
Abstract
Background
Medical training from undergraduate to residency shows high rates of depression and suicidal ideation in students. These findings have been associated with excessive hours worked, little sleep, fatigue, and stress, with a higher possibility of making medical errors and committing suicide within the following year.
Objective
To determine the prevalence of depression and suicidal ideation in family medicine residents.
Methods
Multicenter, cross-sectional, and exploratory study in resident physicians from 18 states of Mexico. A four-part questionnaire was sent: sociodemographic characteristics, experiences during medical residency, “Patient Health Questionnaire-9” (PHQ-9), and personal and family history.
Results
It was reported that 14.3% of resident physicians have moderately severe and severe depression. However, when including the subgroups of physicians who also present mild to mild-moderate depression, the prevalence increases to 59.7%. 16.7% of residents reported having had thoughts of death, and 7.9% reported one or more suicide attempts.
Conclusions
The prevalence of depression in family medicine residents is present in three out of five residents, and although suicidal ideation is also high, it is very worrying that almost 8% of the subjects had already attempted suicide, between one and three times higher than reported in another research.
Introduction
Depression is a mood disorder characterized by feelings of sadness, loss of interest, guilt, sleep disturbances, appetite, fatigue, lack of concentration, and/or inability to experience pleasure associated with daily life events (McCarron et al., 2021; PAHO/WHO, 2021). The WHO reported in 2021 that 3.8% of the world’s population suffered from this disease, similarly, the Institute for Health Metrics and Evaluation (GHDx) reported that approximately 280 million people worldwide suffered from depression in 2023 (Institute for Health Metrics and Evaluation (GHDx), 2023). In Mexico, the National Survey of Self-Reported Well-Being (ENBIARE) found that the general population with symptoms of depression was 15.4%, being more frequent in women (19.5%) than in men (10.7%) (Instituto Nacional de Estadística y Geografía & Encuesta Nacional de Bienestar Autorreportado, 2021). It is estimated that 8.5% of life years are lost due to this disease (Gómez-Dantés et al., 2016). In 2011, it was the leading cause of disability and years of productive life lost globally (Gore et al., 2011).
Depression is one of the most common psychiatric problems in the world and is also known as major depression, major depressive disorder, or clinical depression (National Institute of Mental Health [NIMH], 2023). Its symptoms must last at least 2 weeks. According to the American Psychiatric Association (APA, 2023), one in six people may suffer from this disease at some point in their life.
The origins of depression are multifactorial, involving various contributing factors. These include alterations in the regulation of brain neurotransmitters, such as serotonin (Lesch et al., 1996; Rot et al., 2009); genetic predisposition; environmental influences; individual personality traits, particularly in people with low self-esteem (APA, 2023); and exposure to chronic stress (Firk & Markus, 2007; Miller & Raison, 2016; Pérez-Padilla et al., 2017; Ramírez et al., 2018). A clear example of chronic stress exposure is the medical field, where professionals routinely face adverse circumstances. Depression and suicidal ideation rates are already alarmingly high in medical training programs at the undergraduate level (Betiati et al., 2019). In a meta-analysis that included medical students from 47 countries, Rotenstein et al. (2016) found that in 43 of them, the students had depression or depressive symptoms with prevalences ranging from 27.2% to 35.6%.
Depression is approximately 10% more prevalent among medical professionals compared to the general population, with higher rates observed in women (Garza-Rincones et al., 2018). This increase is linked to risk factors inherent in the demanding nature of medical residency. The residency period is marked by significant stress from various sources, including academic, economic, administrative, personal, psychological, physical, legal, and social challenges, testing residents’ resilience and coping abilities (Reyes et al., 2023).
Studies have consistently documented the negative impact of these factors on residents’ mental health, including symptoms of depression, anxiety, physical exhaustion, and burnout syndrome. Burnout, in particular, has been reported at alarmingly high levels, with prevalence rates of up to 63% for emotional exhaustion and depersonalization (Ishikawa, 2022; Jaulin et al., 2021; Levy et al., 2019; Pasqualucci et al., 2019).
In a systematic review that included almost 20,000 subjects, developed between 1963 and 2015, regarding depressive symptoms and suicidal ideation in resident physicians of different specialties, an average prevalence of 28.8% was found, with a range, according to the assessment tool used, from 20.9% to 43.2%. Furthermore, in a second systematic analysis, it was concluded that the first year of residency can cause an increase of up to 15.8% in depressive symptoms, regardless of the specialty or country (Mata et al., 2015). These findings are concerning because the presence of depression and suicidal thoughts has been associated with the possibility of committing suicide within the subsequent year (Rotenstein et al., 2016).
Finally, the presence of depressive symptoms, excessive hours worked, short sleep, fatigue, and stress has been associated with evidence of a greater possibility of medical errors (Kwok, 2021; Levy et al., 2019; West et al., 2009).
Therefore, it is essential to recognize and treat depression in medical residents, in this case, in family medicine, not only because of the risks to their health and quality of life but also because of the risks of patients suffering from malpractice. In addition, it is essential to mention that this research corresponds to the initial pilot study of the project “Prevalence of Depression and Suicidal Ideation in the Postgraduate Program of the Faculty” whose number of residents is more significant than 16,000, in 82 specialties. The objective of the present study was to determine the prevalence of depression and suicidal ideation in family medicine resident physicians in 18 states of the Mexican Republic.
Material and Methods
This multicenter, cross-sectional, exploratory study was conducted among family practice medical residents enrolled in any academic year, from 18 states across the Mexican Republic. Four health care institutions recruited participants using a nonprobabilistic convenience sampling method facilitated by their professors and state scientific societies.
