
Abstract
Objectives:
To determine the prevalence and contributing factors of depression and suicidal ideations among stroke survivors in Nigeria.
Methods:
This was a cross-sectional study comprising 75 consenting stroke survivors who were purposively recruited from 2 tertiary hospitals. Suicidal ideations and depression were measured using standard questionnaires. Obtained data was analyzed with appropriate statistical tools.
Results:
9.3% of the participants had depression while 4% reported suicidal ideations. Significant correlation existed between suicidal ideations and depression (ρ = .31, P = .01), and levels of depression and suicidal ideations (χ2 = 85.76; P < .01). Depression had a significant relationship with gender and marital status, while suicidal ideations had a significant relationship with marital status. Females were significantly more depressed than their male counterparts (U = 512.50, P = .04) and also had a higher score on suicidal ideations. The widowed/divorced recorded the highest scores on depression (χ2 = 8.77, P = .01) and suicidal ideations (χ2 = 6.62; P = .04).
Conclusion:
A worrisome prevalence of depression was reported among the study participants. The level of suicidal ideations was quite low. Depression and suicidal ideations were higher among females and those who lost their life partners (either by divorce or death).
Introduction
Stroke remains the major cause of severe, long-term neurologic impairment and functional disability. 1 It is projected that the burden of stroke will increase in sub-Saharan Africa in the next few decades due to epidemiological transition. 2 This reveals the high disability adjusted life years (DALYs) in sub-Saharan Africa which is approximately sevenfold higher than in developed countries. 3 Stroke and psychological stress such as depression are considered major contributors when it comes to total years lost to disability based on the global burden of diseases (GBD) report; and as such, if stroke is associated with emotional disorders such as depression, it is regarded as double burden of stroke. 4 It is associated with poor functional, psycho-social outcome and dependence when considering activities of daily living, and to the severity of neurological deficits. 5
Emotional disorders after stroke greatly contribute to the global burden of disease 6 and are consistently linked with poor psychosocial outcomes and increased mortality affecting people in all communities across the world.7,8 Some diseases of the vascular system like stroke have identifiable contributions to psychiatric co-morbidities. 9 Direct damage in the brain or maladaptive reactions to stroke incidence could be the cause of mental health problems manifesting after stroke. 10 In any of the cases, relationship between the personality makeup of the individual and adverse life situations often has an impact on how survivors adjust to disability and in turn influences the rehabilitation and recovery process. 11 Common mental health problems that manifest after stroke include anxiety, depression, personality changes and psychotic disorders. 12
Depression is a common mental disorder usually characterized by distorted mood, loss of interest or pleasure, sadness, feeling of guilt or low self-worth, disturbed sleep or appetite, low energy, and so on.13,14 Depression often affects patients’ participation in the rehabilitation process and has negative impact on functional recovery, community reintegration and long term outcomes.15,16 Most often, depressed individuals develop suicidal thoughts and ideations with the hope of finding a lasting end to their challenge. 17
Suicidal ideation is a collective continuum that includes thinking about ending one’s own life, developing a plan, unsuccessfully attempting suicide and ending one’s life. 18 It is the thought of intentionally trying to cause one’s own death by any means; ranging from passive thoughts to ideas with elaborate plans and goals of committing suicide. Studies have reported higher rates of suicide ideation, suicide attempts, and completed suicides among stroke patients than in the general population.12,17
Despite the important understanding of negative psychosocial sequelae of stroke, there is a scarcity of studies on suicidal ideations among stroke survivors in low/middle-income countries especially Nigeria. This present study was aimed at determining the prevalence and relationship between depression and suicidal ideations, and their relationship with gender and marital status among stroke survivors in Enugu state, Nigeria. It is hoped that this study will provide information/data to guide health theory, policy, and practice as it concerns the studied variables in the rehabilitation of stroke survivors.
Methods
This was a cross-sectional study involving 75 stroke survivors (aged 18 years and above) who were purposively recruited from follow-up neurology unit and physiotherapy departments of 2 tertiary hospitals in Enugu state, Nigeria. One of them has been reported to be the largest tertiary institution in the South-east of Nigeria providing specialist care as well as training of other specialties.19,20 The other serves an estimated six million people of Enugu as well as its neighboring states. It fulfills a dual purpose of both a general and a teaching hospital, and as well has an unrestricted admission policy. 21 Thus, both locations were selected because they adequately represent the population of this study, being the largest institutions that are more likely to have a greater proportion of stroke survivors. 19
Stroke diagnosis was ascertained from participants’ hospital case folders. Inclusion criteria were stroke survivors with either first-ever or recurrent stroke. Participants were excluded if they had history of any central nervous system disease other than stroke, severe auditory or visual impairment, as well as record of any psychiatric disorders before the stroke. Ethical approval was obtained from the Health Research Ethics Committees of both institutions. Participants gave verbal or written informed consent (depending on the area/severity of affectation, and level of literacy) after the whole procedure had been thoroughly explained to them and their confidentiality assured. A sample size of 75 was calculated from a population of 92 stroke survivors using a 95% confidence level and 5% margin of error.
