
Abstract
Background:
Information on factors that increase mortality in remote settings is limited. This study aims to estimate the independent and joint role of several factors on mortality risk among older adults living in rural Ecuador.
Methods:
Participants were selected from community-dwelling older adults who were included in previous studies targeting mortality risk factors in the study population. Generalized structural equation modeling (GSEM) was utilized to evaluate prior causal assumptions, to redraw causal links, and to introduce latent variables that may help to explain how the independently significant variables are associated with mortality.
Results:
The study included 590 individuals (mean age: 67.9 ± 7.3 years; 57% women), followed for a median of 8.2 years. Mortality rate was 3.4 per 100 person-years. Prior work on separate multivariate Poisson and Cox models was used to build a tentative causal construct. A GSEM containing all variables showed that age, symptoms of depression, high social risk, high fasting glucose, a history of overt stroke, and neck circumference were directly associated with mortality. Two latent variables were introduced, 1 representing the impact of biological factors and another, the impact of social factors on mortality. The social variable significantly influenced the biological variable which carried most of the direct effect on mortality.
Conclusions:
Several factors contributed to mortality risk in the study population, the most significant being biological factors which are highly influenced by social factors. High social risk interact with biological variables and play an important role in mortality risk.
Keywords
Introduction
Several studies have found differences in mortality rates across populations living in urban centers and rural settings. These findings suggest that rural populations tend to have higher mortality rates than those in urban settings.1 -7 Using data from the National Vital Statistics System, a large US study revealed an important increase in the age-adjusted mortality rate in rural areas, which was only 7% higher than in urban centers in 1999, but 20% higher in 2019. 1 However, this and most other studies from High Income Countries failed to focus on the many risk factors that contributed to the greater mortality. As a result, the role of individual risk factors on all-cause mortality was often unrecognized.1 -4
Information on factors that affect the mortality risk in rural areas of Low-and-Middle Income Countries (LMIC) is even more limited, and studies are often confined to specific conditions or diseases.5 -7 It is likely that increased mortality among people living in rural areas may be related to factors at the community-level (underdevelopment, poor medical care) as well as at the individual-level (illiteracy, poor control of risk factors).
During the past few years, several studies have demonstrated the contribution of certain risk factors that are independently associated with increased mortality risk in rural Ecuadorian villages.8 -13 This study aims to estimate the independent role of each of these factors on mortality risk among older adults living in these settings.
Material and Methods
Study Population
This study was conducted in community-dwelling older adults living in Atahualpa, El Tambo, and Prosperidad. Inhabitants of these 3 neighboring rural villages located in coastal Ecuador share several characteristics that reduce the likelihood of confounding variables. The population is homogeneous regarding race/ethnicity (Amerindian ancestry), low levels of education, dietary habits, and comparable cardiovascular risk factors, as previously detailed. 14 The migration rate is low and adherence to the study is high, which provide an ideal setting for conducting longitudinal studies. 15
Study design
Following a longitudinal prospective design, participants were identified by means of yearly door-to-door surveys (2012-2019) and enrolled in the population-based 3 Villages Study cohort. All individuals signed an informed consent form at enrollment and were periodically followed to determine retention in the study. Those who emigrated or declined consent were removed from the cohort at the administrative censoring date of the last annual survey when the individual was interviewed. Participants who died were censored on the day of death, which was confirmed by death certificates. The last administrative censoring date was set as August 1, 2023. The study was approved by the I.R.B. of our Institution. Research was conducted following the ethical principles of the Declaration of Helsinki. Aggregated data will be available from the corresponding author upon reasonable request.
Main risk factors investigated
We selected as independent variables those factors that have shown to be associated with increased mortality risk in previous studies conducted in the same populations. These included neuroimaging markers of cerebral small vessel disease (cSVD), overt (non-lacunar) strokes, social risk, cognitive performance, dietary oily fish intake, severe tooth loss, neck circumference, symptoms of depression, and sleep quality. Table 1 summarizes the main exposures investigated and the cutoffs used for each of them in order to define high mortality risk. A comprehensive description of interviews and procedures used for identifying and categorizing each of these variables is detailed in Supplemental File 1.
