns about morbidity, a continued belief in successful conservative treatments, or fears regarding the extended postoperative recovery period.5,6 However, delaying surgery risks irreversible nerve damage and suboptimal outcomes, with studies showing that delaying for more than 6 months post-diagnosis results in slower and incomplete recovery of hand function and grip strength.6–8
Given the complexity of decision-making and patient hesitancy towards surgery, understanding patient treatment preferences and priorities in CTR is crucial to clinicians. Qualitative studies can offer valuable insights by revealing patients’ attitudes, perspectives, and beliefs. 9 While existing qualitative studies10–12 have explored the patient experience of CTS and perceptions of CTR, they may not capture the full spectrum of patient perspectives.
In recent years, qualitative evidence syntheses (QES) have gained recognition for systematically reviewing primary qualitative research in healthcare studies. 13 QES serve to summarise findings and consolidate multiple perspectives, including contradictory viewpoints, which may not be fully represented within a single study, thus generating conceptual insights or theories. 14 While similar QES have been conducted on the decision-making process for total knee replacement surgery, 15 such syntheses are lacking in CTS research. Thus, conducting a QES regarding the perceptions of CTR may provide a more comprehensive understanding of patient preferences, motivations, and concerns, offering detailed interpretations and insights into their decision-making experiences. 16
The objective of this review therefore is to identify, appraise, and synthesise current evidence regarding patient perceptions of CTR, focusing on factors influencing patient decision-making of CTR.
Methods
This review adheres to the Enhancing Transparency in Reporting the Synthesis of Qualitative Research (ENTREQ) statement. 17
Eligibility criteria
The study’s eligibility criteria adhere to the PICOS (Population, Intervention, Context, Outcomes, and Study Design) framework
18
: (i) Population: Individuals aged 18 or older diagnosed with CTS seeking healthcare services, regardless of severity, duration, demographics, or previous treatment. Exclusions include mixed samples with other conditions. (ii) Intervention: Studies investigating participant perceptions of any CTR method. (iii) Context: Studies examining contextual factors affecting perceptions of CTR, including location, socioeconomic status, and caregiver presence. (iv) Outcomes: Studies exploring perceptions, experiences, and decision-making regarding CTR. Exclusions are studies not focused on these aspects. (v) Study Design: Qualitative research
19
using methods such as focus groups and interviews are included. Mixed methods studies with qualitative components are included, while non-qualitative studies and non-empirical works are excluded.
Electronic searches and search term
Comprehensive electronic searches were conducted on MEDLINE, EMBASE, CINAHL Ultimate, and PsycINFO databases from inception to August 2023, limited to English-language studies. The search employed a combination of free-text terms and Medical Subject Headings (MeSH) based on PICOS categorisation 18 : P (Participants with CTS), I (CTR surgery), C (Not available), O (Perception and preferences), S (Qualitative research). Tailored search strategies for each database were developed, incorporating validated qualitative search filters to optimise results.20–23 Backward reference checking and forward citation searching via Google Scholar supplemented the electronic searches.24,25 The complete search strategy for the four databases can be found in Appendix 1.
Study selection
The search results obtained from electronic and supplementary search strategies were collated in Zotero. Due to the relatively low sensitivity of the search for qualitative studies, the 1st author initially screened the titles and abstracts of all identified studies using three straightforward criteria. Studies were excluded if they: (1) were unrelated to CTS or CTR surgery; (2) did not include participants with CTS; (3) were not qualitative studies. Subsequently, a full-text screening was carried out to determine whether the studies met the full eligibility criteria for inclusion. Any issues raised were resolved through discussion with the 2nd author.
Data extraction, analysis and synthesis
A data extraction form was developed by the 1st author in discussion with the 2nd author. The 1st author independently extracted data on study characteristics (authors, publication year, country of conduct), study population details (sample size, gender, age, ethnicity, employment status), study aims, data collection methods, data analysis methods and the other relevant information for data analysis.
Thematic synthesis
26
served as the synthesis methodology for this review. It is endorsed by Cochrane as a recommended qualitative evidence synthesis method
27
and has been extensively applied in various policy and practice domains. Thematic synthesis comprises three fundamental stages
26
: (i) Line-by-line coding of primary study findings. (ii) Organising codes into “descriptive themes”. (iii) Synthesising “analytical themes” through a deeper interpretation of the data.
The 1st author began by systematically screening the included studies to gain an overall understanding of their content. The results, findings, and conclusions from both the abstracts and full texts of the included studies were electronically extracted as “data” and subsequently transferred to Microsoft Word for further analysis. Line-by-line coding was then conducted by the 1st author using Microsoft Word’s comment function, with new codes added to a code bank. The codes were synthesised to translate concepts across studies and systematically organised in Microsoft Excel. Codes were subsequently grouped into broader “descriptive themes” inductively based on content similarity, applying qualitative thematic analysis. 28 In the final phase, the “descriptive themes” were collated to synthesise “analytical themes” that revolved around factors influencing patient decision-making concerning CTR. This interpretation relied on the authors’ knowledge and insight regarding CTS and CTR. These themes were then presented using illustrative quotations from the original studies.