Instrument
Residents were invited to answer a 30-question questionnaire uploaded to Google Forms, sent via email and WhatsApp, which consisted of four parts: sociodemographic characteristics, experiences during medical residency; the third corresponds to the “Patient Health Questionnaire-9” (PHQ-9). The PHQ-9 has nine questions to screen for depressive symptoms in the last two weeks. Those who obtained a score greater than 15 were considered to have moderate to severe depression. Students who answered question 9 affirmatively, “Thoughts that I would be better off dead or of hurting myself” were considered to have suicidal ideation and major depression, in which case their teachers would be informed so that they could provide the corresponding help through their institutions. Scores below 15 were not considered since, according to the PHQ-9, they correspond to patients without depression and mild or moderate depression. The last part of the questionnaire included personal and family history. Five graduate professors validated the additional questionnaire for the PHQ-9 (in appearance and content).
The study did not aim to explore criterion or construct validity, as it was exploratory. A pilot test was conducted with a group equivalent to the study population (n = 20), and based on the results, necessary semantic and wording adjustments were made. Participation in the study was voluntary and anonymous, with data collected through self-administration of the questionnaire after obtaining informed consent. To maintain anonymity, participants were identified using their university account or institutional registration numbers without including their names. In addition, a consent question was included, specifying that if responses indicated severe depression or suicidal ideation, the participant’s training center would be informed to encourage them to seek medical attention. Acceptance of this follow-up was also voluntary.
Analysis Plan
The questionnaire information was stored in Microsoft Excel and then imported into the SPSS V-26 program. Univariate analysis was performed to describe the characteristics of the sociodemographic, institutional, residence, family, and personal history variables. Frequencies and percentages were reported for qualitative variables, and mean and standard deviation for quantitative variables. Nonparametric tests were applied to estimate differences for the bivariate analysis, and the chi-square of independence was used to determine the association between variables. In addition, multivariate analysis (discriminant) was performed to determine the factors associated with the development of depressive symptoms/depression and suicidal ideation.
The project adhered to the guidelines and ethical considerations of the current Declaration of Helsinki, the current Regulations on Health Research in Mexico, and the Universal Declaration of Human Rights of UNESCO. It was registered and approved by the Research Committees and Research Ethics Committee of the Faculty of Medicine, UNAM, with No. FMED/CEI/PMSS/102/2023.
Results
The study included 365 family medicine residents, 238 (65.2%) women and 127 (34.8%) men. The residents had an average age of 31.4 years (± 4.94 SD), with the youngest being 24 years old and the oldest 57. The majority, 260 (71.2%), reported having no children. Regarding marital status, 218 (59.7%) were single, 132 (36.2%) were married or in a common-law relationship, and 15 (4.1%) were divorced or separated. Regarding religious affiliation, 263 (72.1%) identified as Catholic, 51 (14%) as Atheist, and 36 (9.9%) as Christian. In terms of sexual orientation, 330 (90.4%) identified as heterosexual, 18 (4.9%) as homosexual, 13 (3.6%) as bisexual, pansexual, or asexual, and 4 (1.1%) preferred not to disclose their orientation. Further details are presented in Table 1.
Sociodemographic Data.
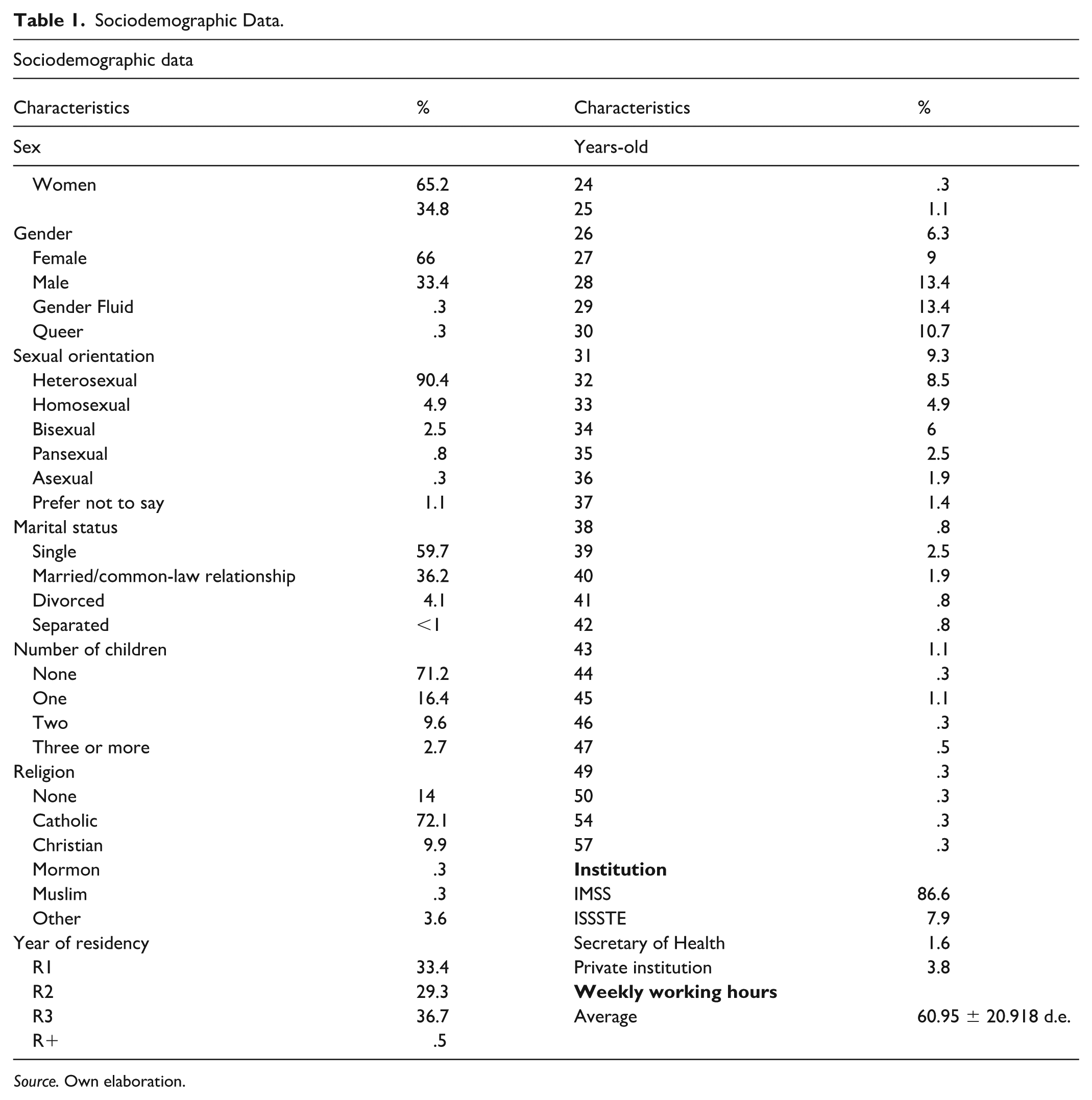
Source. Own elaboration.