Beck’s depression inventory (BDI) was used to measure depression. The BDI is a 21-item self-report multiple choice questionnaire assessing mood, pessimism, and sense of failure, self-dissatisfaction, guilt, punishment, self-dislike, self-accusation, social withdrawal, work difficulties, insomnia etc. The items were scored on a scale of 0 to 3; “0” stands for when you strongly disagree and “3” for when you strongly agree. The total score ranges between 0 and 63, with 0 being the minimum (no depression) and 63 being the maximum (severe depression). Scores of 0 to 10 are considered normal; 11 to 16 mild mood disturbances; 17 to 20: borderline clinical depression; 21 to 30 moderate depression; >30 severe depression. “Normal” is characterized by negligible ups and downs in emotions; has no form or significant disturbance in mood. “Mild mood disturbance” is characterized by a low mood and other symptoms of depression, but the symptoms will be less intense. “Borderline clinical depression” is a mild mental health disorder that impacts the way one thinks and feels about self and others; includes self-image issues, difficulty managing emotions and behavior, and a pattern of unstable relationships. “Moderate depression” is characterized by persistent low mood, fatigue, difficulty concentrating, decreased interest in activities and productivity, etc. “Severe depression” is a major depression which may interfere with one’s daily life and potentially lead to suicidal ideation. The symptoms are severe and noticeable even to person’s loved ones. The BDI has a correlation coefficient of .86 and Spearman-Brown correlation coefficient of .93 from internal consistency studies conducted for the test items. 22
Beck Scale for Suicide Ideation (BSSI) was used to measure suicide ideations. The BSSI is a 19-item instrument which determines the current intensity of specific attitudes, behaviors, as well as plans to commit suicide. Scoring of the tool entails that for additional items to be administered to a participant, he/she would get a score of 1 or above for at least one of the first 5 items. If the participant does not get any score for the first 5 items, the total score will be zero (no ideation). With respect of this scoring method, the distribution of scores typically includes many zeroes (for non-ideators) and a more parametric distribution of scores for those who are involved in suicidal thinking. 23 Each item is made up of 3 choices (ranges from 0 to 2), with a total score ranging from 0 to 38. BSSI relatively has a very high internal consistency, with 84 to 89 percent Chronbach’s alpha. 24
The socio-demographic information of the participants such as age, marital status, gender, level of education was obtained through oral interview. The response rate of the survey was 96%. Data obtained was analyzed using SPSS version 20; using descriptive statistics of frequency and percentage to summarize the participants’ socio-demographic variables. Spearman Rank Correlation was used to assess the relationship between total scores of depression and suicidal ideations. Chi-square was used to test the association between the levels of depression and suicidal ideations. Mann whitney U test was used to test the difference between each of depression and suicidal ideations with the participants’ gender. Kruskal Wallis H was used to test the difference between each of depression and suicide ideations with participants’ marital status. Level of significance was set at P < .05.
Results
A total number of 75 stroke survivors (aged 18 years and above) undergoing rehabilitation in the 2 teaching hospitals participated in this study. Majority of the participants (56%) were older adults, 53.3% were male. Sixty-eight percent were married, 64% had at least a secondary education, 54.7% were self-employed (Table 1). About 9.3% of the participants reported depression and 4.0% had suicidal ideations (Table 2). There was a significant association between levels of depression and suicidal ideations, with mild mood disturbance and moderate depression having suicidal thoughts; and severe depression having suicidal behavior (χ2 = 85.76; P < .01) (Table 3).
Socio-Demographic Profile of Participants.
