
Abstract
Background:
Rheumatic heart disease (RHD) is a potentially life-threatening condition that causes long-standing public health concerns. Echocardiography is a reliable diagnostic and screening technique for many cardiovascular conditions, including RHD. It is commonly used in tertiary care facilities worldwide but less so in the community setting. The primary aim of this study was to introduce and elaborate on the echocardiographic screening for RHD that was implemented by a Malaysian primary care clinic in Penampang district, Sabah. We also set out to present the uptake of the service in its initial years of establishment, as well as the challenges faced.
Methods:
In the first part of this study, document reviews were conducted to compile relevant information about the conceptualization and implementation of this service. Following that, we also obtained secondary data on the echocardiographic screening service from its first implementation in April 2020 until May 2021 to examine the uptake and the patient profile.
Results:
From April 2020 to May 2021, a total of 189 echocardiographic screening was conducted by primary care doctors using handheld ultrasound. Of the 189 children screened, 19 (10.1%) were found to have cardiac anomalies and were referred for a formal echocardiogram. Upon follow-up, 8 were detected with mild mitral regurgitation and referred to the nearest tertiary hospital for further management.
Conclusion:
Based on our review, the echocardiographic screening for RHD among children conducted by the Penampang Health Clinic was deemed successful. Echocardiogram service provided by primary care centers located in suburban and rural areas is highly beneficial for patients with poor access to specialized health care services because they stay far away from tertiary care facilities. Tapping into family medicine physicians located closer to communities to conduct echocardiographic screening and review the results can improve the detection of cardiac anomalies requiring further investigation. With the success of this project, echocardiographic services in the primary healthcare setting can be expanded by garnering the necessary collaborative efforts and consistent support from various stakeholders.
Keywords
Background
Rheumatic heart disease (RHD) is a potentially life-threatening condition caused by untreated acute rheumatic fever (ARF) as a result of group A streptococcal infections. 1 RHD is a significant and long-standing public health concern globally, with developing countries bearing the brunt of this disease due to suboptimal healthcare systems and a lower level of awareness about the condition. Between 1990 and 2019, there was a notable increase of 70.5% in the global prevalence of RHD, resulting in 40.5 million individuals with RHD by 2019 with a male preponderance. 2 According to the World Health Organization (WHO), around 319 400 people die from RHD every year, many of them being young individuals in their productive years. According to a systematic review by Noubiap et al, 3 the prevalence of RHD worldwide varies between countries due to the difference in diagnostic criteria and procedures. The prevalence of definite RHD ranged between 3.7% and 11.4% while the prevalence of borderline or probable RHD varied between 5.6% and 15.2%, depending on the diagnostic criteria used (World Health Organization and World Heart Federation). Locally, a RHD registry of a tertiary hospital in Sabah, Malaysia found that the west coast of Sabah recorded a higher prevalence of RHD, as half of the patients registered between 2010 and 2013 were from there. 4
Echocardiography (ECHO) is an essential diagnostic tool in the assessment of heart disorders. It creates a moving image of the heart using ultrasound waves to detect any abnormalities or anomalies of the heart. 5 ECHO relies on non-invasive ultrasound waves that do not cause any harm or pain. The evolution of portable echocardiographic equipment has dramatically increased the sensitivity of RHD screening. Besides providing rapid and reproducible results, it is also highly portable and convenient. Thus, the application of ECHO has been expanded beyond the confines of typical medical settings in hospitals.
The Malaysian Ministry of Health (MOH) offers a wide range of services that cover curative, promotive, preventive, and rehabilitative treatment. These services are provided by clinics, hospitals, and institutions specializing in long-term care. 6 Under the dual system of public-private healthcare providers, general practitioners (GP) clinics and hospitals in the private health sector commonly concentrate on the provision of curative care, especially in urban areas. Careful planning and investment to develop health professionals in the public and private sectors is imperative as they play a vital role in safeguarding, promoting, and restoring the health of populations. They must be well-equipped to respond effectively to the diverse and ever-changing health needs of the communities. Under the latest Malaysia plan (2021-2025), various strategies were outlined to safeguard universal access to quality healthcare services, one of which was the health human capital development to ensure an adequate supply of competent and skilled healthcare workers. 7 Human resource management must also be prioritized so that the healthcare personnel can deliver optimal services to the population.
