
Abstract
Introduction/Objectives:
There is growing consensus on the benefits of initiating palliative care early in the disease trajectory; however, palliative care needs for non-cancer patients remain to be elucidated. We investigated the trajectory of unresolved palliative care needs of non-cancer patients at home and explored associated factors.
Methods:
We conducted a multicenter prospective cohort study of elderly non-cancer patients at home in Japan between Jan 2020 and Dec 2020. Physicians assessed their palliative care needs using the Integrated Palliative Care Outcome Scale (IPOS). Unresolved palliative care needs were defined as IPOS symptoms above 2 (moderate).
Results:
In total, 785 patients were enrolled. The most frequent unresolved palliative care needs at enrollment were poor mobility (n = 438, 55.8%), followed by weakness/lack of energy (n = 181, 23.1%) and poor appetite (n = 160, 20.4%). Multivariate logistic regression analysis revealed that female and musculoskeletal disease were significantly positively associated with pain at starting home visits (OR = 1.89, P = .015; OR = 2.69, P = .005). In addition, neurological diseases were significantly positively associated with constipation and poor mobility 3 months after starting home visits (OR = 3.75, P = .047; OR = 3.04, P = .009).
Conclusions:
The order of the prevalence of unresolved palliative care needs may remain relatively stable over time, even for those receiving home-based palliative care services. We identified several specific diseases and conditions that were significantly associated with unresolved palliative care needs.
Introduction
The World Health Organization reported that 19 million people need palliative care worldwide, 66% of whom are non-cancer patients. 1 A recent study reported a projected rise in deaths from chronic diseases and an increase in overall deaths. 2 Thus, an increase in deaths at older ages would increase palliative care needs beyond expectations. Strengthening palliative care for non-cancer patients is essential for patients with chronic disease and those in older age groups. Older patients with progressive, long-term conditions may have different palliative care needs from cancer patients, who are more typically cared for by specialist palliative care services.3,4
A previous cross-sectional study reported that older hospitalized non-cancer patients experienced significantly more physical symptoms and functional dependence than cancer patients. 5 Jang et al 6 reported higher psychosocial and educational/referral domain palliative care needs than cancer patients. They also reported that physical and psychosocial domains of palliative care needs were significantly associated with health-related quality of life.
In general, older people with progressive, long-term conditions prefer to receive care and die at home.7 -9 Several recent studies have reported that dying at home is associated with a higher quality of life for patients than dying in a hospital.10 -13 Therefore, palliative care services, especially at the patient’s home, are needed to improve the quality of life of patients by relieving physical, psychosocial, and spiritual suffering. However, although many studies investigated the symptoms of suffering experienced by cancer patients undergoing palliative care, few studies have investigated non-cancer patients. Furthermore, despite the growing consensus on the benefits of initiating palliative care early in the disease trajectory, unresolved palliative care needs and the longitudinal nature of those needs for non-cancer patients remain to be elucidated. 14 The purpose of the study was to clarify the trajectory of unresolved palliative care needs of non-cancer patients at home and explore associated factors.
Methods
Study Design
We conducted a multicenter prospective cohort study to evaluate unresolved palliative care needs and explore the palliative care services offered to elderly non-cancer patients at home in Japan between Jan 2020 and Dec 2020.
Participants
Eligible patients were enrolled consecutively when starting home care at the participating facilities. The eligibility criteria were: (1) 65 years old or older, (2) non-cancer patients, and (3) started home care at the participating facilities during the study period. The exclusion criterion was refusal to participate by the patient or their family. The physician obtained oral consent from the patient, or from families if the physician determined that the patient lacked consent capacity.
Data Collection
We recruited participating facilities from the facilities that had participated in our previous studies.15 -22 We recruited 32 home care facilities in Japan between Jan 2020 and Dec 2020. Primary care physicians with expertise and experience in palliative care at home were primarily responsible for each patient evaluation and recorded all measurements on the day of enrollment. The physician followed the patient until 12 months after enrollment or discontinuation of home care such as due to death at home or admission to hospital or care home. The physicians routinely assessed and recorded the intensity of the patient’s needs and the services they utilized every 3 months. The Institutional Review Boards of University of Tsukuba approved this study and all participating facilities approved this study. This study was conducted under the ethical standards of the Declaration of Helsinki and the ethical guidelines for research presented by the Ministry of Health, Labour and Welfare of Japan. We obtained individual oral informed consent from all participants or their legal guardians.