Covariates and Exposures Investigated in This Study, Measurement Procedures, and Cutoffs Used to Define High Mortality Risk.

Clinical Covariates
Demographics and traditional cardiovascular risk factors were assessed at baseline and designated as potential confounders. Cardiovascular risk factors were assessed according to the Life’s Simple 7 construct of the American Heart Association. 16
Statistical Analysis
All analyses were carried out using STATA version 17 (College Station, TX, USA). To calculate the person-years of follow-up we considered the time from enrollment to the last administrative censoring date, study drop-out, or the day of death.
Evaluating the outcome (mortality) using a single regression approach (Cox Proportional hazards or Poisson regression models) was not comprehensive enough to identify all the potential causal links hypothesized for the present study. Therefore, generalized structural equation modeling (GSEM) was utilized to evaluate the proposed causal assumptions (biological or social), to redraw the causal links according to significant direct effects, and to introduce latent variables that may better explain how all the univariate significant variables were associated with mortality. GSEM used Poisson regression analysis with person-time as exposure to estimate the direct effects of confounding covariates and risk factors for mortality as the outcome. A hypothesis-driven first approach (causal model) guided a recursive modeling technique, instead of depending on model fit alone or attempting multiple combination of risk factors. These factors were discarded for the initial GSEM if they were not in the causal path and not significantly associated with the intermediate exposure or the outcome investigated.
The initial hypothesized model is a graphical representation of expected connecting links, with arrows pointing to the direction of causality. Odds ratios (OR) or Incidence Rate Ratios (IRR) were added to understand multivariate structure which corresponded to logistic or Poisson regression models for each variable that accumulates arrows toward it. Then, a measurement GSEM utilized Poisson or logistic regressions for binary variables in a sequence, choosing the variables assigned to each dependent variable through prior full regression models. Incidence rate ratios for the direct effect of the main mortality risk factors were obtained by exponentiation of the coefficients. Subsequently, a latent GSEM was fitted with a hypothesized structure based on the prior measurement model. Two latent variables were chosen, one representing the impact of mostly biological risk factors (biological latent variable), and another representing the impact of mostly social factors on mortality (social latent variable).
Additionally, to account for the fact that some mediators may be on the causal pathway for others, we allowed social risk, the cSVD score, and overt stroke to act as mediators individually or jointly. Similarly, we examined symptoms of depression and high fasting glucose to evaluate the size of their direct effect over mortality. The total effect was calculated as the sum of the direct (unmediated) and indirect effects (indirect effect of all mediators combined). The proportion mediated was calculated by diving the coefficient of the total indirect effect by the total effect. 17
Results
A total of 712 community-dwelling individuals aged ≥60 years living in 3 proximate villages were identified by means of door-to-door surveys. Of these, 590 (83%) received brain MRI and were included in the study. The population of this cohort study (n = 590) was prospectively followed for a median of 8.2 years (interquartile range: 4.2-11.2 years), and an average of 7.6 ± 3.4 years)
accumulating 4,480 years of follow up. Reasons for not obtaining MRI included refusal to participate (n = 53), severe disability (n = 14), claustrophobia (n = 12), and implanted pacemaker (n = 1). Twenty-five additional individuals had died and 17 had emigrated between recruitment and the invitation for MRI. All the above-mentioned variables were obtained for these 590 participants, with the exception of 23 subjects who did not complete cognitive assessment. Multivariate imputation of the missing scores was utilized according to prior research on the matter. 18
The mean age (at baseline) of the study population was 67.9 ± 7.3 years, 337 (57%) were women, and 469 (79%) had primary school education only. Cardiovascular risk factors in the poor range including: current smokers or quit <1 year: 21 (4%), body mass index ≥30 kg/m2: 150 (25%), poor physical activity: 72 (12%), unhealthy diet: 55 (9%), blood pressure ≥140/90 mmHg: 256 (43%), fasting glucose ≥126 mg/dL: 179 (30%), and total cholesterol blood levels ≥240 mg/dL: 69 (12%). Symptoms of depression were reported by 79 (13%) individuals, neck circumference was ≥40 cm in 88 (15%), severe tooth loss in 274 (46%), high social risk in 193 (33%), poor sleep quality in 252 (43%), low oily fish intake in 210 (36%), and cognitive impairment in 258 out of 567 screened individuals (46%), The total cSVD score was 3 to 4 points in 47 (8%) and 62 (11%) had an overt (non-lacunar) stroke. A total of 141 (24%) participants died during the study years, for a crude mortality rate of 3.4 per 100 person-years.