The study included 122 first-year residents (R1) (33.4%), 107 second-year residents (R2) (29.3%), and 134 third-year residents (R3) (36.7%). The majority of participants conducted their residency at the Mexican Social Security Institute (IMSS) 316 (86.6%), followed by the Institute of Social Security and Services for State Workers (ISSSTE) 29 (7.9%), private institutions, and the Secretary of Health 6 (1.6%). The average number of working hours per week was 60.95 ± 20.92 SD.
Regarding medical errors committed by residents attributable to fatigue or lack of concentration, 223 (61.1%) reported having had them. Of the residents with medical errors, 178 (48.8%) had no repercussions for the patient, 27 (7.4%) had minor, and 2 (0.5%) had serious consequences. Nine (2.5%) residents preferred not to respond (see Table 2).
Types of Medical Errors During Residency.
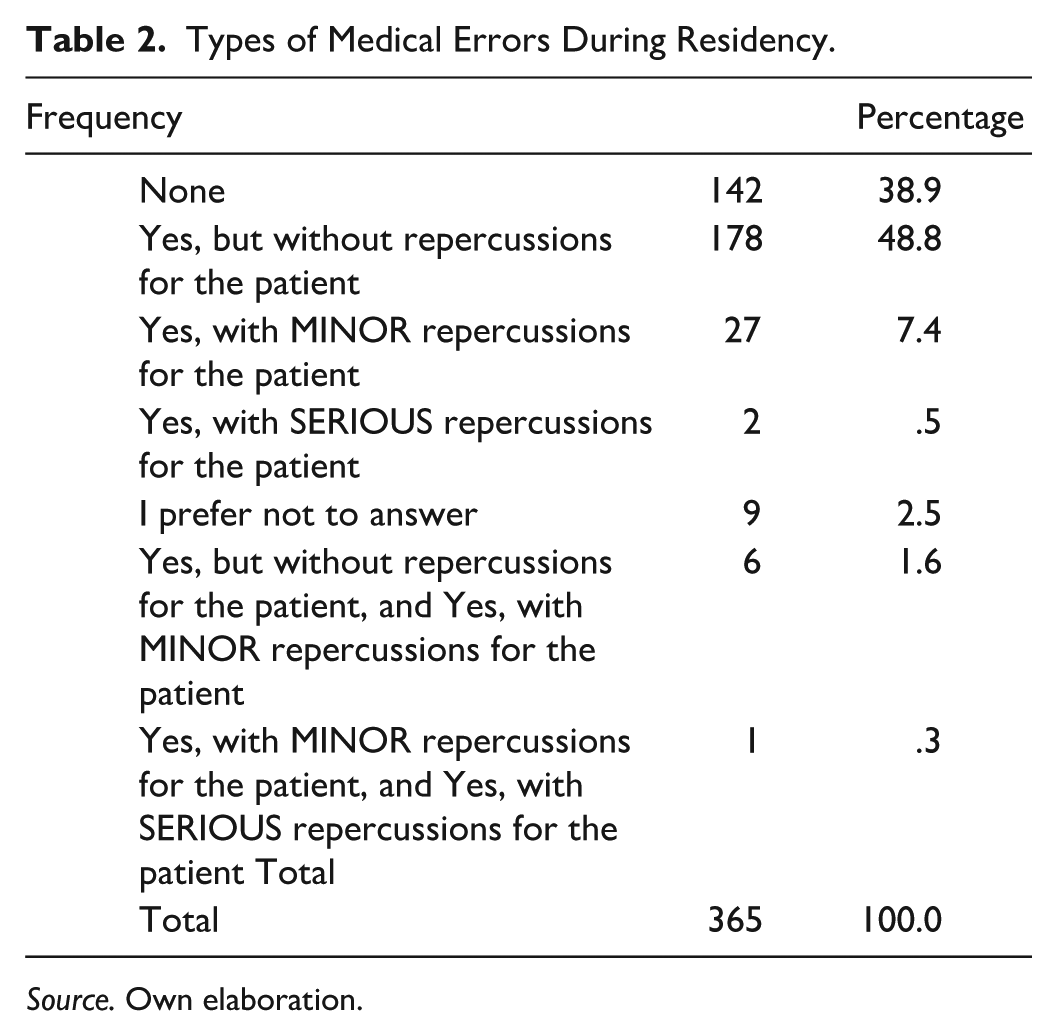
Source. Own elaboration.
During their residency, 199 (54.5%) of residents reported not experiencing harassment, bullying, discrimination, or violence, while 115 (31.5%) indicated they had experienced such incidents, and 51 (14%) chose not to respond. Of the residents who suffered some aggression 115 (31.5%), the most frequent were: workplace harassment 44 (12.1%); discrimination 41 (11.2%); violence from other physicians 38 (10.4%); violence from patients 36 (9.9%); violence from fellow residents 32 (8.8%); violence from their teachers 25 (6.8%), bullying 22 (6.0%), and sexual harassment 15 (4.1%) (see Figure 1).