Measures
Demographic Characteristics
We assessed patients’ demographic characteristics: age; sex; diseases and conditions requiring home visits; living with family or not; Palliative Performance Scale 23 ; Communication Capacity Scale (Item 4), which was used to evaluate the content of answers made by the patient during an interview 24 ; Palliative Care Phase of Illness 25 ; Age-adjusted Charlson Comorbidity Index 26 ; utilizing service (visiting nurse, visiting carer, visiting pharmacist, visiting rehabilitation, daycare, or short-term stay); and medical equipment in use (home oxygen, urinary catheter, enteral/parenteral nutrition, or continuous/biphasic positive airway pressure).
Palliative Care Needs
We assessed the intensity of the palliative care needs for pain, shortness of breath, weakness/lack of energy, nausea, vomiting, poor appetite, constipation, sore/dry mouth, drowsiness, and poor mobility. Physicians assessed not feeling at peace using the Integrated Palliative Care Outcome Scale (IPOS), 27 which was scored as 0 (not at all), 1 (slight), 2 (moderate), 3 (severe), and 4 (overwhelming). We defined unresolved palliative care needs as any IPOS symptoms specified as 2, 3, or 4, based on previous studies.21,28
Statistical Analysis
We employed descriptive statistics to present demographic information and IPOS scores. We used frequencies and percentages for categorical variables and means with standard deviations (SD) for continuous data. We excluded missing values from the analysis. We also performed a univariate analysis of unresolved palliative care needs and demographic characteristics and multivariate logistic regression analysis to explore the association between unresolved palliative care needs and demographic characteristics at and after enrollment. Based