In the past few decades, the field of public health has evolved to keep up with the latest changes. Following the Declaration of Alma-Ata 1979, many countries strive to strengthen primary care services. Primary care doctors are the main pillar of primary healthcare teams. They play a major role in encouraging community engagement via various methods such as providing media-based health education, training health volunteers or village health promoters, and acting as Clinic Health Advisory Panels at multiple service delivery points including Health Clinics, Rural Health Clinics, Mobile clinics, and schools. Furthermore, in the face of the non-communicable diseases (NCD) epidemic, primary prevention at the community level has been proven effective in preventing and reducing the incidence of NCD. Some of these primary care-related programs at the community level are often assumed to be too expensive for the healthcare system. Therefore, policymakers will be interested in knowing 2 key questions: How much does it cost? Is it an excellent value?8,9
The use of many scientifically proven and socially acceptable medical technologies is now progressively expanding beyond tertiary care facilities. 10 When applied by well-trained primary health care providers, certain medical devices can be used as screening tools in the general population to facilitate early detection and prompt management of certain conditions. In the field of cardiovascular diseases, ECHO is an effective screening instrument, particularly for patients with cardiovascular symptoms. 10 Conventionally, ECHO is predominantly offered in tertiary care facilities by cardiologists or ECHO technicians. ECHO screening for RHD is not a common provision under primary health care services in the community, be it in Malaysia or other countries. Primary care doctors would refer children suspected of RHD, that is, those with recurrent sore throats and abnormal findings during cardiac auscultation to tertiary hospitals with cardiology service for additional evaluation and therapeutic intervention. 11 However, many children in developing nations face significant challenges in obtaining prompt and suitable medical intervention, either due to socioeconomic factors such as poverty and limited educational attainment, or insufficient primary healthcare establishments with the capacity for early identification and ongoing disease management. This can result in loss of follow-up or delayed diagnosis, leading to avoidable morbidities like cardiac failure, cerebrovascular incidents, and endocarditis, as well as increased healthcare burden on the families and communities, and lastly, premature mortality.
Penampang is a district on the western coast of Sabah, Borneo Island. It spans an area of approximately 424.73 km2. The predominant ethnic group in the region is the Kadazan-Dusun while Chinese, Bajau, and other Bumiputras comprise the remaining populations. Penampang is geographically partitioned into urban, suburban, and rural regions. Around 70% of Penampang is classified as suburban and rural regions. The district of Penampang is divided into 8 sub-districts, namely Donggongon, Sugud, Bahang, Kepayan, Kobusak, Penampang Baru, Inobong, and Moyog. There are a total of 9 government health centers and 17 private clinics in Penampang.
In recent years, the provision of ECHO by skilled professionals in primary care clinics has been shown to facilitate timely intervention for RHD, subsequently minimizing the risk of patients failing to adhere to hospital referrals. The aim of this study was to introduce and elaborate on echocardiographic screening for RHD implemented by a Malaysian primary care clinic in the Penampang district of Sabah.
Methods
Primary care-based ECHO was launched at Penampang Health Clinic and expanded to 8 other government health clinics throughout the Penampang district over the period of 13 months. Figure 1 shows the flow of the screening protocol. Children between the ages of 5 and 18 years old, regardless of citizenship, were included while those with underlying RHD were excluded. All criteria were thoroughly checked by the nurses and doctors. Regardless of the eligibility criteria, all the routine outpatient follow-up was carried out as usual. A Liaison Officer was briefed regarding this project before being assigned to each clinic. Children who came for treatment, follow-up, immunization, or as companions were approached in the clinic waiting area either before or after their consultation. Parents or caretakers who consented to their children’s participation were briefed on this study. A data collection form was used to capture the following details: Name, Identification/Birth Certificate number, age, gender, education status, ethnic group, nationality, home address, school, as well as any history of medical illness.