The first hypothesized causal construct included all variables that have been shown to be associated with mortality in the study populations, as well as other factors that were suspected of affecting mortality based on our previous experience with this cohort. Except for the initial separate logistic/Poisson regression modeling, full models were fitted with potential confounders, and risk factors were discarded for the next modeling step (GSEM) if they were not in the causal path and not significantly associated with the outcome investigated.
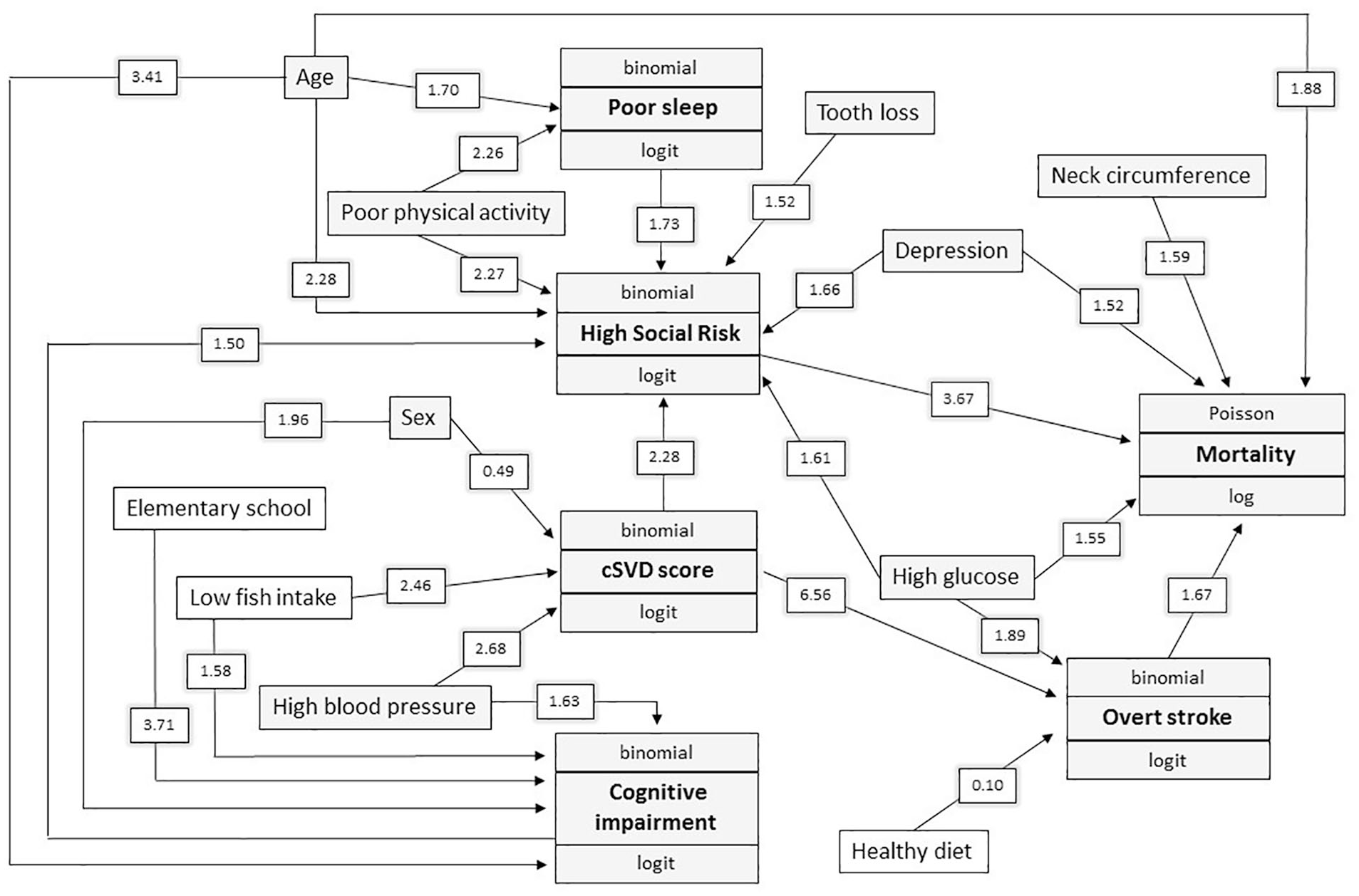
Figure 1 summarizes 2 levels of risk factors, 1 level corresponds to the hypothesized mediated factors such as poor physical activity, severe tooth loss and oily fish intake, and the next level corresponds to the mediators, where symptoms of depression, high social risk the cSVD score and overt stroke are depicted. Significant associations with mortality as well as between exposures (covariates and risk factors) are detailed in Table 2. The diverse significant associations between risk factors, exposures, and their influence on the outcome (mortality) are also shown in Figure 1.

Causal generalized structural equation modeling with arrows pointing to the hypothesized direction of causality. The Odds ratios or Incidence Rate Ratios were added in significant associations to understand multivariate structure and corresponded to separate Poisson or logistic regressions that were fitted for each variable that accumulates arrows toward it. Data below the boxes represented associations not initially hypothesized within this construct that resulted to be significant.