on discussions among the authors, we used the following variables: age, sex, diseases and conditions requiring home visits, living with family, using a visiting nurse, and using home oxygen as explanatory variables in each multivariate logistic regression. Multivariate logistic regression analysis was used to calculate odds ratios (ORs) and 95% confidence intervals after controlling simultaneously for potential confounders. Significance was defined as P < .05 and all analyses were conducted using SPSS-J software (ver. 28.0; IBM, Tokyo, Japan).
Results
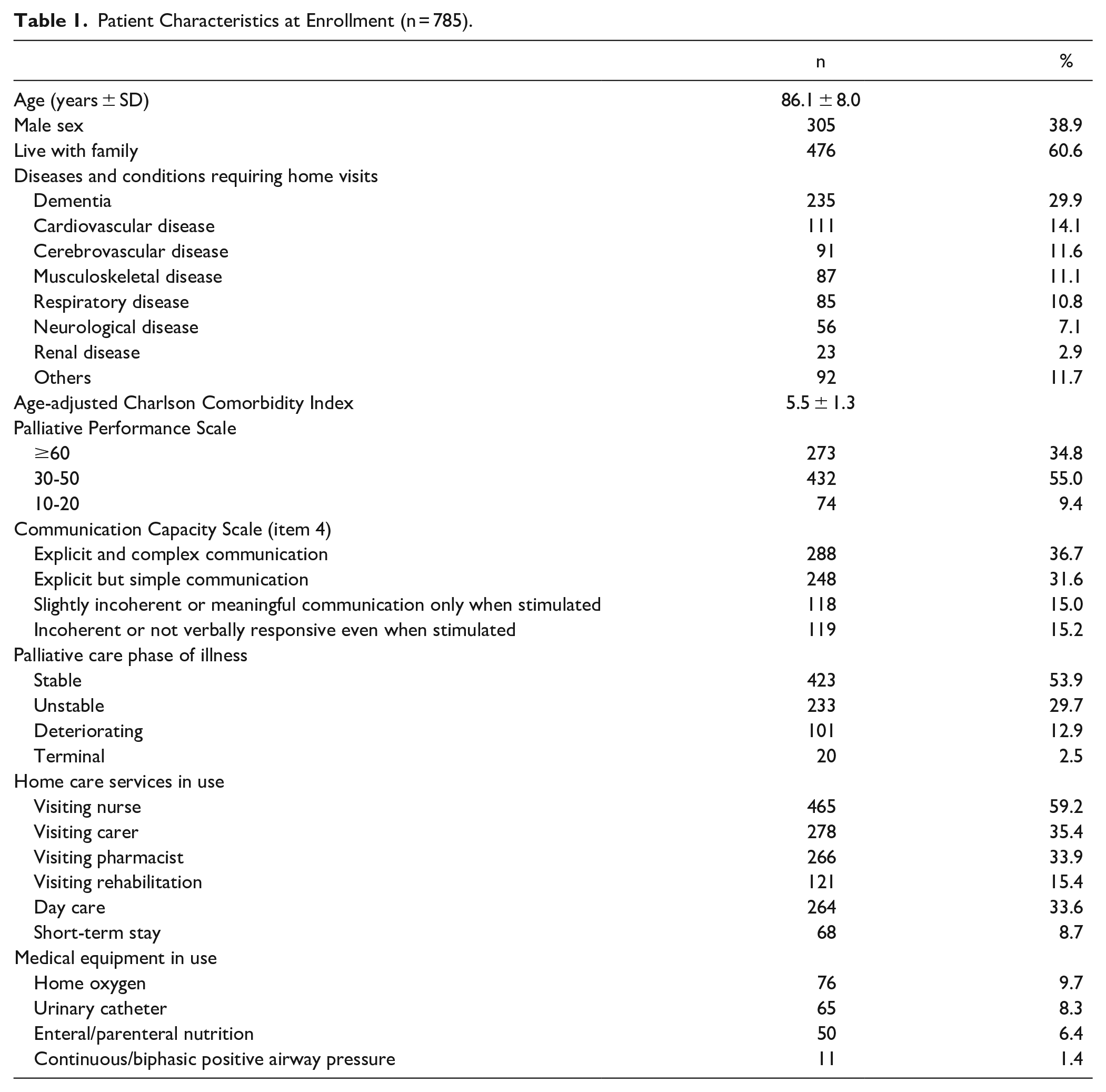
In total, 785 patients were enrolled. Figure 1 shows the patients’ flow diagram. Table 1 shows patients’ characteristics at enrollment. The mean age of the subjects was 86.1 ± 8.0 years, and 305 (38.9%) were men. Almost 60% of patients were living with family. The most frequent diseases and conditions requiring home visits were dementia (n = 235, 29.9%), followed by cardiovascular disease (n = 111, 14.1%) and cerebrovascular disease (n = 91, 11.6%). More than half of the patients were stable in the palliative care phase of illness (n = 423, 53.9%), 465 (59.2%) used visiting nurses, and 278 (35.4%) used a visiting carer at enrollment.

Participant flow.
Patient Characteristics at Enrollment (n = 785).
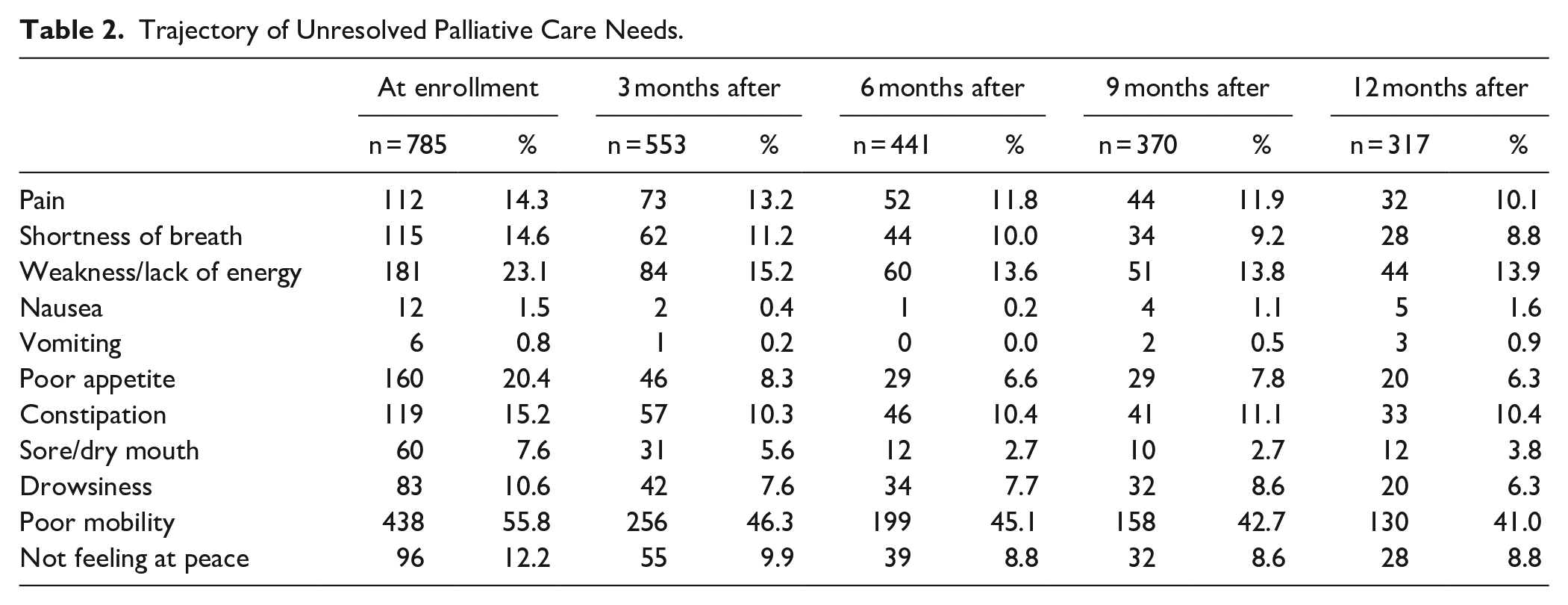
The trajectory of unresolved palliative care needs is shown in Table 2, and the trajectory of the Palliative Care Phase of Illness, home care service, and medical equipment are shown in Supplemental Appendix 1. The most frequent unresolved palliative care needs at enrollment were poor mobility (n = 438, 55.8%), followed by weakness/lack of energy (n = 181, 23.1%), and poor appetite (n = 160, 20.4%). The most frequent unresolved