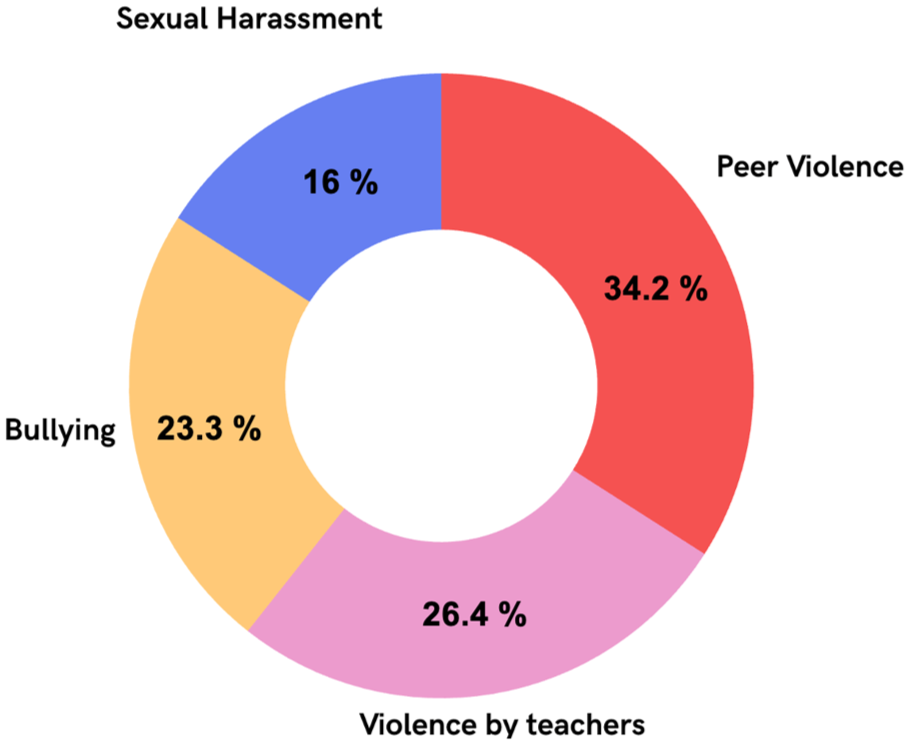
Harassment, Bullying, Discrimination, and Violence.
These data were obtained through multiple responses, so the sum of the percentages does not correspond to 31.5% because the residents reported having suffered more than one and up to seven of the events questioned.
In the family history of the residents, depression was found in 138 (37.8%); anxiety in 124 (34%); schizophrenia in 26 (7.15%); other psychiatric illnesses in 20 (5.5%); alcoholic father or mother in 34 (9.3%); drug use in father or mother in 4 (1.1%); suicides in the family 18 (4.9%), and sexual abuse 19 (5.2%)
The residents reported experiencing the following during their childhood and/or adolescence: bullying or cyberbullying 74 (20.3%), domestic violence 43 (11.8%), child abuse 5 (1.4%), rape 4 (1.1%), and 20 (5.5%) chose not to respond. Regarding their medical history, residents identified the following diagnosed conditions: depression 87 (23.8%), anxiety 115 (31.5%), previous suicide attempts 18 (4.9%), high blood pressure 20 (5.5%), hypothyroidism 15 (4.1%), heart disease 6 (1.6%), diabetes mellitus 6 (1.6%), cancer 3 (0.8%), kidney failure 1 (0.3%), and other degenerative diseases 19 (5.2%). In terms of substance use, the residents reported consuming alcohol 152 (41.6%), tobacco 39 (10.7%), marijuana 6 (1.6%), cocaine 1 (0.3%), morphine 8 (2.2%), antidepressants 73 (20%), anxiolytics 28 (7.7%), benzodiazepines 13 (3.6%), and other psychiatric medications 16 (4.4%).
Table 3 shows the results obtained by residents using the PHQ-9 questionnaire. The sample reported that 52 (14.3%) of resident physicians have moderately severe to severe depression. However, when including the subgroups of physicians who also have mild to mild-moderate depression, the prevalence increases to 218 (59.7%).
Depressive Symptoms Result According to PHQ-9.
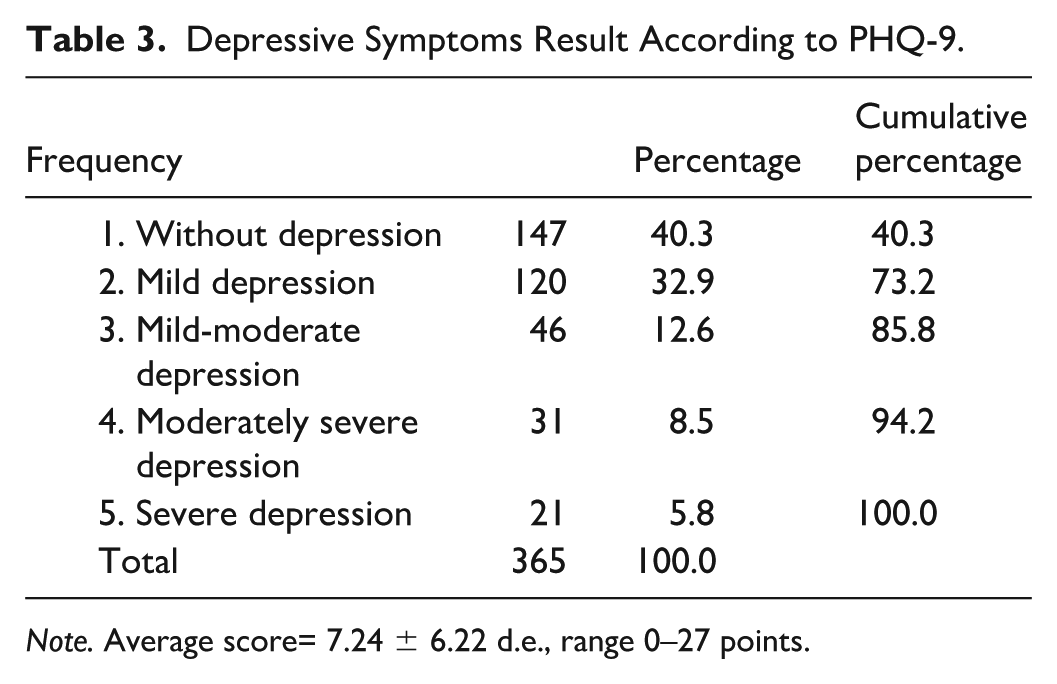
Note. Average score= 7.24 ± 6.22 d.e., range 0–27 points.