Separate Parsimonious Poisson and Logistic Regression Models Showing Significant Hypothesized Causal Associations Between Risk Factors and Main Exposures.

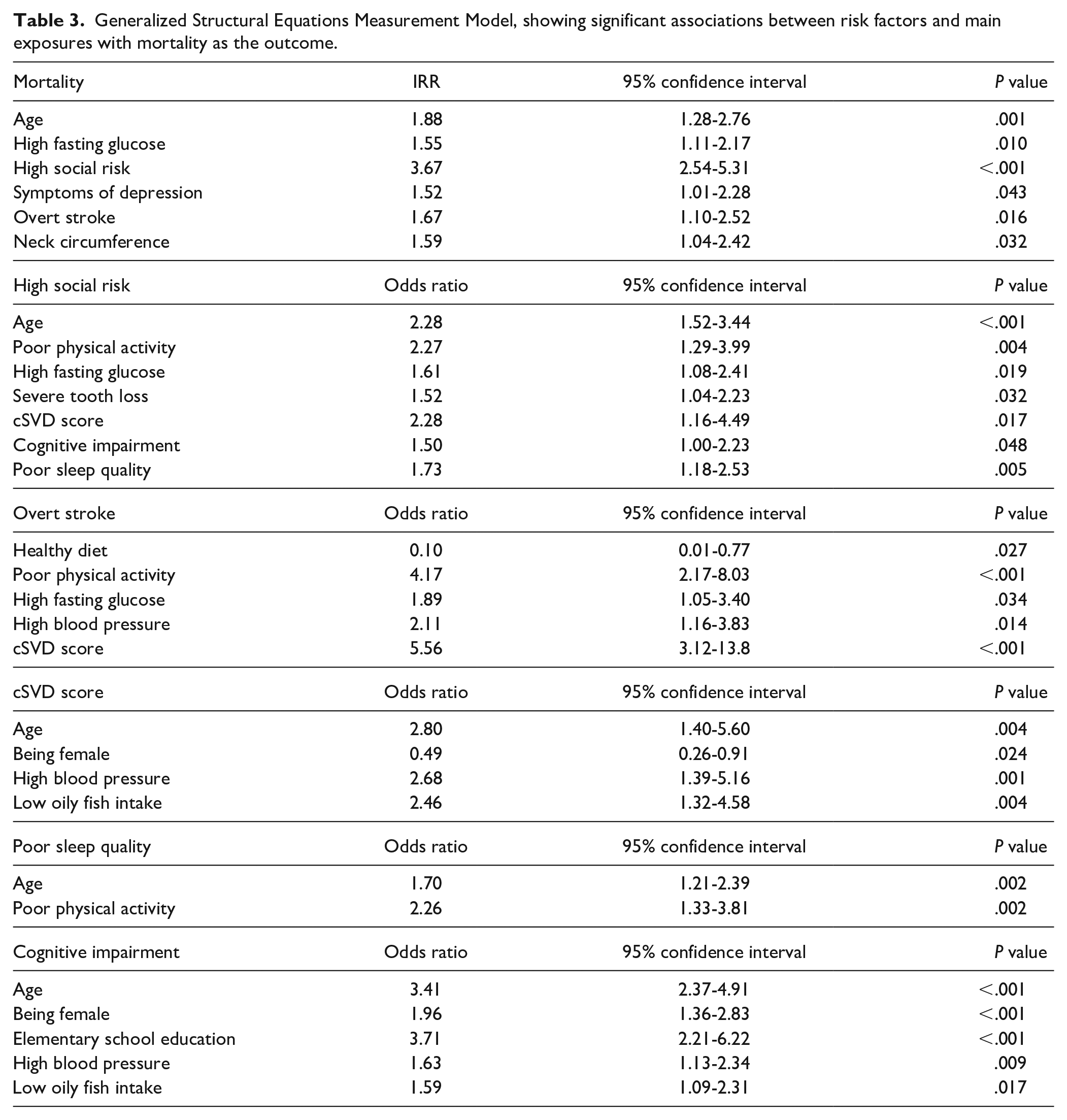
A GSEM without latent variables included 5 risk factors, which themselves had significant covariates associated with them, but only 2 (high social risk and overt stroke) directly affected mortality, while the other 3 (poor sleep quality, cognitive impairment and cSVD score) impacted mortality through social risk and overt stroke (Figure 2). Other variables significantly associated with mortality risk included age at baseline (IRR = 1.88; 95% CI: 1.28-2.76), symptoms of depression (IRR = 1.52; 95% CI: 1.01-2.28), and neck circumference (IRR = 1.59; 95% CI: 1.04-2.42). A detailed representation of the GSEM with coefficients and confidence intervals is detailed in Table 3.
Measurement generalized structural equation modeling showing the estimation of the associations between risk factors and confounders (the diagram shows only significant associations).
Generalized Structural Equations Measurement Model, showing significant associations between risk factors and main exposures with mortality as the outcome.
Using GSEM to estimate mediation effects, notable risk factors that were not directly associated with mortality—but in simpler multivariable models may be—were poor sleep quality, oily fish intake, the cSVD score, severe tooth loss, and cognitive impairment. Their total effect was mediated by overt stroke and particularly by high social risk (Figure 2). Other factors could be classified into 2 groups, those with mostly indirect effects, such as poor diet, poor physical activity, low levels of education, and high blood pressure, and those with a significant direct on mortality such as high fasting glucose and symptoms of depression.
A more nuanced examination of Figure 2 indicates 2 general paths,1 through social risk with mostly social factors feeding it (depression, tooth loss, and poor sleep) and another through overt stroke, with high blood pressure, high glucose levels, and cSVD score contributing.
In a GSEM with latent variables, we hypothesized a more complex structure based on the exogenous variable model, and 2 latent variables were chosen and tested, as previously mentioned (Figure 3). The biological variable represented the accumulation of mostly biological factors, which is more than just the total cSVD score or overt stroke. The social variable accumulated factors that have an important social component or are highly influenced by social risk and may be in the causal path to mortality. This model was fitted using a hypothesized causal structure, and covariates and risk factors were not included if they were not associated with the latent variable construct. The social latent variable significantly influenced the latent biological variable but did not independently influence mortality when the biological latent variable was in the model. In addition, age at baseline was independently associated with mortality risk irrespective of biological and social latent variables.