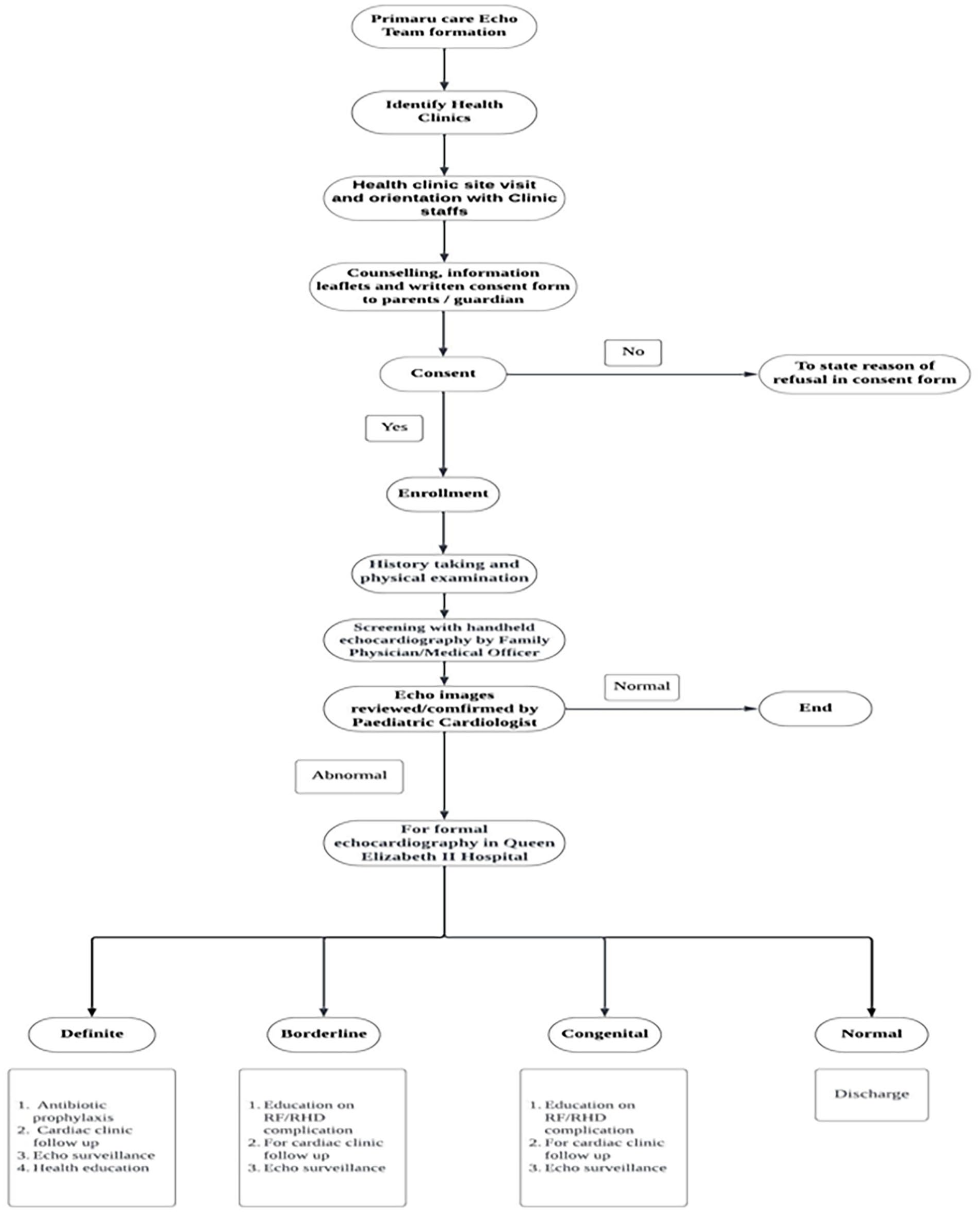
ECHO screening protocol in Penampang district of Sabah, Malaysia (adapted with World Heart Federation Criteria for Echocardiographic Diagnosis of Rheumatic Heart Disease 12 ).