Finally, residents reported having thoughts of death in 61 cases (16.7%) and one or more suicide attempts in 7.9% (n = 29).
Multivariate Discriminant Analysis
Seventy-four independent variables were selected and grouped into six areas: (1) demographic and social profile, (2) school and work profile, (3) medical errors, (4) history of harassment, bullying, discrimination, and violence, (5) family history, and (6) personal history. The dependent variable was the result obtained by the residents in the PHQ-9 questionnaire score. Given that the questionnaire categorizes respondents into five classification subgroups based on their scores (Table 4), eight models were tested to determine which approach—either combining subgroups or evaluating them separately—offered the best discriminatory performance.
Eight Discriminant Models for Depression in Family Medicine Residents.
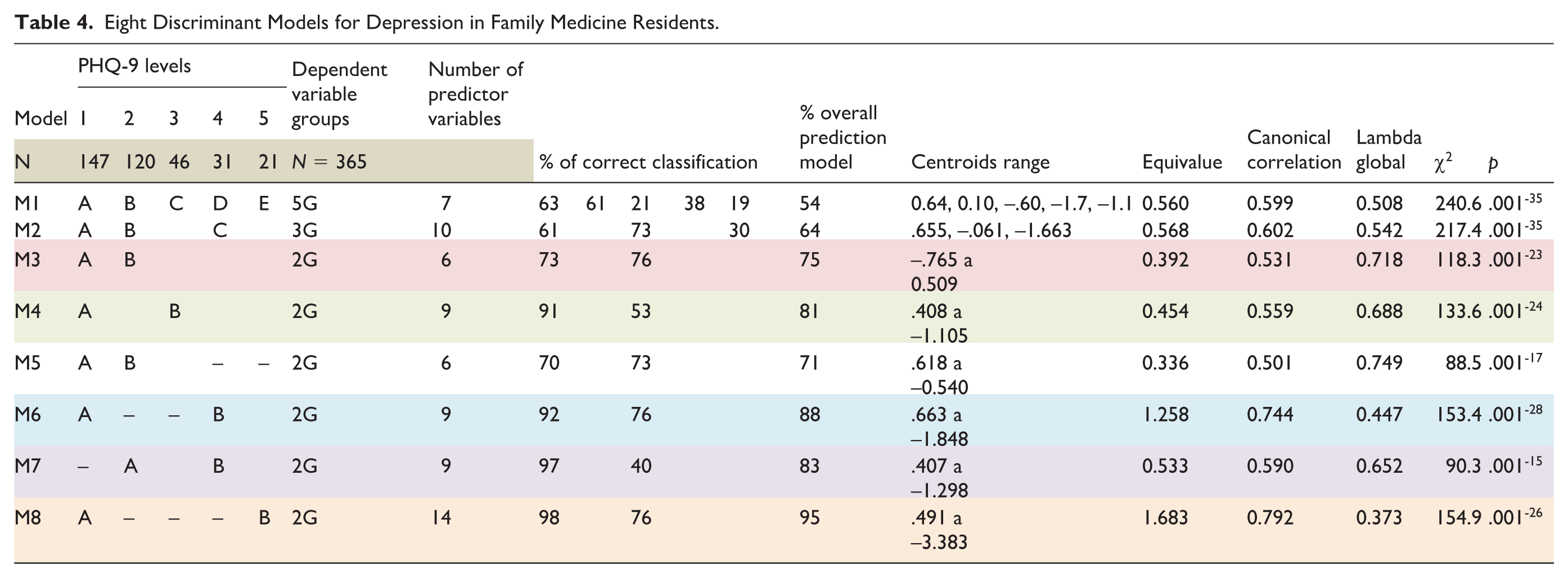
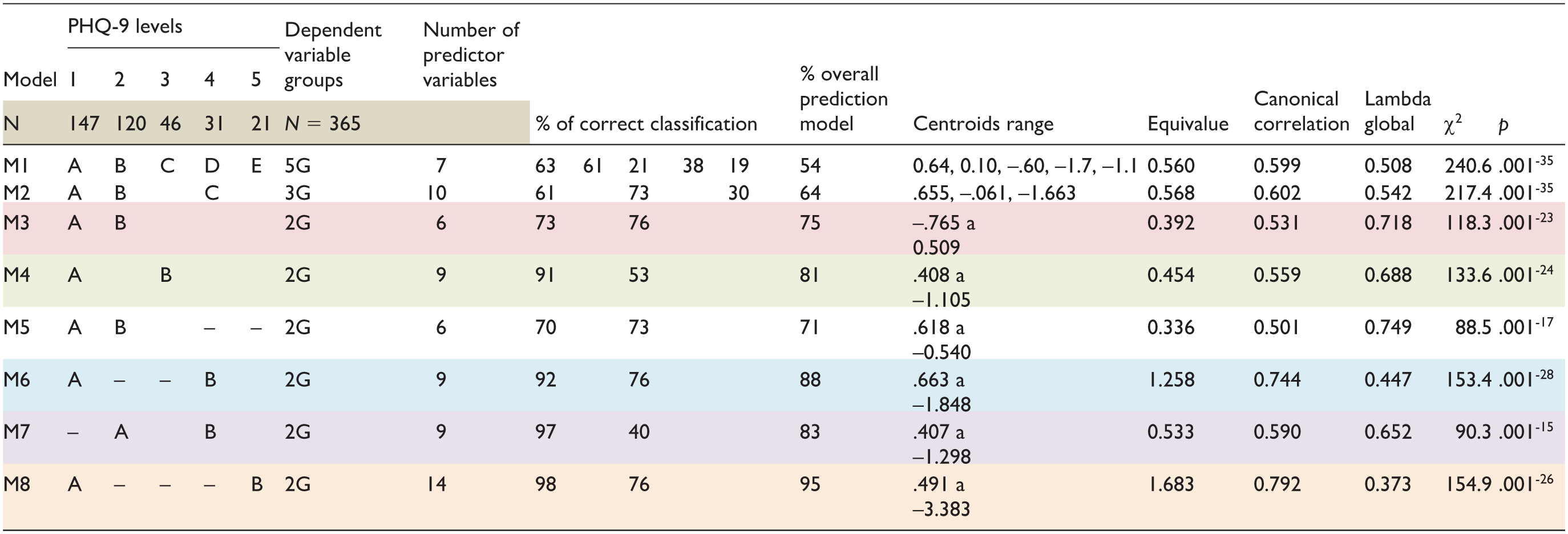
The technical and methodological specifications of the discriminant analysis for the eight calculated models were:
Variable inclusion method: stepwise (one at a time).