Quality appraisal of study methodology
The modified Critical Appraisal Skills Programme (CASP) checklist for qualitative studies, 29 along with the COnsolidated criteria for REporting Qualitative research (COREQ) checklist, 30 were employed by the 1st author to appraise the trustworthiness31–34 of the included studies. The COREQ checklist was used to enhance quality assessment by offering detailed guidance on what to assess in each of the domains covered in the modified CASP checklist. The incorporation of COREQ alongside CASP has been seen in other QES.35,36
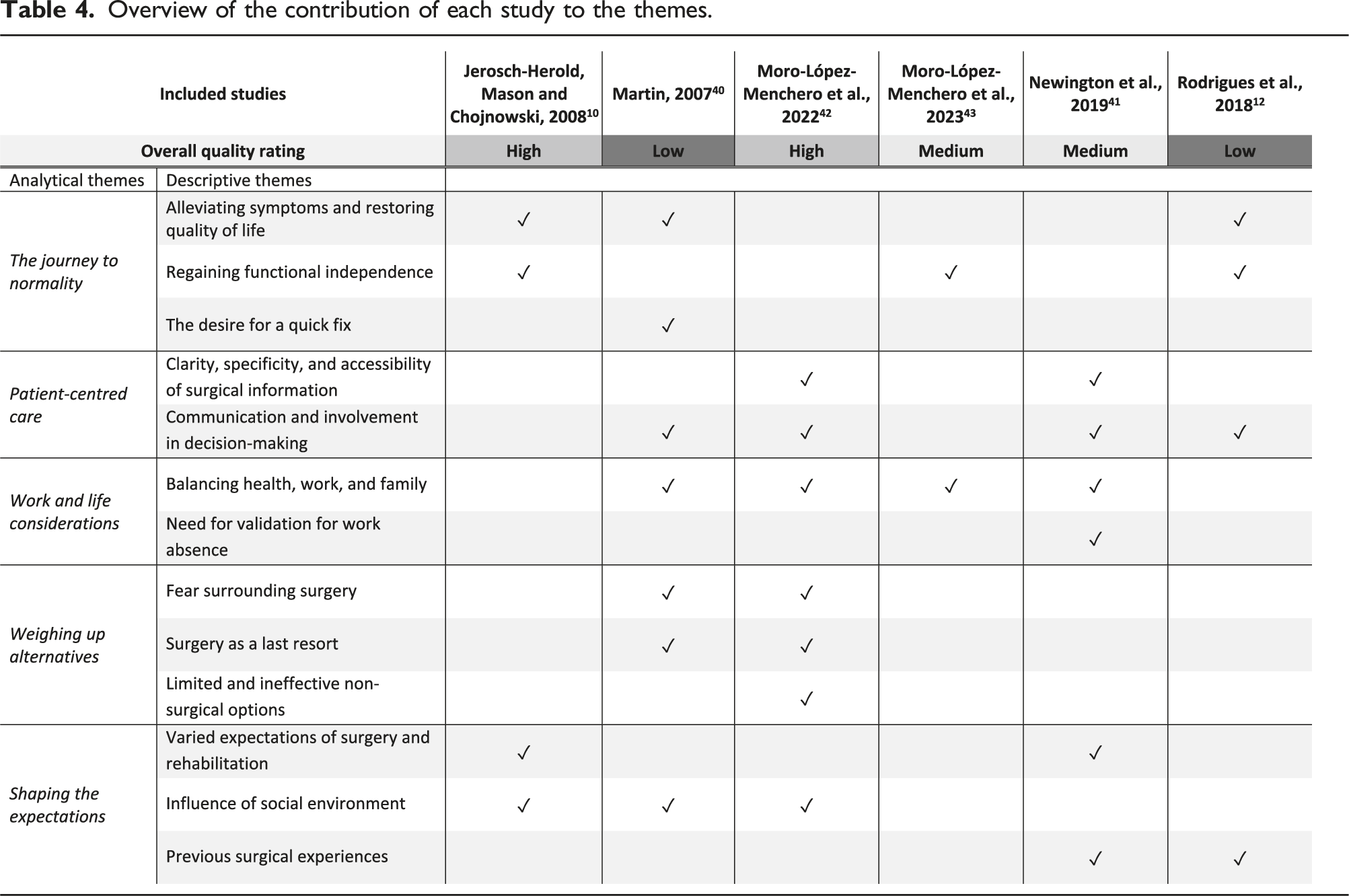
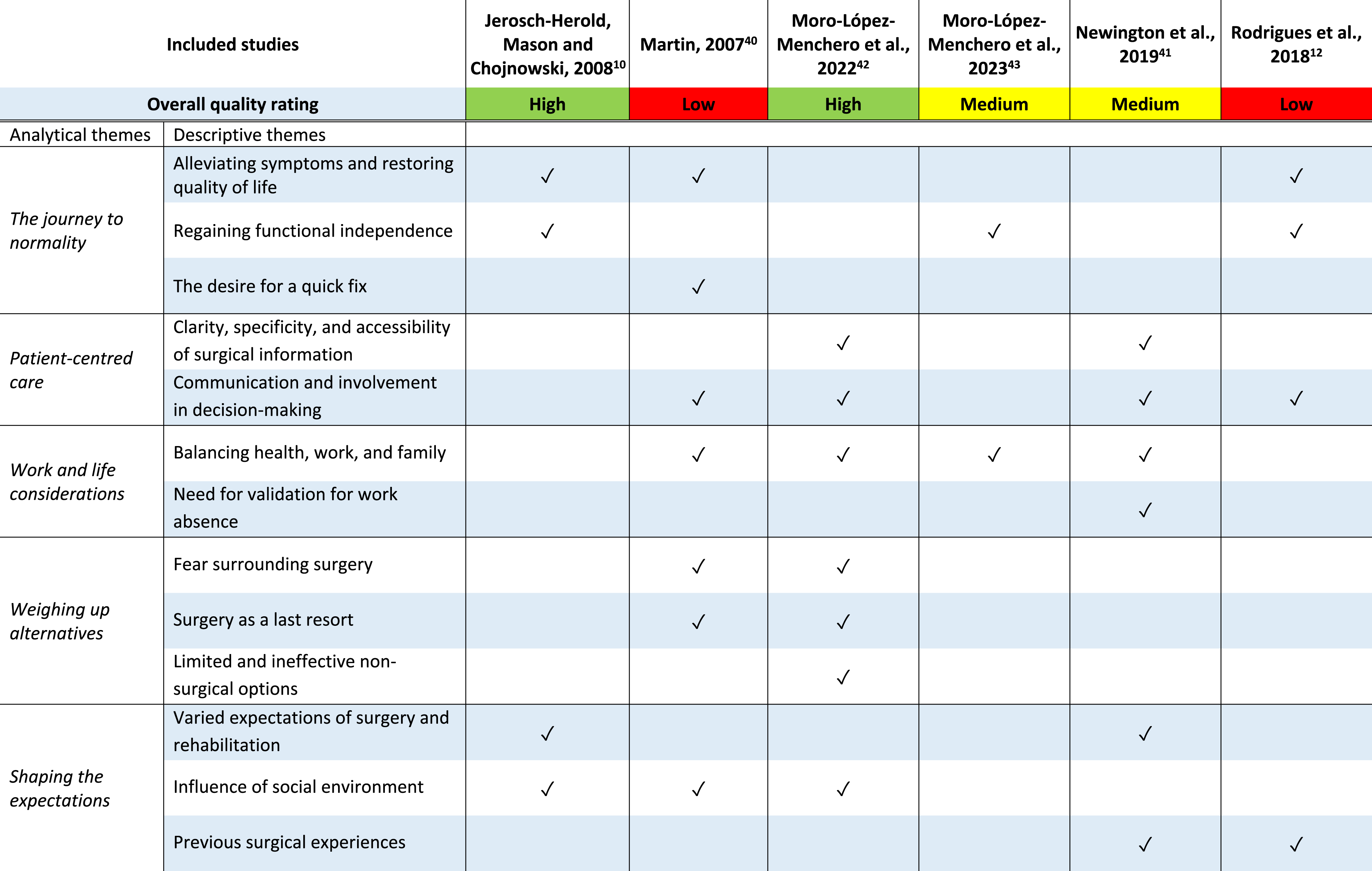
The question whether to exclude low-quality studies from data synthesis remains a topic of discussion. 37 The absence of consensus and standardisation in excluding low-quality studies, attributed to subjective and uncertain criteria, raises concerns about potential arbitrary exclusions and questions whether the quality appraisal checklists genuinely assess study design and execution or merely methodological reporting quality. 38 Dixon-Woods et al. 39 also suggested that research of lower quality, due to methodological weaknesses or inadequate reporting, might still uncover additional insights derived from the data. Hence, we chose to present an overview of each study’s contributions to the themes after synthesis, to preserve all potentially valuable insights. This approach avoids the exclusion of studies based solely on quality appraisal, thereby enabling readers to gauge the significance of study findings in relation to the overall quality of the studies.