The pilot study for this screening program took place at the Penampang Health Clinic, the largest primary care facility in Penampang. It is led by a Senior Family Physician and staffed by several other family physicians and medical officers to provide primary health care services to the local community members. For the purpose of this program, 2 medical professionals from Penampang Health Clinic (a senior family physician and a senior medical officer) underwent training on how to operate a handheld ECHO machine and interpret its results (Image 1). The training was given by a consultant pediatrician from the Pediatric Cardiology Department of the Sabah Women and Children’s Hospital. Parents were notified about the results of the ECHO. Those with abnormal ECHO would be counseled about the need for a referral to the cardiology department of Queen Elizabeth Hospital. In addition, we contacted parents who missed their ECHO appointment to further counsel them about the potential risks and complications of untreated RHD to ensure their compliance.

Medical officer (on the left) and senior family physician (on the right) of Penampang Health Clinic are being trained on ECHO by the consultant pediatric cardiologist.
Ethics of Study
The study complied with ethical principles outlined in the Declaration of Helsinki and the Malaysian Good Clinical Practice Guideline. Ethical approval was obtained from the Medical Research and Ethics Committee (MREC), Ministry of Health Malaysia (NMRR-21-681-59540). Informed consent was obtained from both parents and researchers for this publication.
Statistical Analysis
Statistical Package for Social Sciences (SPSS) 28.0 was used to analyze the data. All data were described using univariate descriptive statistics and frequency distributions.
Results
A total of 189 out of the 196 children approached in the clinics were screened, giving a response rate of 96.4%. The mean age (SD) of the participants was 9.3 (2.90) years old, with more than half of them being male (52.9%) and almost of them being Malaysian (98.4%) (Table 1). Most of the screened children resided in the urban and suburban areas of Penampang (63.5%). Children from the rural areas were offered the Echo screening by the respective rural clinics in their area. None of the screened children had a documented history of congenital heart disease. During auscultation, 3 children were found to have a murmur. Out of the 189 children screened, 19 (10.1%) were found to have abnormal Echo findings by the primary care doctors. All were referred to a tertiary center for further assessment. Of the 19 children, 12 were seen at the pediatric cardiology department of Queen Elizabeth Hospital while 7 defaulted follow-ups. Eight of the 12 children were diagnosed with definite RHD (with Mitral Regurgitation) and given monthly IM Benzathine Penicillin and follow-up appointments. Two children had borderline RHD (one had trivial Aortic Regurgitation, and one had Trivial Tricuspid Valve/ Pulmonic Regurgitation), whereas the remaining 2 showed regular Echo findings. Those with borderline RHD were given an annual Echo screening appointment.
Sociodemographic Characteristics, Auscultation, and Echocardiographic Findings of Respondents (n = 189).

Discussion
Primary care is an approach that prioritizes individuals’ overall health rather than just treating specific diseases. It considers all the factors that contribute to a person’s well-being and offers preventive, curative, and rehabilitative services to address the most pressing concerns in the community. As a result, primary care serves as an important foundation of all other levels of healthcare systems. Screening should be incorporated as part of a preventive program and expanded to primary care centers to make it more accessible for the community. In the case of RHD, the key to reducing premature mortality and morbidity related to RHD is early detection and prompt management through an empowered health system. Our study demonstrated that Echo screening in community settings is feasible and relatively simple to implement. Healthcare facilities should provide Echo screening as it is superior in detecting RHD compared to auscultation. Ploutz et al 13 discovered that non-specialists’ use of handheld ultrasound as part of a community-based Echo screening program in Uganda demonstrated relatively higher sensitivity and specificity in detecting both borderline and definite cases of RHD.
Studies conducted in countries with limited resources, particularly in parts of Africa and Asia, have shown that portable Echo devices are highly effective. 14 These studies highlight the importance of Echo screenings in areas where RHD (Rheumatic Heart Disease) is still prevalent due to socio-economic factors. The literature suggests that non-specialist healthcare workers, such as primary care nurses and general practitioners, can be trained effectively to perform Echo screenings. Decentralizing RHD screening through this approach can make it more accessible for people in need.