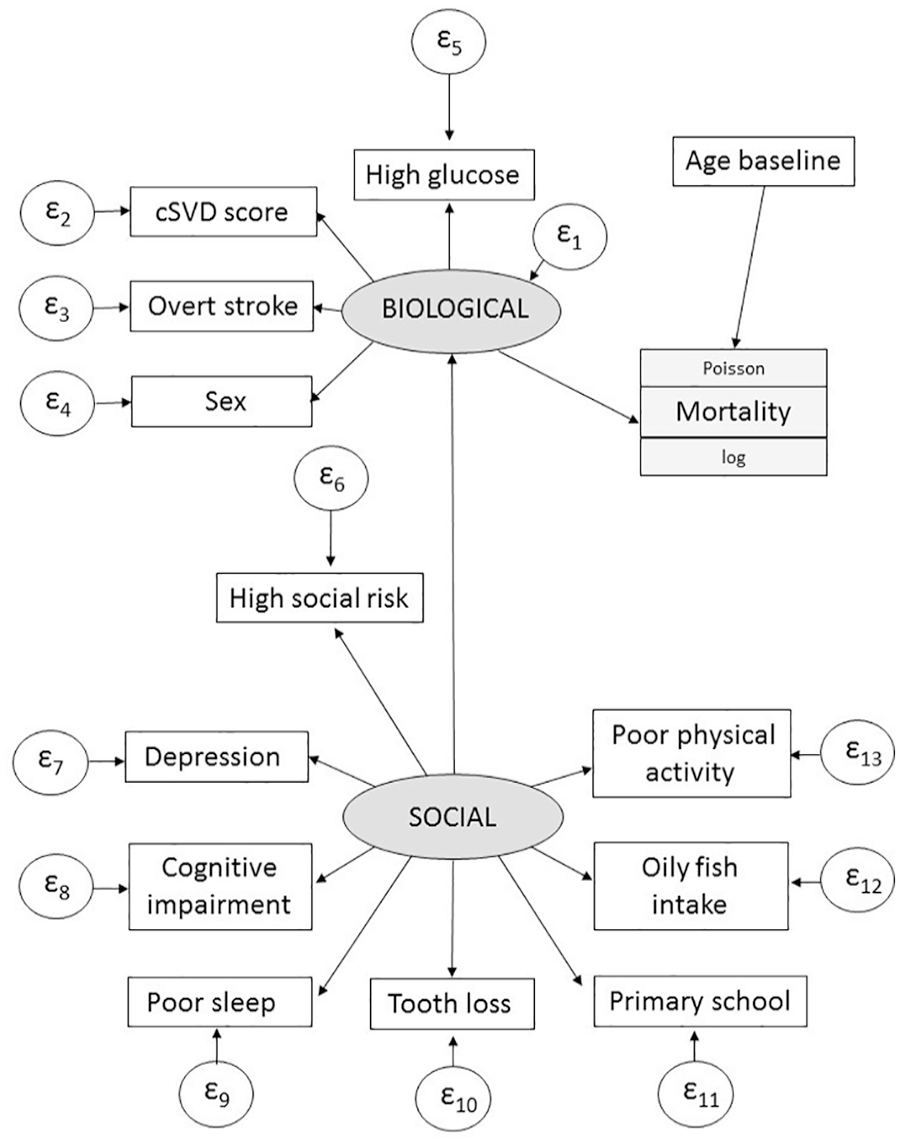
Specification of a generalized structural equation modeling for predicting mortality from known risk factors and 2 hypothesized latent variables (biological and social). Increasing age was associated with mortality independently of latent variables.
Discussion
This population-based study was based on results from distinct simultaneous longitudinal prospective studies conducted in the same population.8 -13 These combined results detailed the contribution of independent and joint risk factors on mortality risk among older adults living in rural settings of a LMIC.