Furthermore, while some researchers assign scores to studies, Cochrane has cautioned against this practice due to the unequal weighting of quality domains, potentially yielding misleading and imprecise scores. 27 Therefore, we opted to assign an overall quality rating (low, moderate, and high) based on the study’s overall rigour and credibility.
Reflexivity statement
As part of our commitment to maintaining rigour in qualitative research, we, the review authors, have critically considered how our personal views and opinions regarding CTS might influence the decisions made during the design and conduct of this study, as well as how the study results could impact those views and opinions.
This review was conducted as part of the 1st author’s graduate dissertation in occupational therapy. Consequently, the analysis was carried out solely by the 1st author. This solitary approach to analysis was primarily motivated by the requirement for graduation and lacked any preconceived notions regarding the findings. This lack of prior bias is an important strength, as it ensures that the review was driven by the data itself rather than any prior expectations or assumptions.
When considering cultural positions, it is noteworthy that the 1st author is an Asian Chinese who is a non-native English speaker living in Hong Kong for almost his whole life. The first author is aware that being an outsider to the culture under investigation may pose challenges in fully understanding colloquial language or nuanced meanings in English. However, this potential limitation is minimized due to the nature of this research as a review, rather than an interview-based study. The review process relies on existing literature, which allows for a more structured and less interpretive approach to language.
The second author contributed her specialized knowledge and expertise in CTS to discuss the implications of the results. Her involvement was crucial in ensuring the findings were interpreted correctly and any potential clinical and practical implications were thoroughly explored. While her expertise added significant value to the discussion, we remained mindful of how professional knowledge and experience could shape the interpretation of the data.
By maintaining a transparent and reflective stance throughout the research process, we aimed to mitigate the influence of our personal and professional biases, ensuring that the synthesis of qualitative evidence remained as objective and rigorous as possible.
Results
A systematic search initially yielded 680 records (426 from electronic search and 254 from supplementary search), with 542 titles and abstracts screened for eligibility after the duplications were removed. After a rigorous screening process, 58 studies underwent full-text screening, resulting in the inclusion of six studies10,12,40–43 for comprehensive analysis, all published between 2007 and 2023. A description of the study identification and selection, along with the reasons for exclusion, is illustrated in the flowchart adapted from PRISMA in Figure 1.
44
It is noteworthy that, two of these articles,42,43 authored by Moro-López-Menchero et al., involved the same group of participants and conducted interviews but pursued different research objectives and analyses. Rather than assessing the results of just one of these articles, we merged the findings from both to encompass all dimensions of participants’ experiences. Flowchart of study identification and selection adapted from PRISMA.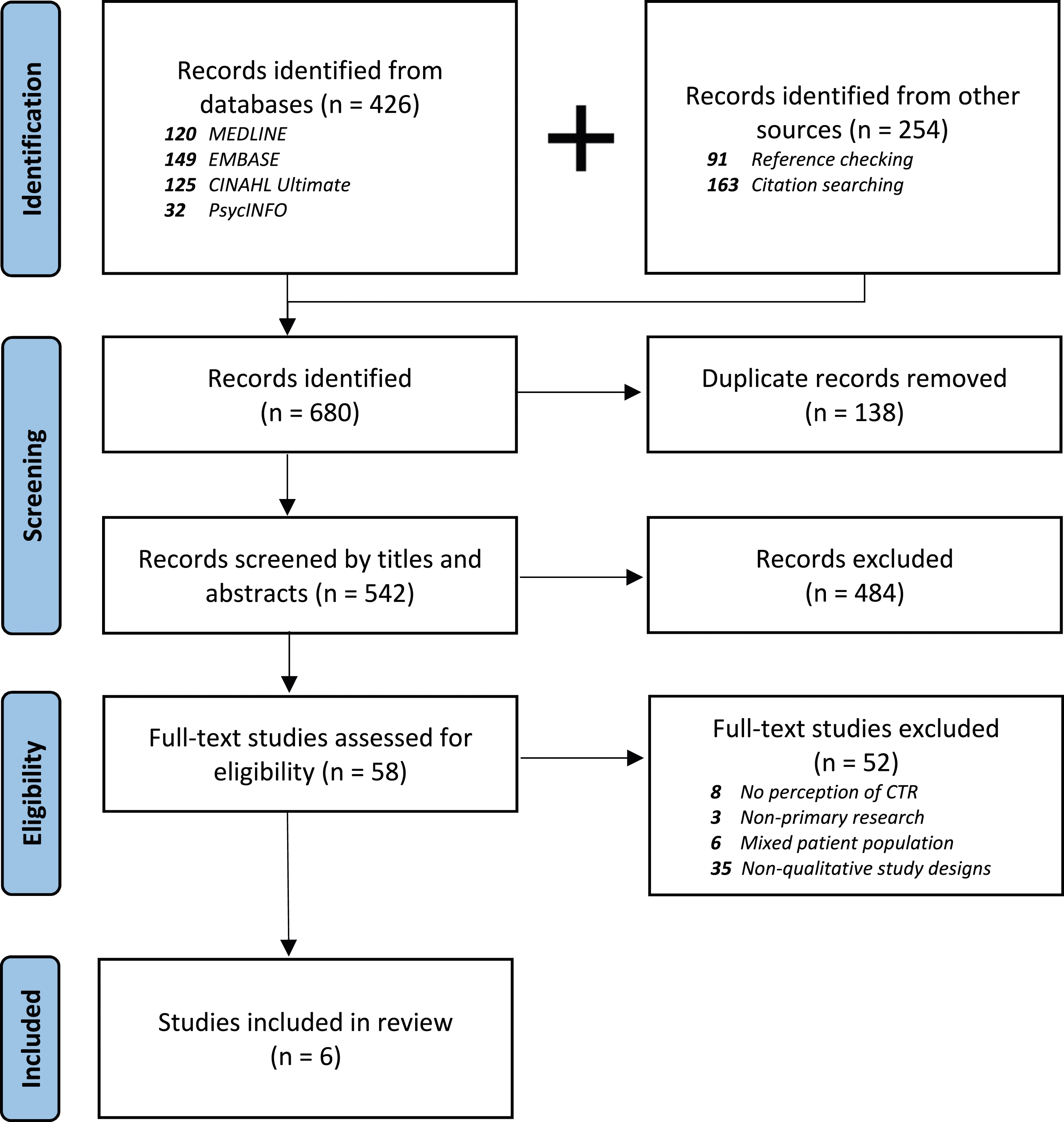
Characteristics of included studies
Characteristics of included studies.
