
Abstract
An increasing number of older persons have complex health care needs. This, along with the organizational principle of remaining at home, emphasizes the need to develop collaborations among organizations caring for older persons. A health care model developed in Sweden, the Mobile Integrated Care Model aims to promote work in teams across organizations. The aim of the study was to describe nurses’ experiences in working and providing health care in the Mobile Integrated Care Model in the home with home health care physicians. Semi-structured interviews were conducted with 18 nurses and analyzed through qualitative content analysis. The method was compliant with the COREQ checklist. A mutually trusting collaboration with physicians, which formed person-centered care, created work satisfaction for the nurses. Working within the Mobile Integrated Care Model was negatively impacted by being employed by different organizations, lack of time to provide health care, and physicians’ person-centered work abilities.
Introduction
A rapidly increasing older population with complex health care needs has moved health care from the hospital environment to the home of the older adult. In the home, the home health care nurse is the patient's core contact. Patients receiving home health care are often older adults who have several medical diagnoses and functional impairments and are frail. Hence, these patients require complex health care from several health care organizations.1,2 Potentially, there is a risk that a patient's personal needs will not be met when several organizations are involved. Similarly, patients may not be given the opportunity to participate in planning their own health care. 3 Municipalities and regions need to undergo structural changes to provide coherent and coordinated health and social care. 4 To meet this need, health caregiving organizations within one county of Sweden have worked together to create a care model for health care given across organizational borders: the Mobile Integrated Care Model (MICM). The aim of this care model is to provide coherent health care for older adults receiving care within the home. The health care is provided by an integrated team consisting of health care professionals employed by the municipality and a home health care physician (MICM physician) who conducts home visits. The health care team also co-creates a medical health care plan (MHCP) with the patient and their next of kin.
Knowledge about nurses’ experiences of working in integrated health care teams with home health care physicians is limited. That, in combination with the novelty of the model, emphasizes the importance of exploring nurses’ experiences in working within MICM.
Swedish home health care
In Sweden, the municipality is responsible for health care and social service for older persons, excluding physician health care, for which the county council carries the responsibility. 5 Collaboration between health and social care is a necessity for providing good quality care, not least for older persons with complex care needs. Accordingly, the Board of Health and Welfare has expressed a need for change in collaboration between health care organizations. 6 Specifically, the board emphasized the need for improvements in the provision of coherent health and social care to increase continuity, accessibility, and patient participation. As a response to this inquiry, the county of Skaraborg created the Mobile Integrated Care Model (MICM).
The Mobile Integrated Care Model
The MICM consists of three forms of health care: mobile hospital health care team, mobile home health care physician, and mobile hospital palliative team (Figure 1). 7 In the MICM, professionals from health care authorities work across borders to provide person-centered, coherent, coordinated, and cost-effective health care with good quality provided by integrated teams.7,8

The Mobile Integrated Care Model.
Previous research has shown that one of the benefits of interdisciplinary teams is how different professionals acquire an increased understanding of what the other professionals within the team do and why. 9 Successful teamwork develops over time through teambuilding and meetings, 10 as well as shared understanding of the concepts of care. 11 By doing this, relationships and trust are built within the team. 10 Having few and easily accessible care contacts have been identified as central to creating a sense of security and quality of care. 12 In the Swedish context, challenges include collaboration with MICM physicians, as they are employed by an organization different from that of the other health care professionals within the MICM team. 9
The aim with the MICM is focused on creating value in life for the patients and their next of kin while diminishing the number of health care contacts and increasing continuity for the patient. 7 The MICM also aims to be person-centered, where the patient participates in creating the MHCP when meeting the MICM physician and nurse in the home. 7 The basis of person-centered care is to initiate a partnership with the patient and, through their narrative, to identify the patient's history, current situation, resources, and needs, as well as to find common goals. The health care needs to be documented, monitored, adapted, and merged with the patient's goals and context.13,14 Person-centered care has a beneficial impact on work satisfaction, productivity, and organizational commitment from staff. 15 To our knowledge, there is limited knowledge about nurses’ perspectives on working within an interdisciplinary team and naturally within the MICM, as it is a new model. Taken together, these factors provide motivation to explore the subject.
Aim
This study aimed to describe nurses’ experiences of working and providing health care in the Mobile Integrated Care Model in the home with home health care physicians.
Method
Design
The inductive, qualitative study design included semi-structured interviews, conducted using an interview guide. The design provided the opportunity to access the nurses’ experiences. 16 The data collected were then analyzed through content analysis according to the method described by Graneheim and Lundman. 17 The study method was compliant with the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist. 18
Setting
The MICM with an MICM physician is an interdisciplinary team that includes an MICM physician employed by a primary health care center. The other members of these teams are nurses, occupational therapists, physiotherapists, and assistant nurses performing health care, employed by the municipality. The MICM physician and nurse make home visits to the patient's home when needed, and create medical health care plans (MHCPs) together with the patient and their next of kin once a year.