palliative care needs at 3, 6, and 9 months after enrollment were: poor mobility (n = 256, 46.3%; n = 199, 45.1%; n = 158, 42.7%), followed by weakness/lack of energy (n = 84, 15.2%; n = 60, 13.6%; n = 52, 11.8%) and pain (n = 73, 13.2%; n = 52, 11.8%; n = 44, 11.9%). Twelve months after enrollment, the most frequent unresolved palliative care needs were: poor mobility (n = 130, 41.0%), followed by weakness/ lack of energy (n = 44, 13.9%) and constipation (n = 33, 10.4%; Table 2).
Trajectory of Unresolved Palliative Care Needs.
Associated Factors of Unresolved Palliative Care Needs
Tables 3 and 4, and Supplemental Appendices 2, 3, and 4 show multivariate logistic regression analysis results at each assessment period. Multivariate logistic regression analysis revealed that female and musculoskeletal disease were significantly positively associated with pain at starting home visits (OR = 1.89, P = .015; OR = 2.69, P = .005), whereas dementia was significantly negatively associated (OR = 0.47, P = .038). Cardiovascular and respiratory disease were significantly positively associated with dyspnea at starting home visits (OR = 3.08, P = .016; OR = 5.71, P = .001), whereas dementia was significantly negatively associated (OR = 0.14, P = .016). Using visiting nurses at the starting home visits was significantly positively associated with poor appetite and mobility (OR = 2.20, P < .001; OR = 1.85, P < .001).
Associated Factors of Unresolved Palliative Care Needs at Starting Home Visits.

Multivariate logistic regression uses the following explanatory variables: age, sex, diseases, and conditions requiring home visits, living with family, using visiting nurse, and using home oxygen.
Associated Factors of Unresolved Palliative Care Needs 3 Months After Starting Home Visits.