Analysis method: Wilks’ Lambda.
F criterion of the predictor variables: entry = 3.84 and eliminated = 2.71.
Prior probabilities: all different groups.
Centroids of the discriminant scores.
Determination of the discriminant function.
Probabilities of membership in the cases.
Classification agreement of the discriminant model.
Total discriminant scores.
The operational criteria to determine the best calculated discriminant predictive model were:
Greater number of predictor variables.
Higher percentage of correct classification.
Higher percentage of global prediction.
Greater separation in absolute units between the centroids.
Higher eigenvalue.
Higher multivariate canonical correlation.
Lower global lambda.
Model probability < 0.00001.
The final analysis was carried out using the following methods: The model was performed with information from 365 residents. Table 4 shows a summary of the operational criteria for each calculated model. It can be observed that model eight had the best predictive capacity, obtaining 14 variables that, in synergy, predicted the dependent variable, p = .001–26. Likewise, this model obtained the lowest overall lambda and the most significant absolute distance between the centroids. It should be mentioned that this model only analyzed the extreme groups of the PHQ-9 classification, that is, the group without depression versus the group with severe depression. Model six was considered the second-best calculated; it groups residents without depression versus those who had moderate-severe and severe depression.
In both models (8 and 6), only four predictor variables coincided: (a) personal history of depression, (b) I prefer not to answer, having suffered family violence, child abuse, or abuse, (c) having made medical errors with minor repercussions, and (d) use of benzodiazepines.
The predictor variables of Model 8 are shown in Table 5.
Predictor Variables of the Multivariate Discriminant Model 8.
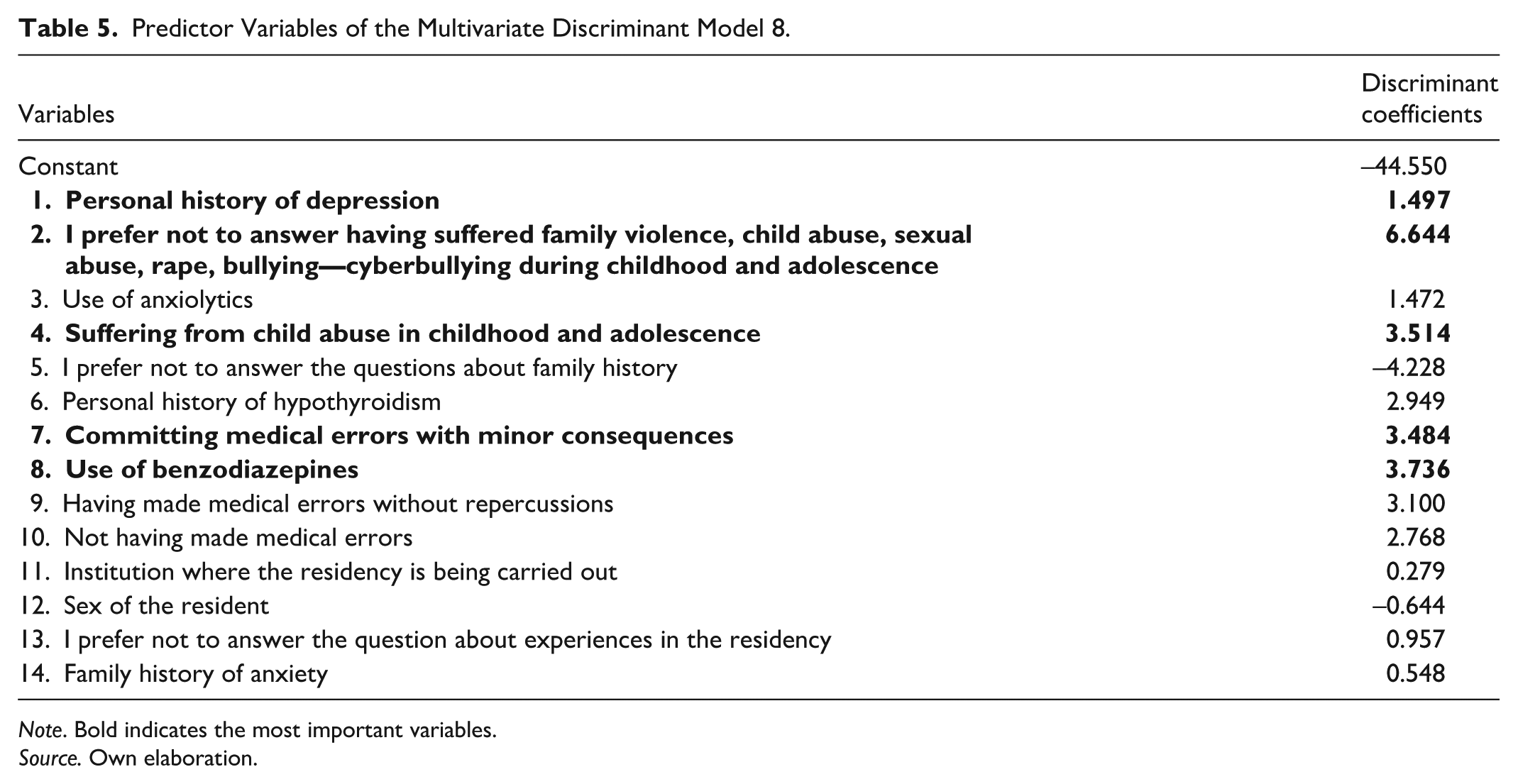
Note. Bold indicates the most important variables.