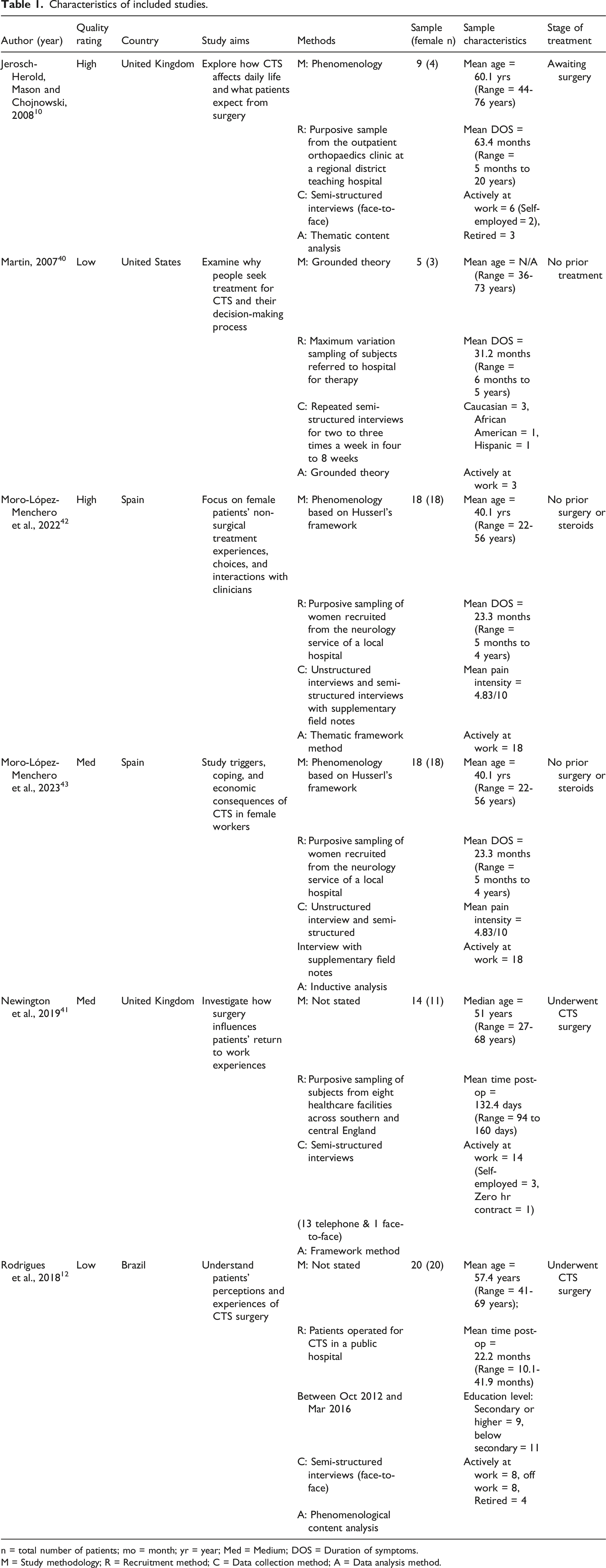
n = total number of patients; mo = month; yr = year; Med = Medium; DOS = Duration of symptoms.
M = Study methodology; R = Recruitment method; C = Data collection method; A = Data analysis method.
They were conducted in diverse geographical locations, spanning the United Kingdom,10,41 Spain,42,43 the United States, 40 and Brazil. 12 The majority occurred in high-income countries (the United Kingdom, Spain, and the United States), with one in an upper-middle-income country (Brazil), following the World Bank’s 2016 criteria. 45 Collectively, 66 participants with CTS were included in these studies, with a mean age of approximately 51 years (ranging from 22 to 76 years) and a majority of female participants (n = 56). Among them, 49 participants remained employed while 17 had withdrawn from the workforce for various reasons.
Among the six included studies, four10,40,42,43 explored participants who had not undergone CTR, either due to non-acceptance or while awaiting the procedure. The reported symptom duration ranged from 6 months to 20 years, with an average of 36 months and a median of 24 months. Conversely, two studies12,41 examined participants who had undergone CTR. About 52% of the participants (n = 34) had undergone surgery as part of their CTS treatment.
Quality appraisal
Summary of the quality appraisal of the included studies using a modified CASP checklist.