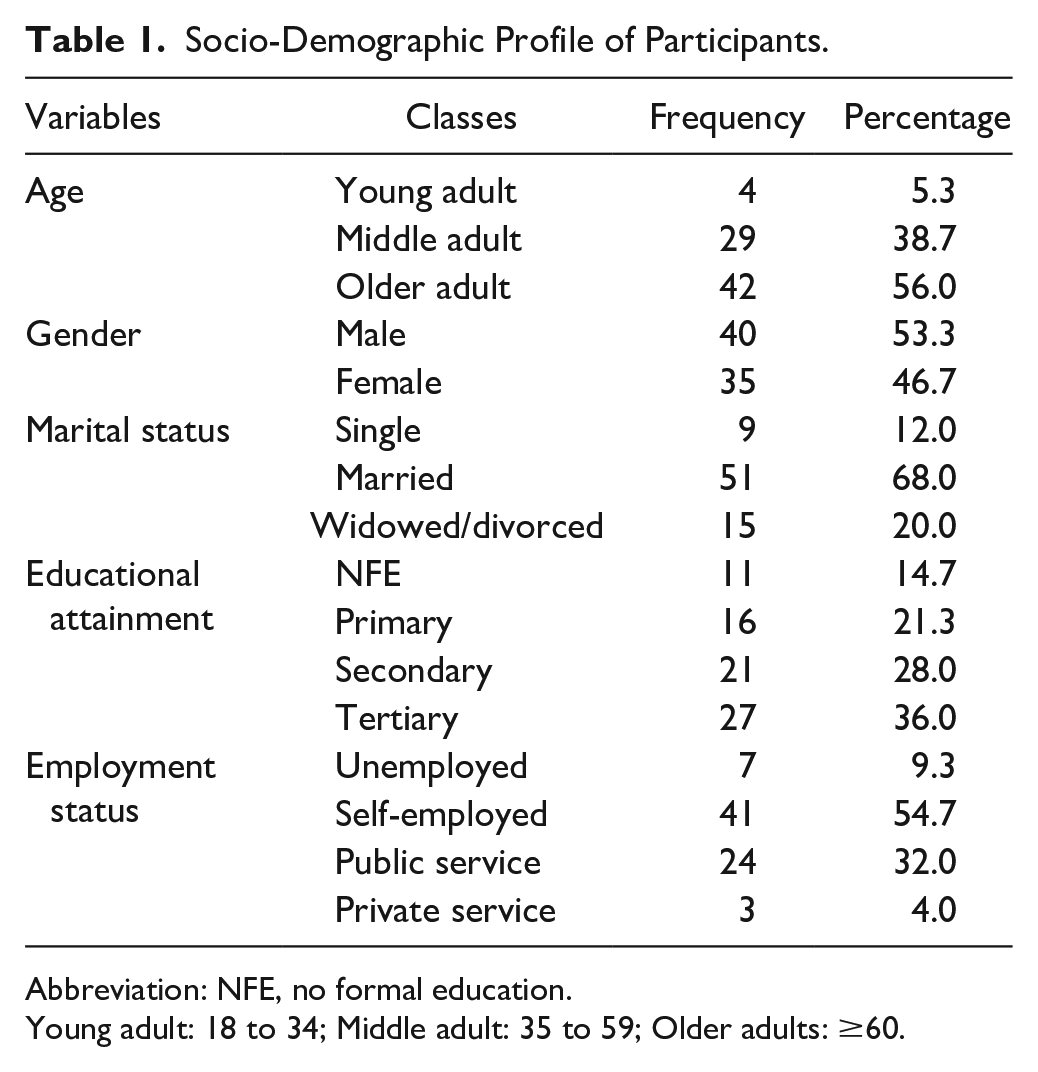
Abbreviation: NFE, no formal education.
Young adult: 18 to 34; Middle adult: 35 to 59; Older adults: ≥60.
Distribution of Proportions of Participants on Suicidal Ideations and Depression.

Abbreviation: MMD, mild mood disturbance.
Chi-Square Test Showing the Association Between Levels of Depression and Suicidal Ideations.

Abbreviations: No suic idea, no suicidal ideations; Suic thoughts, suicidal thoughts; Suic behav, suicidal behavior; Mild M D, mild mood disturbance.
Indicates significance at 0.05.
There was a significant difference between marital status and depression (χ2 = 8.77, P = .01), with the widowed/divorced having the highest score on depression. Females were significantly more depressed than their male counterparts (U = 512.50, P = .04) (Table 4). There was also a significant difference between marital status and suicidal ideations (χ2 = 6.62; P = .04), with the widowed/divorced having the highest score on suicidal ideations. Females also had a higher score on suicidal ideations (Table 5). There was a weak but significant correlation between suicidal ideations and depression (ρ = .31, P = .01).