Participants
Executive directors in 15 municipalities in Skaraborg were asked to give their consent to allow nurses in their organizations to participate in an interview. Out of those 15, 12 met the inclusion criteria of having implemented the MICM at least six months before the start of the study. The participating municipalities were geographically distributed across the region and varied in size. Nurses who had worked for longer than six months within the municipality were invited to participate. The nurses were recruited by their manager, who asked if they wanted to participate. If the nurses accepted, the manager sent contact information to the project manager. The researchers were not informed if any nurses declined. The nurses received a written information letter that described the study's aim, method, and the researchers’ credentials. Eighteen nurses within the age span of 25–60 years, with experience ranging from 7 months to 39 years within municipality care, were interviewed. One to three nurses from each municipality participated, based on how many MICM physicians there were, as well as the size of the municipality. Out of the participating nurses, 17 were female and one was male. All nurses were registered nurses, while some were also clinical specialists in primary health care and/or geriatric fields.
Data collection
Data were collected through individual semi-structured interviews, which lasted 36–106 minutes, and were voice-recorded and transcribed verbatim. Field notes were made by the researchers after each interview but were not included in the analysis. The interview guide was constructed with open-ended questions to provide an opportunity for the nurses to describe their own experiences. The questions focused on their general experience with the MICM within municipal health care. Follow-up questions were asked to deepen the dialogue and enable reflection. Two pilot interviews were conducted to test the interview guide. The interview guide was deemed satisfactory in addressing the aim of the study and was therefore included in the results. The interviews took place at a location chosen by the nurse. The workplace was preferred by all the participants. Seventeen of the interviews were conducted in person, and one was conducted digitally via a video call. Ten interviews were conducted during the winter of 2018–2019 by the second and last authors, as well as by two students in a postgraduate specialist nursing program in primary health care nursing. Eight interviews were conducted during the autumn of 2020 by the first author. This was to reach saturation in the material. The interviewers had all worked as nurses prior to the study but not within the MICM. There was no relationship between the researchers and the participants at the time of the study.
Analysis
The transcribed data were analyzed through qualitative content analysis, according to the method described by Graneheim and Lundman. 17 The method is used for making replicable and valid inferences from data to their context, with the purpose of providing knowledge and new insights. The goal is to attain a condensed and broad description of the phenomenon in which the outcome of the analysis results in concepts, categories or themes. 19 The textually close analysis in this method was suitable to address the aim of describing the nurses’ experiences, while keeping the result as true to the data as possible, in the manifest (obvious) and latent (underlying) meaning. 18 The transcribed text of the interviews was read several times to gain a sense of the overall content. Meaning units that addressed the study's aim were drawn from the interview text, abstracted, condensed, and subsequently labeled with codes. Further, the codes were sorted into content areas that later became sub-categories and categories on a manifest level. An interpretative theme on a latent level, representing the underlying content in the categories (Table 1), was identified by all coauthors. The transparency of the analysis as well as quotation usage enhanced the trustworthiness of the analysis. The quotations also illustrate the findings and validate the results. The first author analyzed the data, although the analysis consisted of a back-and-forth process in which there was transparency through the analysis among all coauthors, which increased the credibility and the trustworthiness of the results. No software was used to analyze the material.
An example of the analysis process.
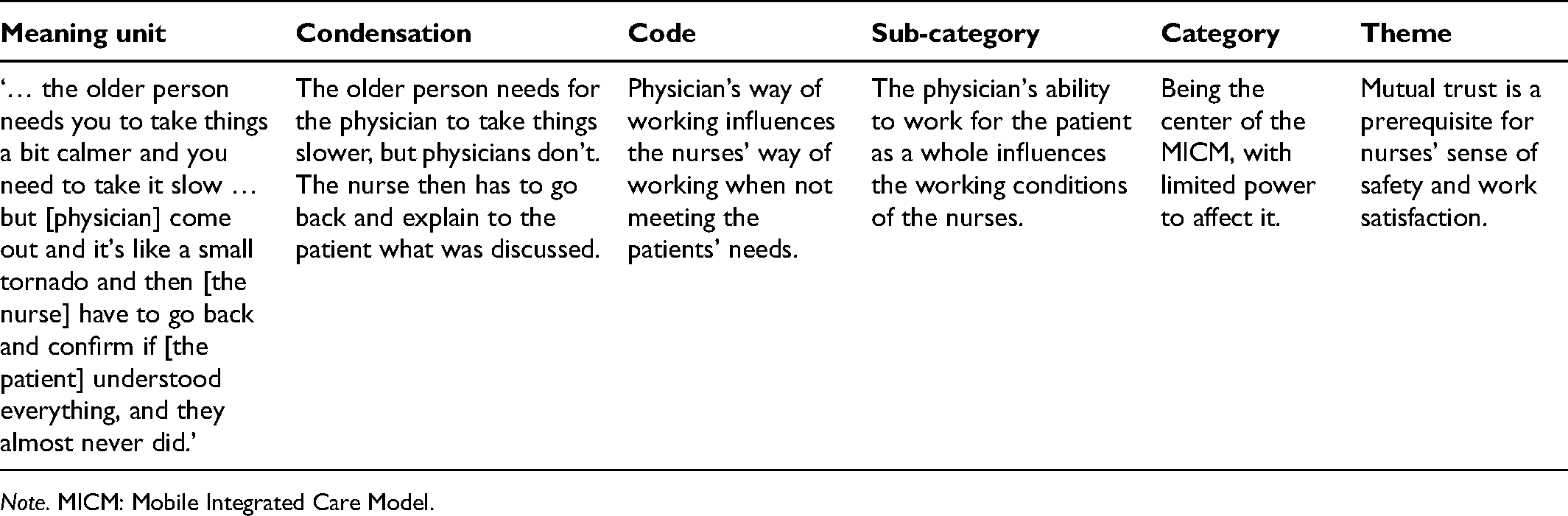
Note. MICM: Mobile Integrated Care Model.