Our project aimed to replicate a similar study in Sabah. We believe that this is an essential step in improving the detection and management of RHD. Tertiary facilities frequently manage complicated RHD cases at an advanced stage that require specialized care and prolonged hospital stays. 15 Identifying and managing cases earlier at the primary care level can reduce the number of severe cases that require tertiary care. Thus, expanding screening to the primary care setting can reduce the diagnostic and treatment burden of RHD on tertiary facilities. By doing so, extra capacity and resources can be freed up for other patients in need. It also decreases the long-term costs associated with advanced RHD treatment, such as surgeries, prolonged hospital stays, and complications.
Malaysia has a wide coverage of primary care services. They are readily available to everyone, regardless of socioeconomic background. Primary care personnel such as doctors and nurses are often the first point of contact for individuals and families. In the case of RHD, an untreated streptococcal throat infection often causes RHD. Penicillin has been proven as an effective form of primary prevention. It is easily accessible and affordable in most parts of the world. Studies have shown that benzathine penicillin G injections successfully treat streptococcal infections. 16 Therefore, the administration of benzathine penicillin G injections can prevent the onset of rheumatic fever and subsequently RHD.
Sustainability of the Program
Regardless of whether communicable diseases or NCDs, community awareness is a crucial ingredient in the aspect of prevention. Every individual should be educated on the significance of health, rather than just as a part of primary disease prevention or in the event of a disease outbreak. 17 With regard to RHD, early childhood is a crucial time for the intervention needed to reduce disability-adjusted life years (DALYs) associated with RHD.
For the betterment of the communities and optimal use of healthcare resources, it is crucial to ensure the sustainability of any primary care programs. Our project has successfully demonstrated that primary care doctors can be trained by experts from tertiary centers to perform Echo. Therefore, our primary care-based Echo screening can be expanded to other regions, states, or even countries. However, to ensure competency, it is crucial to provide regular supervision and training. Field supervisors must be appointed to ensure direct supervision and to conduct performance evaluations as part of staff appraisal. A safe and healthy working environment is crucial in providing a conducive atmosphere for healthcare workers. 18
Implementing screening programs, such as our proposed RHD Echo screening, is a complex and multifaceted task. It involves economic costs, legislative frameworks, community activities, and environmental considerations, all critical to the program’s sustainability and success. Most important of all, continuous assistance and support from MOH stakeholders are imperative. Such support would enable the program’s expansion to other regions within Malaysia.
Addressing Health Disparities Towards Achieving the Universal Health Coverage
The primary objective of Universal Health Coverage (UHC) is to guarantee that every individual and community has good access to all the necessary health services without experiencing undue financial burden. 19 To achieve UHC, it is essential to recognize and address existing health inequalities within and between countries. One key strategy to mitigate these disparities and move toward UHC is the implementation of community-based health screening. 20 Community-based health screening programs have been shown to effectively reduce health disparities caused by socio-economic and environmental factors, leading to better health outcomes for marginalized populations. This community Echo screening program was customized to be culturally sensitive to address the linguistic and social needs of the community in Penampang to ensure greater engagement and relevance.
Apart from opportunistic screening tests, health events at the community level also provide an avenue to educate community members on various health concerns, preventive measures, and to remind them of the significance of attending regular health check-ups and screening tests such as pap smears, Clinical Breast Examination (CBE), the fecal immunochemical test (iFOBT) etc.21,22 The Mobile Health Clinic is another example of reaching out to the community. In this study, we showed that the mobile health team in Penampang can easily carry out portable Echo screening for RHD and even transmit real-time images to specialists or cardiologists for review. Compared to communicable disease control during outbreaks or pandemics, the prevention and screening efforts of RHD are not emphasized enough. 23 By instilling health-related knowledge and resources to community members, individuals can be empowered to take responsibility for their health and adopt healthy lifestyle measures to enhance it. An empowered community is more likely to engage in health-promoting behaviors to adopt an active role in improving overall well-being. 24 By tapping into local capacity, community health workers can play an inclusive role in the screening program. By involving community members in the process, trust is built and more people are willing to participate in health programs and comply with recommended treatments. Following the COVID-19 pandemic, major advancements have taken place in the field of information and communication technologies (ICT). Many health promotion activities are now easily accessible via mobile devices and computers. Based on recent studies, approximately 90% of Malaysians actively engage in social media activities and maintain various accounts on these platforms. 25 The Mobile Health Clinic can easily carry out portable echocardiographic screening, immediately transmitting images to a nearby specialist or cardiologist for review.