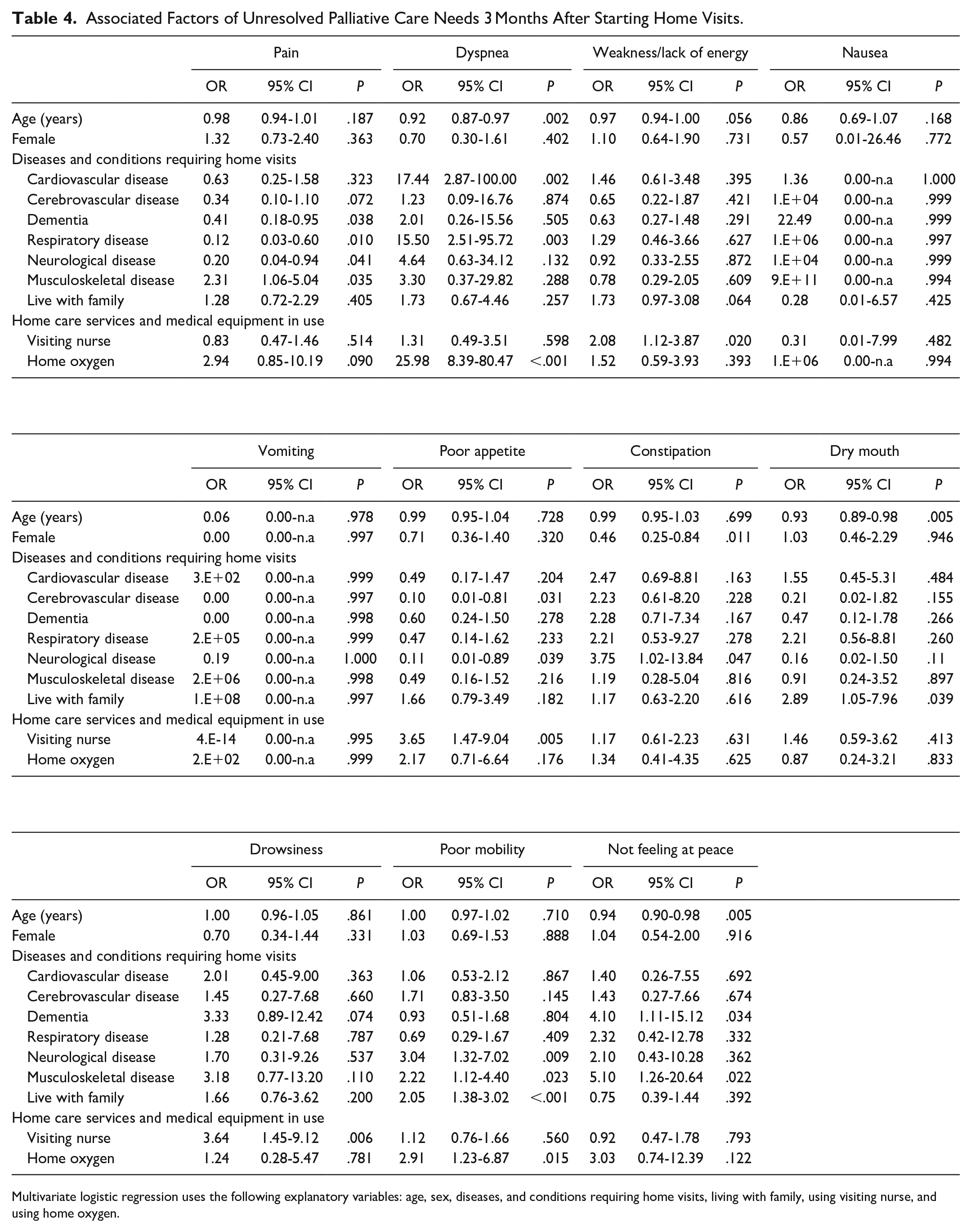
Multivariate logistic regression uses the following explanatory variables: age, sex, diseases, and conditions requiring home visits, living with family, using visiting nurse, and using home oxygen.
Neurological diseases were significantly positively associated with constipation and poor mobility 3 months after the starting home visits (OR = 3.75, P = .047; OR = 3.04, P = .009). In addition, musculoskeletal disease was significantly positively associated with pain, poor mobility, and not feeling at peace 3 months after the starting home visits (OR = 2.31, P = .035; OR = 2.22, P = .023; OR = 5.10, P = .022, respectively).
Regarding factors associated with unresolved palliative care needs over time, some symptoms, such as nausea, constipation, drowsiness, and not feeling at peace, varied. The number of associated factors decreased, but certain needs were specific such as pain, weakness/lack of energy, and poor appetite. Although the number of associated factors of dyspnea, dry mouth, and poor mobility decreased, each of these unresolved palliative care needs had some specific factors: dyspnea with cardiovascular and respiratory disease, dry mouth with older age, and poor mobility with neurological disease.
Discussion
To the best of our knowledge, this is the first survey to explore the trajectory of unresolved palliative care needs of non-cancer patients at home.