Source. Own elaboration.
In Table 5, the order presented means the importance of each variable in the model, according to the decrease in the overall Wilks’ lambda.
Using the coefficients provided in the table, the predictive equation for the multivariate canonical discriminant function is constructed following an additive linear model:
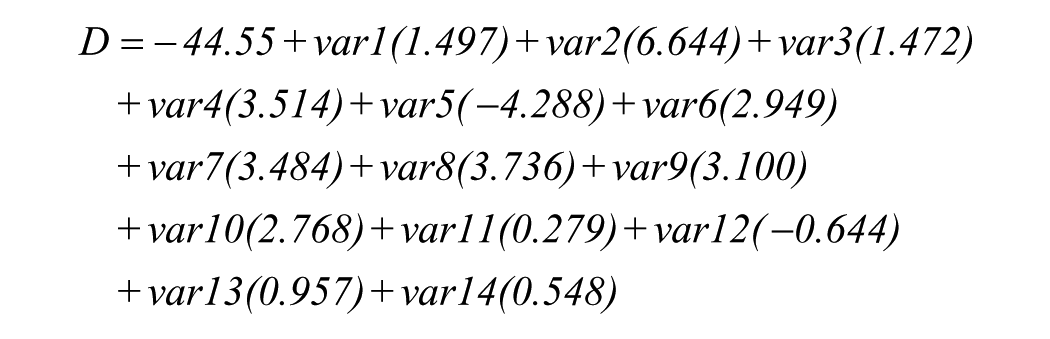
Finally, the discriminant scores for each resident, obtained from the model, did not show normality in their distribution; their average was −0.42614 ± 2.092 SD, with a minimum value of −8.455 and a maximum of 4.782.
Discussion
In 2023, the National Examination for Medical Residency Applicants (ENARM) in Mexico received 47,246 applications for residency positions. Of the 18,167 spots available, 2,580 (14.2%) were allocated to family medicine (Secretary of Health, 2023). The health institutions offering the most positions were the IMSS, SSA, and, in third place, the ISSSTE. Each year, applicants face intense pressure to achieve top scores, as competition for residency placement is highly stressful and demanding.
The medical profession has been characterized by its high competitiveness, from undergraduate education to residency and other postgraduate studies. While chronic stress is inherently associated with the medical field, other factors—such as genetic predispositions, environmental influences, and personality traits—also play a significant role in triggering or exacerbating mental health conditions like depression and anxiety (APA, 2023; Ishikawa, 2022; Jaulin et al., 2021; Levy et al., 2019; Pasqualucci et al., 2019). Notably, depression rates among undergraduate medical students and residents are strikingly similar, at 27.2% and 28.8%, respectively (Mata et al., 2015; Rotenstein et al., 2016; Schipper, 2016). Other studies have reported prevalence rates among residents ranging from 6% to over 60%, depending on specialty, location, and country (Al-Humadi et al., 2021; Alva-Diaz et al., 2021; Jiménez-López et al., 2015; Kwok, 2021; Levy et al., 2019; Talih et al., 2016). However, many studies fail to clarify the severity of depression, and variations in the sensitivity of screening instruments often result in inconsistent findings (Castaño-Castrillon et al., 2015; Mata et al., 2015), raising questions about the accuracy of reported prevalence and severity.
In this study, the prevalence of moderately severe to severe depression among residents was found to be 14.3%, closely aligning with the 15.4% rate reported for the general population by ENBIARE in 2021. However, when mild and mild-to-moderate depression were included, the prevalence rose alarmingly to 59.7%. Another critical finding of this study was that 16.7% of residents reported experiencing thoughts of death, and 7.9% had attempted suicide one or more times. These rates are lower than those reported at the University of British Columbia in Vancouver, where 33.3% of family medicine residents reported suicidal ideation, though the suicide attempt rate there was significantly lower at 2.9% (Laramée & Kuhl, 2019).
In a survey conducted among first- and second-year residents of various specialties at the Faculty of Medicine of the National Autonomous University of Mexico, personality profiles and their association with mental health issues and suicidal ideation were examined. The findings indicated that neurotic personality traits were most strongly associated with suicidal ideation, with a prevalence of 8%. Specialties with the highest risk included urology, psychiatry, forensic medicine, family medicine, critical care, and anesthesiology (Vargas-Terrez et al., 2015).
In the discriminant analysis, two of the eight discriminant models for depression identified four overlapping predictor variables: a history of depression, opting not to answer questions about violence during childhood and/or adolescence, having made medical errors, and the use of benzodiazepines. Notably, a history of depression—whether personal or familial—is strongly associated with an increased risk of developing or exacerbating depressive symptoms during residency (Al-Humadi et al., 2021; Angeles-Garay et al., 2020; Castaño-Castrillon et al., 2015; Cantón-Cortés & Rosario-Cortés, 2015). Furthermore, a family history of suicide or mental illness can heighten the likelihood of suicidal thoughts, as individuals may identify with the family member and imitate their behavior (Castaño-Castrillon et al., 2015). Despite these risks, three out of four residents do not receive antidepressant treatment (Levy et al., 2019), mirroring findings in a study of North American surgeons, where only 26% of those experiencing suicidal ideation sought specialized help within the previous year (Shanafelt et al., 2011).