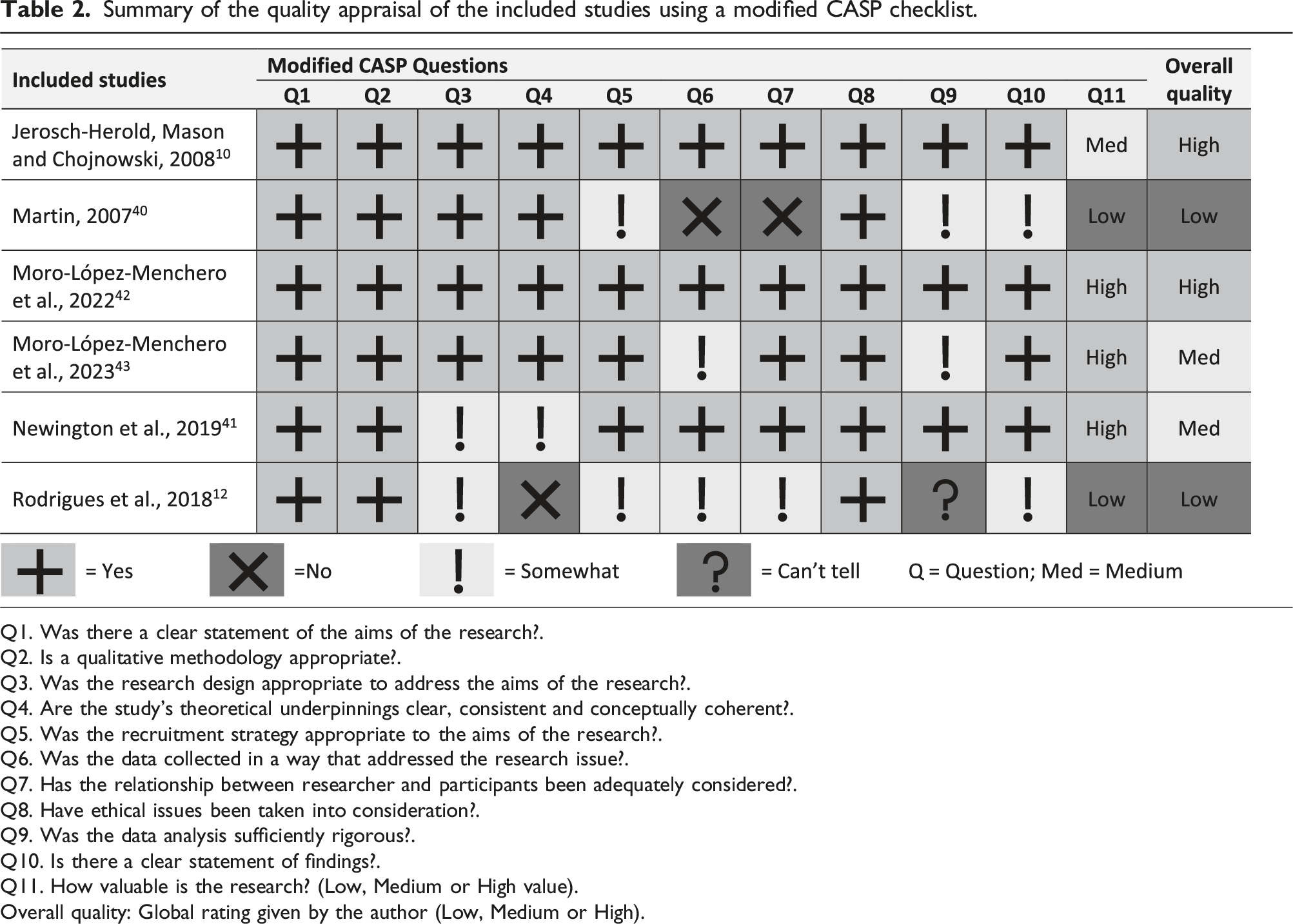
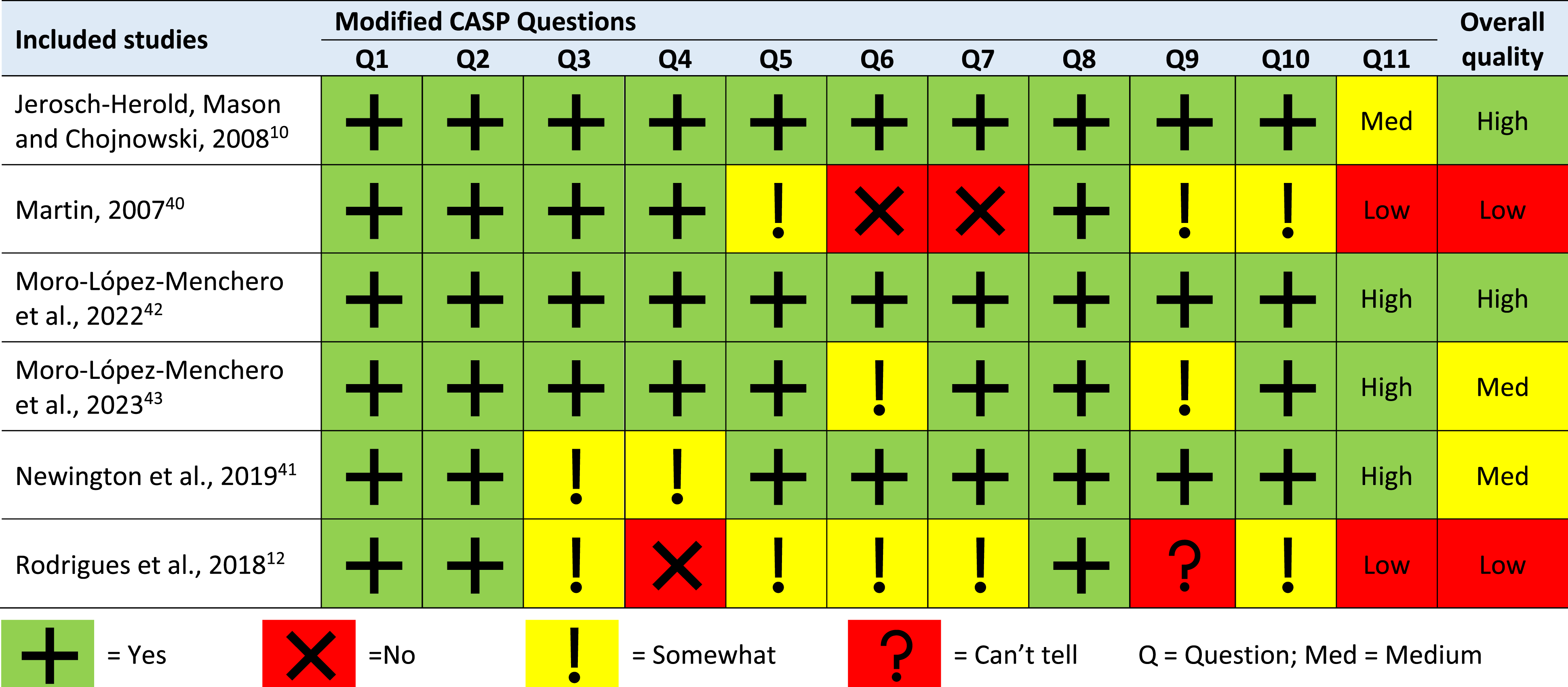
Q1. Was there a clear statement of the aims of the research?.
Q2. Is a qualitative methodology appropriate?.
Q3. Was the research design appropriate to address the aims of the research?.
Q4. Are the study’s theoretical underpinnings clear, consistent and conceptually coherent?.
Q5. Was the recruitment strategy appropriate to the aims of the research?.
Q6. Was the data collected in a way that addressed the research issue?.
Q7. Has the relationship between researcher and participants been adequately considered?.
Q8. Have ethical issues been taken into consideration?.
Q9. Was the data analysis sufficiently rigorous?.
Q10. Is there a clear statement of findings?.