Mann Whitney U and Kruskal Wallis Tests Showing the Influence of Gender and Marital Status Respectively on Depression.

Abbreviations: U, Mann Whitney U test value; P, significance value; χ2, Kruskal Wallis test value.
Indicates significance at 0.05.
Mann Whitney U and Kruskal Wallis Tests Showing the Influence of Gender and Marital Status Respectively on Suicidal Ideations.

Abbreviations: U, Mann Whitney U test value; P, significance value; χ2, Kruskal Wallis test value.
Indicates significance at 0.05.
Discussion
This study explored the prevalence of depression and suicidal ideations, their interconnections, and relationships with gender and marital status among stroke survivors.
The findings of this study revealed a worrisome 9.3% prevalence of depression among stroke survivors. Previous studies have reported a prevalence of 22.9%among post-stroke patients attending an out-patient hospital in Nigeria using structured interview 9 ; and a prevalence of 41.6% was reported while using BSI-II. 25 A prevalence of 45% had been reported among older adults from a healthy population, 13 thus, necessitating the validation of the geriatric depression scale for use amongst this population. 26 Stroke patients might exhibit high intolerance of their disability and uneasiness to cope with the challenge, thus, the tendency to experience lots of psychological problems such as depression. 25 Evidence shows that depression is a common complication of stroke, resulting in high morbidity and mortality, 27 and approximately 40% to 50% of patients experience depression. 28 Reactions resulting from depression such as a feeling of worthlessness, loss of interest or pleasure, and low self-esteem are common among stroke survivors, particularly as they try to handle the sudden interruption and new experience of living with a stroke that is often frightening and wrongly perceived. 9
The 4% prevalence of suicidal ideations reported in this study is lower than rates of between 7.8% and 11.8% reported in global studies, which are mostly from high-income countries.29,30 It is also lower than the findings reported in a previous study from southwest Nigeria, in which nearly 1 of every 6 participants had suicidal thoughts. 31 The actual reason for the increased risk of suicide after stroke remains unclear.31,32 Nonetheless, the risk of suicidal ideations in the background of depression reported in this present study is sequel to the results of a recent meta-analysis of 9 studies which revealed that the strongest systematic correlate of post-stroke suicidality is depression. 32 Results of this present study also fit within common models of the pathways to suicide33 -35 such as the interpersonal theory of suicide, which supports why death by suicide is relatively small. According to the theory, the concurrent occurrence of all 3 necessary conditions (perceived burdensomeness, thwarted belongingness, and the acquired capability that can result to being involved in lethal self-injury) is experienced only by a small group of individuals. 36 In clarifying the various ideas of consideration, suicide occurs on the path from depression to real suicidal thoughts, plans, attempts/ behaviors, and completed suicide.37,38
Depression was significantly associated with suicidal ideations in this present study. Studies have shown that stroke survivors who develop suicidal thoughts once experienced depression. 39 Moments of increased hopelessness, anxiety, and worries associated with depression are what give birth to suicidal thoughts and behaviors. Sequel to previous studies on suicide in the US, about 3.4% of people with major depression commit suicide in the United States, and up to 60% of people who commit suicide have depression or related mood disorder. 39 This evidence is supported by the findings of this study which revealed that participants with no depressive symptoms had no suicidal ideation; whereas, the ones with severe depression reported suicidal behavior. Interestingly, mild mood disturbance and moderate depression were both associated with suicidal thoughts and not behavior, showing that higher depressive symptoms may lead to an increased possibility of suicide. Initial studies have reported higher rates of suicide ideation, suicide attempts, and completed suicides among stroke patients than in the general population.12,17 Stroke incidence does not only increase the risk of suicidal thoughts but also the risk of suicide.40,41 Ekechukwu et al 42 reported that the observed differences in motor function, balance, depression, self-esteem, and self efficacy between stroke survivors and the matched subjects are corroborative pointers that the physical and psychological impairments seen among stroke survivors are not primarily due to aging but are sequela of stroke pathology.