The first important finding of our study was that the most frequent unresolved palliative care needs at starting home care were poor mobility, followed by weakness/lack of energy. Moreover, based on prevalence/descriptive statistics, there were no significant changes in the order of unresolved palliative care needs over the following 12 months. Moreover, pain and dyspnea were not the primary unresolved palliative care needs at starting home care and over the following 12 months. These findings are inconsistent with a previous retrospective study of the last 6 months of life of non-cancer patients that found that pain had about 20% prevalence and dyspnea had from 20% to 70% prevalence. 29 One possible explanation for this difference was that the previous study did not assess symptoms other than pain and dyspnea. In addition, most of the patients in the previous study were cardiovascular, respiratory, and renal disease patients with a high prevalence of dyspnea.
Our findings partially differ from a previous systematic review, which reported that the most prevalent needs in cancer patients were fatigue, pain, and constipation 30 ; however, the rating scale was not standardized. Thus, the orders of the prevalence of unresolved palliative care needs may not change significantly over time, even for those receiving palliative care services at home.
The second important finding of our study was that the disease and conditions requiring home visits had a significant association with unresolved palliative care needs, such as pain, dyspnea, weakness/lack of energy, dry mouth, and poor mobility, at starting home care. Although over the following 12 months, the correlation between the disease and conditions requiring home visits and unresolved palliative care needs reduced, neurological and musculoskeletal diseases were significantly associated with several specific needs after starting home visits. One possible interpretation of this result is that home care services may conduct the appropriate pharmacotherapy and adjustment of the patient’s living environment. Recent studies have explored the symptom clusters of cancer patients in hospice/palliative care settings29 -31; thus, it would also be worthwhile to explore the symptom clusters of non-cancer patients along with home care.
Although utilizing a visiting nurse was significantly positively associated with several unresolved palliative care needs, such as poor appetite, poor mobility, and weakness/lack of energy, this result may imply these needs were refractory despite multidisciplinary treatment and care. Therefore, it is necessary to develop a multidisciplinary approach, such as physiotherapy and dysphagia rehabilitation, for home palliative care treatment.
This study is also noteworthy regarding what can be expected from home care for elderly non-cancer patients. Although causal relationships were not investigated in this observational study, the relief of symptoms, particularly poor appetite and sore/dry mouth, following a home visit may support the value of home care. Our findings suggest the potential of a multidisciplinary approach at home. Further studies using a complex intervention trial are necessary.
The present study had some limitations. First, we could not assess the details of patients and family background such as details of the medical history of disease, condition, and family support. Therefore, we could not adjust for confounding factors, such as the severity of the disease and condition and dose-response treatment effect. Thus, we could not conclude whether there was a causal relationship or clarify the mechanisms between unresolved palliative care needs and covariate items.
Second, we could not consider the interaction of successive needs; for example, poor mobility-induced constipation and medical treatments in a time-dependent manner. Thus, further research is needed to clarify the potential needs for cascade and medical treatments as time-dependent confounding factors.
Third, patients at home could not be assessed on a defined date due to factors such as the COVID-19 infection rate. Some of the evaluations at home were based on physicians’ estimates, which may have caused under- or overestimation of needs for home-based palliative care patients.
Fourth, since we recruited participating facilities from those that had participated in our previous studies, the generalizability of the results should be interpreted with caution.
Fifth, since we could not analyze patients who stopped using the home care service, the prevalence of unresolved palliative care needs trajectory and associated factors after starting home visitss had selection bias. Thus, caution is required to interpret the results of our study.
Sixth, since this study was conducted during COVID-19 pandemic, there was several barriers and bias in terms of availability of hospital care, drugs, and home care service. Thus, the caution is needed to interpret the result of this study.
Further high-quality observational studies that strengthen causal inference, such as those recommended in a previous study, 32 are needed to overcome these limitations and validate the generalizability of the study results.