Q11. How valuable is the research? (Low, Medium or High value).
Overall quality: Global rating given by the author (Low, Medium or High).
The completeness of reporting varied across the studies, covering 17 to 31 of the 32 COREQ framework items. All six studies specified sample size and participant characteristics, and included participant quotations in the results. Five studies discussed data saturation and previous relationships with participants. However, only half of the studies reported interview duration, use of field notes, returning transcripts to participants, recording methods, and information on participant refusal or dropout. Only one study reported participant checking.
The two studies rated as low quality12,40 had inadequate reporting (both covered 17 out of 32 COREQ framework items) or methodological flaws in data collection and analysis, a lack of clear audit trails for readers, insufficient strategies to establish the credibility of findings and a deficiency in researcher reflexivity regarding their role and relationships with participants.
Data synthesis
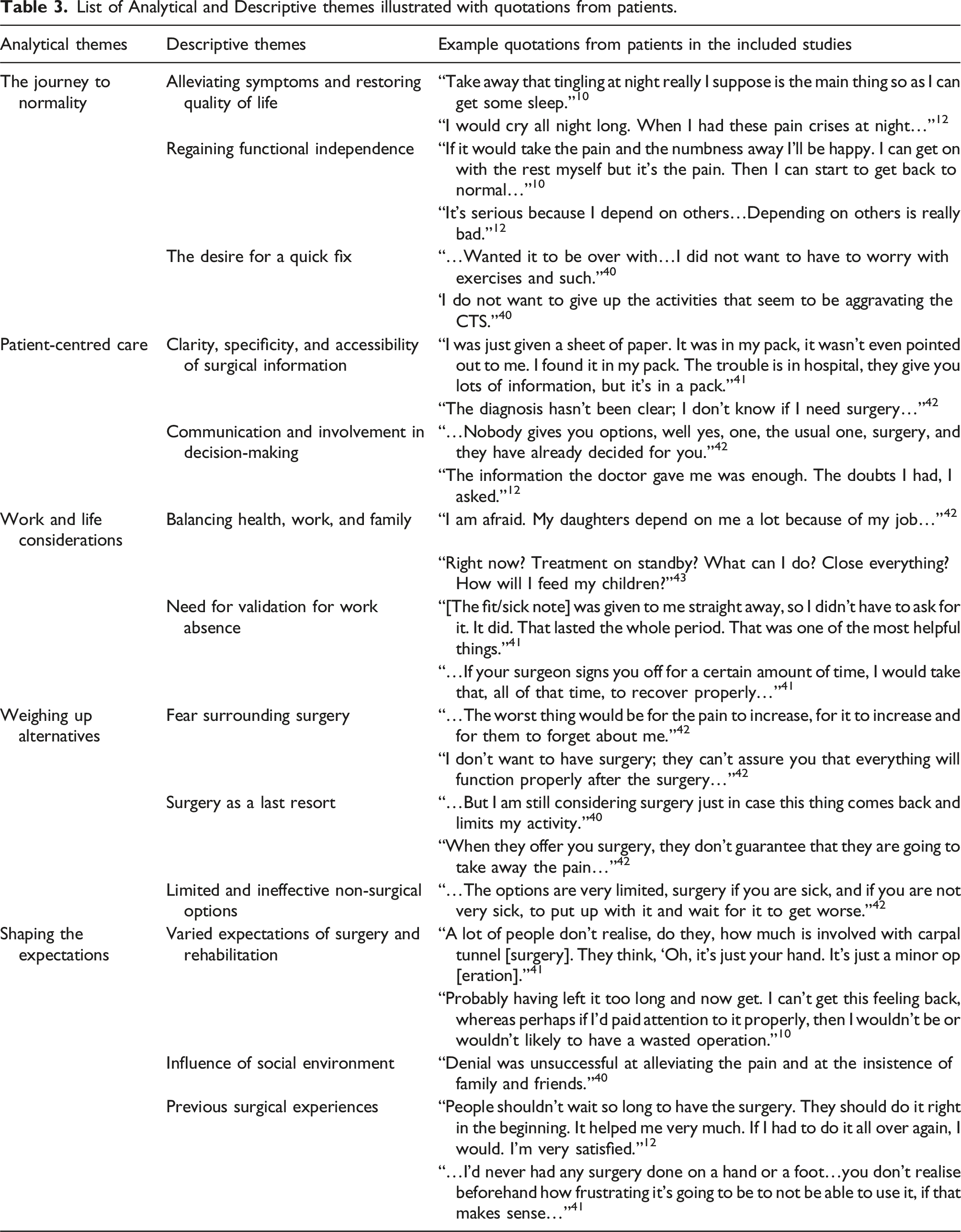
List of Analytical and Descriptive themes illustrated with quotations from patients.
Overview of the contribution of each study to the themes.
The journey to normality
The theme, “The Journey to Normality”, captures the nuanced decision-making process surrounding CTR, emphasising participants’ fervent pursuit of a return to normality in their lives. Participants often seek surgery due to debilitating symptoms, such as numbness, tingling, pain, and stiffness, significantly impacting their quality of life and hope to alleviate this discomfort via surgery.10,12,40 Each participant’s experience highlights the unique nature of their condition. Some participants also express a willingness to endure certain discomforts while prioritising the elimination of specific symptoms through surgery. 10
Beyond symptom relief, participants see CTR surgery as a means to regain functional independence. 12 CTS severely limits their ability to perform fine motor tasks, impacting daily life and professional pursuits. Surgery is anticipated to enable them to resume domestic, professional, and leisure activities without hindrance, as well as regain independence.
Some participants choose surgery to avoid significant changes to daily routines necessitated by conservative treatment. 40 Surgery is perceived as simpler and quicker than alternative treatments like exercises and therapy, offering immediate relief from persistent symptoms and facilitating a return to normality without enduring ongoing lifestyle alterations.
Patient-centred care
The patient-centeredness of care and the quality of information received play pivotal roles in the decision-making process for CTR. This encompasses the clarity, specificity, and accessibility of surgical information, and the degree of patient involvement in treatment decisions.
Numerous participants conveyed that their decisions regarding surgery were confounded by a paucity of clear information about their medical condition and the available treatment options.41,42 They expressed frustration and bewilderment, highlighting that the unclear information left them uncertain about the necessity of surgery, significantly impacting their treatment choices and motivation for the procedure. Some participants desired more personalised and proactive support from their clinicians, as the general guidance provided did not adequately address their individual circumstances or provide insight into the rationale and consequences of surgery.41,42 For instance, participants received peri-operative information that emphasised aspects like wound care while overlooking their specific concerns about function. 41 Moreover, the way information was delivered acted as a barrier to decision-making, as some participants received unclear information packs, making it challenging for them to understand and engage with the provided information. 41 The absence of comprehensive and tailored information fostered scepticism towards surgical decisions.