Extensive research carried out in low- and middle-income countries (LMICs) has demonstrated the effectiveness of community-based health screening programs. A systematic review comprising of 167 studies from 33 LMICs, including countries such as Ethiopia and India, highlighted the success of these programs. 26 The studies demonstrated the significant role played by community health workers in improving health equity by reaching out to marginalized populations and addressing various health disparities. The success of these programs in LMICs underscores the potential of community-based health interventions to enhance health outcomes in resource-limited settings.
Role of the Community Health Volunteers
More importantly, community members should be incorporated as volunteers in the planning and execution of health programs to build a stronger trust between healthcare personnel and the local population. In this study, a situational assessment was undertaken to better understand the healthcare needs of the Penampang population before deploying the best strategies for the community-based Echo screening program. We found that community health volunteers are crucial in reaching out and engaging with rural populations in remote and underserved areas. Studies have shown that involving Community Health Workers (CHWs) in health interventions can effectively increase health screening rates. A systematic review has highlighted that interventions which engage community health volunteers have led to significant increases in cancer screening rates for cancers. 27 These interventions have been found to be effective for individuals from all sociodemographic backgrounds. The health promotion team can collaborate with community health volunteers to disseminate the necessary awareness and information regarding any ongoing health program. Nutbeam and Muscat 28 defines health communication as a comprehensive range of activities encompassing both interpersonal and mass communication, with the primary objective of enhancing the health outcomes of individuals and communities. In recent years, advancements in ICT have facilitated health communication. 29 By conducting conventional health education activities using multi-media ICT, better and wider dissemination of messages and information can be achieved. These technological improvements enable individuals and populations to acquire health information more comfortably at their fingertips. Furthermore, individuals can receive objective assessments about their well-being due to the wide availability of health-related information.
We believe that our project represents the first step forward in community Echo screening for RHD. Ongoing advocacy efforts involving collaboration between district health and education officials, village headmen, local radio/television stations, private health facilities, and non-government organizations are crucial to expanding and sustaining this program. By disseminating pertinent details about this program via electronic media platforms and local communication channels such as radio announcements and infographic posters shared on Facebook, we can spread awareness about this condition and its relevant management to a broader audience. In this program, an information session was conducted during the Parent-Teacher Association meeting as part of the lobbying efforts. Additional community engagements were also performed across various entities, including private clinics, information departments, district education and dental offices, as well as police stations.
Challenges and Limitation
Despite its strengths and benefits, there are some limitations to this program. Firstly, limited funding and resources (equipment and personnel) are the main challenges in ensuring the sustainability of this program. Continuous support from various stakeholders, including MOH and the State Health Department is vital. More importantly, the identification and diagnosis of RHD are not sufficient. It should be complemented by an efficient mechanism for subsequent management and treatment. A seamless flow of follow-up procedures can improve adherence to follow-ups at tertiary centers. Last but not least, data collection was limited to primary and essential information due to the lockdown during the COVID-19 pandemic. A more comprehensive data collection in future projects can provide a more in-depth analysis of the incidence and risk factors of RHD in the community.
Conclusion
This community-based Echo screening pilot project for RHD represents a good start to address neglected health concerns in the community in the progress toward UHC. Community-based screening programs can increase healthcare access for marginalized communities and reduce any disparities, with the aim of achieving health equity. To ensure the sustainability of community screening programs, commitment and collaboration from healthcare providers and community health volunteers are imperative.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.