Results from this study showed that there was a significant difference between depression and each of gender and marital status; and that stroke survivors who are females experienced more depressive symptoms compared to their male counterparts. This corresponds with the findings of previous studies which revealed gender-based differences in stroke outcomes, and involving daily activity independence and quality of life. 43 Having lower independence in daily activities and as well, poorer physical, cognitive, and emotional functioning after discharge was seen to be highly prevalent among female stroke patients than male stroke patients. 44
The majority of the participants of this study who experienced symptoms of depression have separated marriages (either through divorce or death). This finding corresponds with previous studies that investigated the relationships between post-stroke depressive symptoms and various demographic characteristics including; gender, age, educational level, income status, and the presence of a spouse; and revealed that depressive symptoms of women living with a spouse were lower compared to those without a spouse. 45 Since spouses are the primary caregivers, and a great number of patients are physically dependent on others, 46 it becomes meaningful to assume that there are partner-dependent effects on emotional functioning. Similar outcomes from other studies show that there is a negative correlation between depressive symptoms and social support. 47 Thus, it suggests that stroke survivors without a spouse might be more depressed compared to individuals with spouses.
This study showed no significant association between suicidal ideations and gender. This implies that being a male or female does not directly influence the risk of suicidal ideations among stroke survivors, rather it possibly depends on the level of thwarted belongingness and feelings of burdensomeness as explained by the interpersonal theory of suicide. A previous study that categorized the factors increasing suicidal ideation with gender differences among community-dwelling stroke survivors found that suicidal ideation was more common in those who were widowed, rather than married, those who rarely contacted neighbors, current smokers, and frequent drinkers among male stroke patients. On the other hand, being old, having lower monthly household incomes, being unemployed or who were housewives/students, those with low social contacts, and diabetics results in higher level of suicidal ideation among female stroke patients. 48
Furthermore, the findings of this study revealed a significant relationship between suicidal ideations and marital status. This is in line with the outcome of previous studies which have observed a significant association between marital status and the risk of suicide among stroke survivors. A recent meta-analysis revealed that stroke survivors who were married were less at risk of suicidal ideation. 32 Kim and Lee 48 in their study found that widowed males were more likely than married males to exhibit suicidal ideation, whereas, no significant relationship was observed between marital status and suicidal ideation among the female participants. Why only widowed males who have had strokes show greater level of suicidal ideation remains vague to explain. However, a possible reason might be the impact of bereavement which differs between genders. A previous study on healthy populations identified that marriage can be seen as a protective factor against suicidal ideations. 49 There were more likely reports of suicidal ideation among individuals who were not married—thus, live alone, contrary to those who have family support. 50 Similar findings from previous studies showed a significant association between living alone and developing suicidal ideation. 50 In comparison to individuals with other marital statuses, married individuals have lower levels of completed suicide. 51 In stressful events, married couples can provide support to each other 52 ; and the risk for suicide mortality can be lowered by helping each other or being responsible toward a spouse. 51 Compared to unmarried individuals, protection against suicidal thoughts could be a result of married individuals being more integrated into a bigger supportive network. 53 In contrast to the outcome of this study, a previous study on marital status and burdensomeness as risk factors of suicide ideation in post-stroke patients, suggests that marital status does not protect nor is a risk factor for suicide ideation among stroke survivors. 54 This may largely be due to the idea that stroke survivors with spouses who have low burdensomeness might get protection against suicidal ideation through marriage, whereas individuals with spouses who developed high levels of burdensomeness tend to see marriage as a risk factor. Thus, the effect of marriage on suicide may be neutralized by the two opposing effects. Battling with physical disabilities and inabilities which make stroke survivors dependent on their loved ones for activities of daily living such as bathing and eating could be a major post-stroke challenge.
Limitations
This study was clinic-based, thereby excluding stroke survivors living in core rural areas with little or no access to hospital settings; and therefore might affect the generalizability of the present results. Another limitation is the small sample size. The cross-sectional design of the study also did not allow the determination of direction of causality, and findings were only reported based on observed relationships, and should thus be interpreted with caution.
Conclusion
There was a worrisome prevalence of depression among the study participants, and suicidal ideation was low. There was a significant relationship between depression and suicidal ideations among the participants; with females and those who lost their life partners (either through divorce or death) having higher scores on depression and suicidal ideations. Equal priority should be given to both the medical and psychosocial aspects of stroke management and rehabilitation. Future research should seek to recruit a more diverse population of participants from the core rural areas who might not have the access to tertiary hospitals, for more insight into different factors affecting the day to day living and independence in the population of stroke survivors.
Footnotes
Acknowledgements
We thank our participants for being part of this study
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from the Health Research Ethics Committee of UNTH, Ituku-Ozalla-Enugu (NHREC/05/01/2008B-FWA00002458-1RB00002323) and also, from the Ethical Committee of ESUT Teaching Hospital Parklane-Enugu.