Conclusions
The order of frequencies of unresolved palliative care needs did not change significantly when palliative care services at home were analyzed. Several specific diseases and conditions had a significant association with unresolved palliative care needs. Therefore, our findings suggest that multidisciplinary professionals must use standardized assessment tools and recognize and share the unresolved palliative care needs of non-cancer patients at home.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319231221431 – Supplemental material for Unresolved Palliative Care Needs of Elderly Non-Cancer Patients at Home: A Multicenter Prospective Study
Supplemental material, sj-docx-1-jpc-10.1177_21501319231221431 for Unresolved Palliative Care Needs of Elderly Non-Cancer Patients at Home: A Multicenter Prospective Study by Jun Hamano, Takuya Shinjo, Kazuhiko Fukumoto, Maiko Kodama, Hongja Kim, Sen Otomo, Shoichi Masumoto, Kotaro Hashimoto, Takamichi Matsuki, Kazuhiro Hisajima, Nobuyuki Miyata, Riri Suzuki, Shoji Yokoya, Keijiro Miyake, Ryo Takayanagi, Masakatsu Shimizu, Yoshihiro Kataoka, Hiroshi Taira, Sachiko Ozone, Hiroki Takahashi and Yoshiyuki Kizawa in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The participating investigators and study sites of this study were as follows: Keijiro Miyake, M.D., Ph.D. (Keijiro Clinic), Yoshihiro Kataoka, M.D., Ph.D. (Oomori Clinic/ Hitachi Oota Family Clinic), Masanori Kawahara, M.D., Ph.D. (Soshukai Okabe Clinic Sendai), Hongja Kim, M.D. (Kaita Hospital), Takashi Inaba, M.D. (Kasama City Hospital), Hiroki Takahashi, M.D. (Kamisu Saiseikai Hospital), Kaoru Okawa, M.D. (Kameda Medical Center), Ryo Osawa, M.D. (Kitaibaraki Family Clinic), Fuminao Kitanishi, M.D. (Total Family Care Kitanishi Clinic), Keiichirou Sakato, M.D. (Kensei Kuroishi Clinic), Takuya Shinjo, M.D. (Shinjo Clinic), Yohei Shinya, M.D. (Chubu Tokushukai Hospital), Yu Yamamoto, M.D. (Tsukuba Central Hospital), Hiroshi Taira, M.D. (Torimachi Clinic), Kazuhiro Hisajima, M.D. (Dr. GON Kamakura Clinic), Tomoyuki Koga, M.D. (Nozominohana Clinic), Asumi Nakamura, M.D. (Himawari Clinic), Kotaro Hashimoto, M.D. (Fukushima Home Palliative Care Clinic), Ryo Takayanagi, M.D. (Maebashi Kyoritsu Clinic), Mariko Shutoh, M.D., Ph.D. (Minato Home Care Clinic), Shouko Nishimizu, M.D. (Miyazaki Clinic), Yuri Morimoto, M.D. (Morimoto Clinic), Jun Sasaki M.D. (Yushoukal Medical Corporation), Junichiro Toya, M.D. (Sakura-shinmachi Urban Clinic), Hiroto Shirayama, M.D. (Osaka Kita Home Care Clinic), Yasuhiro Saitou, M.D. (GP Clinic Jiyugaoka), Nobuyuki Miyata, M.D. (Miyata Clinic), Yurika Kawamura, M.D., Ph.D. (Miyata Clinic), Masakatsu Shimizu, M.D., Ph.D. (Shimizu Medical Clinic), Ryo Yamamoto, M.D. (Saku Central Hospital Advanced Care Center), Yousuke Kimura, M.D. (Yamato Clinic), Yasuyuki Arai, M.D., Ph.D. (Iki-iki Clinic), Hideki Shishido, M.D. (Shishido Internal Medicine Clinic), Kazushi Nakano, M.D., Ph.D. (Nakano Zaitakuiryou Clinic), Maiko Haruki, M.D. (Orange Home-Care Clinic), and Sen Otomo, M.D. (Seimeikan Clinic).
Author Contributions
All authors made substantial contributions to the conception and design of the work. JH and TS facilitated the acquisition of data, YK, SY, and SM led the interpretation and drafting of the manuscript, all authors revised it critically, and all authors read and approved the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI Grant Number 19K10551, and a research grant of the Mitsubishi Foundation (201930027). The funder had no role in the design and conduct of the study; the collection, management, analysis, and interpretation of data; the preparation, review, and approval of the manuscript; or the decision to submit the manuscript for publication.
Ethical Approval and Consent to Participate
This study was conducted under the ethical standards of the Declaration of Helsinki and the Ethical Guidelines for Epidemiological Research issued by the Ministry of Health, Labour and Welfare of Japan. The Institutional Review Boards of the University of Tsukuba approved this study (No. 1651).
Consent for Publication
Not applicable.
Availability of Data and Materials
The datasets generated and analyzed during the present study are not publicly available due to them containing information that could compromise research participant privacy/consent but are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.