Participants often felt marginalised in the decision-making process, perceiving that clinicians had already arrived at conclusions without considering their perspectives.40,42 The binary treatment option—acceptance or refusal of surgery—reinforced the perception that surgery was the only viable choice. 42 This perceived rigidity, coupled with reported shortcomings in clinicians’ responsiveness and limited consultation time, led to frustration, strained relationships, and dissatisfaction with their involvement in decision-making. 42 Despite these challenges, some participants had positive experiences when clinicians communicated transparently and explained the associated risks and benefits. 12 While shared decision-making was valued by most participants, some preferred a more self-reliant approach, emphasising their own judgment and incorporating expert advice into their unique circumstances. 41
Work and life considerations
The decision-making process for CTR involves a delicate balance between health, work commitments, and family responsibilities, with particular emphasis on how surgery will impact professional life and financial stability. Participants express significant concerns about taking time off work for surgery, fearing it will disrupt their ability to fulfil job responsibilities.40–43 This fear stems from the need to maintain income and support families, leading to difficulty in balancing between treatment demands and parental responsibilities. Self-employed individuals and business owners face additional challenges, as surgery may disrupt their businesses.41,43 The fear of impacting livelihoods and financial stability often leads individuals to delay or reject surgery.
Moreover, there is a notable need for validation to justify time away from work due to surgery. 41 Sickness certification, obtained from surgical teams, is highly valued as formal confirmation of the need for work absence. Surgeons’ authority in providing this validation is crucial. Participants also perceive it as internal validation, affirming that their absence from work is legitimate. 41 The availability of sickness certification holds significant importance for working-class individuals, enabling and motivating them to accept surgical treatment.
Weighing up alternatives
Non-surgical options for managing CTS allow participants to carefully consider their choices. Fear of surgery and its perceived risks dissuade many from viewing surgery as a viable option. However, for some participants, the inefficacy of non-surgical treatments creates a dilemma: choosing between effective but risky surgery and ineffective non-surgical options.
Participants have a profound sense of apprehension surrounding the decision-making process of surgery, encompassing fears about the surgical procedure, the operating room environment, anaesthesia, potential complications, and post-surgery consequences.40,42 Collectively, these fears portray surgery as a daunting prospect, despite its potential benefits, casting a long shadow of anxiety and uncertainty over the decision-making process.
Many participants see surgery as a last-resort option due to its risks, believing it should be pursued only after exhausting other alternatives.40,42 In their view, surgery represents a final, potentially life-altering step taken only when no other viable options remain. Despite this cautious perspective, some participants still view surgery as a beacon of hope, even after trying non-surgical treatments that offered temporary relief. 40
Several participants expressed frustration with the limited non-surgical treatment options for conditions not requiring surgery. 42 They desired a broader spectrum of choices that bridged the gap between conservative treatment and surgery. Throughout their experience, they faced a dilemma, torn between the prospect of surgery and the acceptance of conservative treatments that often failed to provide relief.
Shaping the expectations
The overarching theme of “Shaping the Expectations” examines how factors such as the social environment and past surgical experiences influence participants’ expectations of surgery, crucial in their decision-making process regarding surgery participation.
Participants held diverse expectations regarding the surgical process and rehabilitation period, ranging from an immediate return to normality to the anticipation of weeks or months of recovery.10,41 Some participants, due to the belief that they had delayed surgery for too long, harboured limited expectations, fearing that the delayed intervention might compromise the results, leading to their decision to undergo surgery. 10
Participants’ expectations were also significantly shaped by their social environment, including family and neighbours,.10,40,42 Opinions and information shared within this social network played a pivotal role in shaping participants’ choices regarding surgery. Some participants shared how their expectations of time to recovery are influenced by knowledge of others’ experiences of surgery. 10 This highlights the impact of the social environment in guiding individuals towards or away from surgery.
Participants’ previous experiences, or lack thereof, with surgery, had a considerable impact on their decision-making processes. Those lacking prior surgical exposure often underestimate the complexity and consequences of the procedure, perceiving it as minor, thus driving their decision to undergo surgery. 41 Conversely, participants with prior surgical experience expressed satisfaction and recommended surgery to others. 12 These individuals approached their decision-making process with more confidence and insights from their past experiences, potentially guiding their future choices.
Discussion
This is the first QES investigating the patient perception of CTR, with a focus on the factors influencing patient decision-making. The findings reveal that decision-making in CTR is complex, driven by the desire to relieve debilitating symptoms and regain independence. Participants consider the appeal of quick relief through surgery and potential disruptions from non-surgical options. They also navigate fears, assess surgery risks and benefits, and consider its impact on work and family life. Social influences and past surgical experiences shape participant expectations. Patient-centred care, providing clear, personalised information and active involvement in decision-making, significantly influences the decision-making process.
Our findings align with other studies emphasising the significance of symptom relief, ineffective non-surgical treatments, work-family considerations, and the social influence in surgical decision-making. In a retrospective study conducted by Gong et al., 46 involving 282 female patients diagnosed with CTS, key factors influencing the decision to undergo CTR were identified. The top five reasons for choosing CTR included the presence of severe symptoms, failed conservative treatments, and knowledge of successful outcomes in others, while the fear of surgery and the economic burden on their families were the top reasons for avoiding CTR. These findings are also consistent with a similar study on total knee replacement surgery by O’Neill et al., 15 which revealed common themes in surgical decision-making, revolving around symptom perception, negative perceptions of surgery risks, and effective communication about the surgical process.
Furthermore, the review revealed that some participants favoured surgery over conservative treatments due to their perception of surgery as a quicker and more effective solution, without the need for lifestyle adjustments. This aligns with the findings of Hageman et al., 3 which found that patients generally preferred non-invasive treatments but acknowledged their limitations as palliative and lacking the immediacy in facilitating a quick recovery for resuming regular activities.
Our review underscores a consistent trend where participants often experience marginalisation and insufficient information in pre-operative decision-making, highlighting the need for shared decision-making during this phase. Previous research on the decision-making in CTR supports these findings, indicating a preference for shared decision-making, especially before surgery.47–50
Gong et al. 47 delved further, revealing that patients with milder symptoms tend to prefer a collaborative role in decision-making, while those with a history of prior surgery, a caregiver, and private insurance leaned towards a more active role. This aligns with our findings that previous surgical history significantly shapes participants’ expectations, potentially prompting a more proactive role in surgical decision-making. Moreover, private insurance can alleviate financial concerns for patients and their families, which is a significant factor in the decision-making process, as supported by Kortlever et al., 49 who also found an association between private insurance and a preference for reduced surgeon involvement.