The initial GSEM based on a preliminary causal path model, demonstrated several risk factors that were directly associated with increased mortality risk. At the same time, most of these variables (with the exception of neck circumference) were not independently associated with mortality; rather, their effects were likely the result of their association and interaction with other risk factors, as depicted in Figure 2. Additional variables did not have a direct effect on mortality but served to influence those factors that were associated with fatal outcomes. Most notably, symptoms of depression and cognitive impairment may increase mortality risk by contributing to high social risk, while cSVD score is associated with a history of overt stroke and high social risk which have a direct effect on mortality. In addition, low oily fish intake is associated with cSVD score which is associated with overt stroke that, in turn, has a direct effect on mortality. Symptoms of depression are associated with high social risk that increases the mortality risk and are also directly associated with mortality. Of interest, increased neck circumference and high fasting glucose were directly associated with mortality without influence from any other risk factors or conditions in this population.
Based on the above-mentioned considerations, a latent GSEM included 2 variables that could be inferred indirectly, one that incorporated all relevant biological factors (sex, high fasting glucose, cSVD score, and history of overt stroke), and another that took account of relevant social factors (symptoms of depression, cognitive impairment, poor sleep quality, severe tooth loss, level of education, dietary oily fish intake, and poor physical activity). It is plausible that some of these variables were in the path of high social risk, while others were just markers of frailty. The social latent variable influenced the biological latent variable but did not independently influence mortality when the latter was in the model. In this study, the effect of factors associated with mortality that are mediated by a high social risk included symptoms of depression and cognitive impairment, thus highlighting the independent relevance of these variables on mortality. As expected, age was independently associated with mortality risk irrespective of latent biological and social variables. Further models confirmed the importance of age as a mediator of mortality related to several exposures included in this study.
We are not aware of any prior studies that use a similar approach to assess the role of various risk factors and conditions on fatal outcomes in a population of community-dwelling older adults living in remote rural settings. However, important pieces of evidence may be gathered from the literature. A recent, large-scale study conducted in Canada used GSEM to ascertain the contribution of modifiable risk factors to socioeconomic inequities in cardiovascular disease mortality. 19 The authors found that these factors mediated two-thirds of the association between socioeconomic position and mortality, particularly in women. Other studies focused on factors influencing mortality among individuals with specific disabilities and cancer patients, and may not be comparable with results of the present study, but in general terms, are in line with our findings by showing that high social risk (social isolation and poor socioeconomic status) interact with biological variables and play an important role in mortality risk.20,21
The study has limitations. The main assumption of the GSEM is that the expected value of the outcome conditional on covariates is linear for both the exposures and covariates. Another issue is that we predicted how covariates are related to each other, and these assumptions may not always be correct. 22 The causal order of a significant association may not be verified for baseline covariates. In addition, there may exist other latent variables associated with mortality that were not hypothesized.
Major strengths of our study include the population-based design with unbiased enrollment of participants, as well as the models used for assessing potential causal directions in the complex relationship between the various covariates and exposures investigated and mortality. Our previous studies have modeled most of the risk factors, including some for mortality, and we have accumulated considerable evidence of the association between most of the confounders in our population. The measurement GSEM with its separate levels and multiple logistic and Poisson models, provides a unique perspective, enhancing the construct validity of the latent variables.
In summary, there is a vast array of risk factors and conditions that may contribute to mortality risk in a given population, underscoring the importance of gaining knowledge of the study population to better formulate cost-effective interventions aimed at targeting mortality at the population level. Results of the present study open new avenues of research aimed to increase knowledge on the complex associations, mediating effects, and interactions between risk factors and conditions that may influence mortality in selected populations living in remote settings.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241228123 – Supplemental material for The Impact of Biological and Social Factors on Mortality in Older Adults Living in Rural Communities
Supplemental material, sj-docx-1-jpc-10.1177_21501319241228123 for The Impact of Biological and Social Factors on Mortality in Older Adults Living in Rural Communities by Oscar H. Del Brutto, Robertino M. Mera, Denisse A. Rumbea and Mark J. Sedler in Journal of Primary Care & Community Health
Footnotes
Author Contributions
OHD: study design and manuscript drafting; RMM: statistical analysis and significant intellectual contribution to manuscript content; DAR: study coordinator, data collection, and analysis; MJS: significant intellectual contribution to manuscript content.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Universidad Espíritu Santo—Ecuador. The sponsor had no role in the design of the study, in the collection, analysis and interpretation of data, or in the decision to submit the manuscript for publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.