Regarding experiences of violence during childhood and/or adolescence, 20% of residents reported being victims of bullying or cyberbullying, 12% experienced domestic violence, and 5.5% chose not to respond, suggesting that this group may have been exposed to severe forms of violence. Studies indicate that survivors of childhood sexual abuse are at a significantly higher risk of developing emotional disorders in adulthood, including depression, anxiety, low self-esteem, and difficulties in sexual relationships. The impact of such trauma depends on factors such as the nature of the abuse, the context in which it occurred, and the relationship with the aggressor (Cantón-Cortés & Rosario Cortés, 2015). In severe cases, such experiences may even lead to suicidal behavior. Moreover, a higher prevalence of childhood trauma has been documented in patients with borderline personality disorder (Cáceres-Taco & Vásquez-Gómez, 2013). Dysfunctional family environments often contribute to emotional instability during childhood, with long-lasting consequences that carry into adulthood (Garza-Rincones et al., 2018).
Depressive symptoms have also been linked to an increased likelihood of committing medical errors. In this study, 61% of physicians reported having made errors, with 48% reporting no repercussions for patients, 7.4% noting mild impacts, 0.5% identifying profound effects, and 2.5% declining to specify the implications, suggesting the possibility of severe outcomes. These adverse events have been associated with factors such as excessive working hours, physical exhaustion, lack of sleep, fatigue, stress (Kwok, 2021; Levine et al., 2022; Levy et al., 2019; McTaggart & Walker, 2022; West et al., 2009), insufficient clinical skills, cognitive overload, apathy, health problems, and inadequate academic supervision (Chávez-Ciriaco et al., 2024).
Data from the National Medical Arbitration Commission (CONAMED, 2023) indicate that the most frequent complaints resulting from medical errors include incorrect diagnoses, improper treatments and techniques, administration of inappropriate medications, unnecessary surgeries, and erroneous procedures. Notably, Fahrenkopf et al. (2008) found that depressed residents made 6.2 times more medication errors per month than their non-depressed counterparts, a pattern linked to issues with concentration and memory (Ramírez-Mendoza et al., 2023).
The use of benzodiazepines among medical residents does not seem to be related to any pharmacological treatment for depression. Among the first-line drugs to treat the disease are serotonin reuptake inhibitors, subsequently serotonin-norepinephrine reuptake inhibitors, and tricyclic antidepressants (Álvarez-Mon et al., 2017). It seems to correspond to one of the most frequent addictions in this group of people related to health, given the ease of obtaining them, even without a prescription from a psychiatrist.
A well-documented phenomenon during medical residency is the abuse of power, perpetuated by long-standing traditions passed down through generations. This dynamic stems from differences in knowledge and status between professors, heads of service, specialist doctors, and residents, creating an “inherited” power imbalance that fosters mistreatment (García & García, 2023). This culture often places lower-level residents under greater work and academic pressure, with studies showing a 15.8% prevalence of depressive symptoms during the first year of residency (range: 0.3%–26.3%) (Mata et al., 2015). In this study, 45% of residents reported experiencing some form of violence, with 14% choosing not to respond, likely due to mistrust and fear of retaliation from authorities. Among the remaining 31.5%, the most commonly reported issues included workplace harassment, discrimination, and violence perpetrated by other doctors, patients, and teachers. In addition, 4% of residents reported experiencing sexual harassment. These findings underscore the hostile and often traumatic environment that persists within medical residency programs.
The findings regarding the consumption of psychoactive substances reveal that the most commonly used substances among residents are legal ones, with alcohol ranking first, followed by tobacco. Among illegal substances, marijuana is reported at 1.6%, and cocaine at 0.3%. In addition, 3.6% of residents reported using benzodiazepines, and 2.2% reported morphine use. Although these frequencies are lower than those reported in other studies, such as from Ecuador and Colombia (Roldán-Soler et al., 2021), which highlight higher prevalence rates for marijuana, amphetamines, and other reality-distorting drugs, their use is often linked to social pressure from friends and peers, curiosity, and myths about enhanced concentration during study sessions. Furthermore, the use of psychoactive substances has also been associated with depressive and anxiety disorders (Observatorio de Drogas de Colombia [ODC], 2019).
It is interesting to mention that in the study of Family Medicine residents, 9.6% of the residents belong to the sexual diversity of lesbian, gay, bisexual, and transgender people (LGBT+), which represents almost double the percentage reported in the general population, according to the National Survey on Sexual and Gender Diversity (ENDISEG) 2021, with 5.1% of the population in Mexico.
Finally, it is essential to highlight that this study represents the initial pilot phase of the information collection instrument and the PHQ-9, which will be applied to 82 medical and surgical specialties at the Faculty of Medicine, UNAM. The results of this study cannot be generalized, as the specialty of Family Medicine, while clinical, is a horizontal discipline. Its training is characterized by rotations across various clinics, hospitals, and services throughout the 3 years of residency, which may contribute to professional identity conflicts—an issue less common in other specialties. Likewise, the temporality of the traumatic events suffered, especially in childhood or adolescence, could have led to their being forgotten or to some unintentional psychological block, which would affect the clarity of thought. The interpretation of the results in cases of “prefer not to answer” leaves the possibility open to different interpretations, which may not correspond to an accurate observation. In addition, the sample size was relatively small. However, a notable strength of this study is its multicenter design, with representation from multiple locations across four institutions in 18 states of the Mexican Republic, providing valuable insights despite its limitations.
Conclusions
The prevalence of depression among family medicine residents closely aligns with findings from other studies when considering only moderately severe and severe cases. However, when mild depression is included, the prevalence rises dramatically, affecting approximately three out of five residents across all years of the specialty. Even more concerning is that nearly 8% of residents with depressive symptoms reported having attempted suicide, one to three times higher than what has been documented in previous research.
His work also highlights the need to implement interventions to detect and address violence and mental health conditions beginning in elementary and high school, before the “harm” caused to individuals increases.
These findings underscore the urgent need for targeted interventions. Screening measures must be implemented to identify residents with depressive symptoms or risk factors that increase their vulnerability. Moreover, educational and health care institutions must establish robust therapeutic intervention protocols to address this pressing issue and support the mental health of their residents. Strengthening regulations and legislation to ensure the safety and quality of life and work of medical residents (working hours, avoiding violence of all kinds, etc.) could also help improve the quality of health services and reduce the risk of medical errors.
Footnotes
ORCID iDs
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.