Strengths and limitations
The review has several notable strengths. It adhered to the ENTREQ guidelines for reporting, ensuring the integrity and quality of the reviews and enabling readers to assess the reliability and applicability of the review’s findings. The methodology employed in the review is also rigorous, characterised by a comprehensive literature search and the application of modified CASP and COREQ checklists to evaluate study quality. Furthermore, this review encompasses a diverse range of participant perspectives and experiences concerning CTR surgery, ranging from individuals who have undergone the surgery to those awaiting it, as well as those who opt for conservative treatment. This broad spectrum of data sources maximises the diversity of participants, thereby reinforcing the overall synthesis. Furthermore, in the synthesis process, it was observed that the results from studies rated with “low” overall quality were consistent with those from higher-quality studies.
However, several evident limitations should be considered. Firstly, the scarcity of qualitative literature on CTS constrained the depth of the review’s interpretations, given the relative novelty of the research area. In-depth studies specifically addressing the factors influencing the decision to undergo CTR surgery are rare. Many existing studies focus only on general perceptions of CTS and CTR or specific aspects, such as the return to work. 41 This limitation complicates the identification of a comprehensive set of decision-making factors for CTR surgery.
Furthermore, the insights of the review are based on a sample of 66 participants primarily from high-income countries, thereby limiting the transferability of its findings to individuals from other economic backgrounds. The participants had an estimated mean age of 51 years, with the majority (n = 49) being employed, suggesting that the findings are more applicable to a relatively older, working-age demographic.
Despite consistent findings in population studies indicating a significant gender disparity in CTS incidence, with a higher prevalence among women compared to men,51–54 a noticeable gender imbalance persisted within the reviewed dataset. Only 10 male participants were included out of the total 66, potentially introducing gender bias and skewing the findings towards an overrepresentation of female experiences.
Moreover, the review’s search strategy was limited to electronic databases, omitting the exploration of grey literature. While practical considerations, such as time constraints and concerns about the peer-reviewed status of some reports, influenced this decision, it may have limited the breadth of the publication analysis.55,56 It’s worth noting that a unique challenge when integrating grey literature is the potential overrepresentation of data from theses. Theses typically have more generous word limits compared to published articles, which can overwhelm the data from inherently thinner studies. 57 Whenever feasible, prioritising the inclusion of published journal articles derived from theses is advisable. In this review, this was successfully accomplished, as exemplified by the inclusion of one published journal article derived from a thesis. 40
The review’s scope was also constrained to English-language studies, potentially excluding relevant research in other languages. Lastly, it should be acknowledged that the entire review process, including data analysis, was conducted by a sole occupational therapy student, which may not be the ideal approach. 58 A full list of the codes can therefore be made available on request to the corresponding author for transparency and reproducibility purposes.
Implications for clinical practice
In the growing field of musculoskeletal condition management, the Therapist-Led Care Model is gaining prominence. 59 In this model, therapists take on a broader range of responsibilities, including independent patient assessments, patient education, therapeutic interventions, and, in some cases, making treatment decisions beyond their typical scope of practice, such as evaluating the need for surgical intervention.60–62 Consequently, it remains essential for therapists to have a deep understanding of patient preferences and attitudes in order to enhance patient care and assist in the decision-making process.
CTS patients face challenges in making decisions about their care. Among the themes identified in our review, improving patient-centred care through better communication and increased patient involvement in decision-making is a readily adjustable factor for therapists. Patients often experience decisional conflicts and distress due to their limited involvement in the decision-making process. To address these issues, the introduction of decision aids is a potential solution. Decision aids are tools that help patients access medical information, understand their options, weigh the benefits and risks, and navigate the decision-making process. 63 Systematic reviews have shown that decision aids can enhance patients’ knowledge, improve their understanding of medical information, clarify their values, and encourage active participation in decision-making.64,65 This, in turn, leads to more accurate risk perceptions and, ultimately, more values-aligned choices.
However, a recent study by Gong et al. 66 suggests that decision aids may not be entirely effective in reducing decisional conflict among patients with CTS. Instead, they primarily enhance patients’ information levels compared to those who receive standard information from the clinicians. This requires an increased focus on patient-centred communication, as decision aids alone may not be sufficient to alleviate decisional conflict in these patients.
Further insights from Nam et al. 67 revealed that variations in preferences or experiences related to CTR decision-making do not significantly impact patient-reported outcomes. Instead, aligning decision-making experiences with patients’ preferences leads to better subjective outcomes after CTR surgery. This emphasises the importance of patient-centred communication by therapists, who should invest time in understanding patients’ preferences, exploring their experiences, managing expectations, and ensuring their desired level of involvement in decision-making. This patient-centred communication approach carries significant implications for therapists’ role in developing therapeutic alliances, utilising decision aids, and delivering patient-centred care, ultimately enhancing healthcare quality. 68
Future qualitative research should broaden its stakeholder base to include healthcare professionals, caregivers, and relevant organisations involved in decision-making around CTS. Such an approach would enable a comparative analysis of these stakeholders’ values and priorities with those of patients considering various treatment options.
Conclusions
This thematic synthesis of qualitative studies on patient decision-making in CTR reveals a nuanced process influenced by diverse expectations and factors such as symptom relief, treatment risks, and personal commitments. Decisional conflicts arise due to these complexities, shaped by social influences, past experiences, and communication with healthcare providers. The synthesis uncovers the unique role of individual experiences in decision-making and highlights multifaceted fears associated with surgery, including concerns about the procedure, complications, and rehabilitation, underscoring the intricate treatment dilemmas faced by CTS patients. By integrating these findings, therapists can personalise their interactions with patients, addressing the factors explored in the review, and ultimately improving patient care and decision-making outcomes.
Supplemental Material
Supplemental Material - Exploring patient perception of decision-making in carpal tunnel release surgery: A systematic review and thematic synthesis of qualitative studies
Supplemental Material for Exploring patient perception of decision-making in carpal tunnel release surgery: A systematic review and thematic synthesis of qualitative studies by Bing Chun Lui and Christina Jerosch-Herold in Hand Therapy
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
BCL is the Guarantor for the publication of this manuscript.
Contributorship
BCL designed the study, conducted the systematic review and thematic synthesis, interpreted the results, and drafted the manuscript. CJH contributed to the study design, provided guidance in the systematic review and thematic synthesis, and critically reviewed the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.