Ethics
The project was approved by the Ethical Review Authority (Dnr 1020-17; 2019-02563; 2020-04324) and conducted according to the ethical guidelines of the Declaration of Helsinki, through which the informants’ autonomy, beneficence, non-maleficence, and justice were considered. 20 All informants received written and verbal information about the aim of the study and its realization, and informed consent was signed. Participants were also informed about the voluntary nature of participation and that they could choose to exclude themselves from the study at any given time without subsequent consequences.
Findings
The findings are presented through one overarching theme, which consists of the latent content. The findings are also presented in three main categories on the manifest content, each of which consisted of two sub-categories (Table 2).
Theme, categories, and sub-categories.

Note. MICM: Mobile Integrated Care Model.
Mutual trust is a prerequisite for nurses’ sense of safety and work satisfaction
Mutual trust was found to permeate the findings as a whole and was a pervasive component of the nurses’ sense of work satisfaction with the MICM. It could be understood that the mutual trust placed in the relationship with the MICM physician was a significant factor for the nurses to feel safe in the provision of health care. The MICM increased continuity and accessibility to the MICM physician, for the nurses and for the patients, which created a bridge on which mutual trust could be developed. Time was described to be needed to build trust between the nurse and the MICM physician. The nurses experienced that the MHCP made their work within home health care easier, and that the MHCP was a component that increased their sense of safety in the work toward the patient and next of kin.
The varying ways the MICM was implemented in the different municipalities resulted in a diversity of experiences. Lack of prioritization of the MICM by the organization appeared to interfere with accessibility, continuity, safety, and participation in decision-making, as well as with developing the health care (both for the home health care team, patient, and their next of kin). The relationship between the nurse and the MICM physician was also affected, and mutual trust was harder to build. The nurses’ participation in developing the MICM was rarely requested, which could be understood as a lack of mutual trust between the organizations and the nurses. If the nurse had high trust in their own ability, the trust in the MICM, the MICM physician, and organization did not appear to impact the nurses’ work satisfaction to the same extent.
A major goal for the nurses was to create a sense of safety in the provision of health for the patients in the MICM, which was achieved through creating trust. It could be understood that it was the small things the nurses did that created mutual trust between the nurses, patients, and their next of kin. The nurses experienced that the next of kin felt a sense of safety when they understood what the MICM included. From the nurses’ perspective, well-established mutual trust between them and the next of kin was associated with less need for the next of kin to have direct contact with the MICM physician.
Being the center of the MICM, with limited power to influence it
The nurses experienced that they worked more closely with the MICM physician than the other municipality personnel did. They also said that they worked more closely with the patients than the other health care professions did, which made them the center of the MICM. The nurses expressed that they lacked the opportunity to participate in developing the way the MICM physician worked and how the organizations prioritized the MICM. This created an obstacle in building mutual trust, and could in some cases affect the sense of safety and work satisfaction the nurses experienced.
The working conditions of the nurses are influenced by the MICM physician's ability to work for the patient as a whole
According to the nurses, having access to an MICM physician with the ability to work for the patient as a whole was remarkable, and the trusting relationship they built with the MICM physician created a base on which safety in health care rested. Nurses expressed that they had a hard time remembering how they worked before the MICM was implemented: My coworkers and I often say, ‘How did we manage before? How did we work before?’ (Nurse 13)
The MICM physician had a major impact on how the MICM was organized in the separate municipalities. The MICM physician decided where they would have their office, where rounds were conducted, and how communication would work. Accessibility to the MICM physician varied, from being highly accessible even outside of work hours to being almost impossible to reach outside of scheduled time. The MICM physician's ambition level and ability to view the patient holistically influenced the health care the patients received, as well as the working conditions of the nurses.
The nurses had different experiences of how the home visits were conducted and the MICM physician's holistic view of the patient. Some expressed that the MICM physician took time for the home visit and came well prepared. The nurses regarded this as important for safer health care. In other cases, lack of ability to have a holistic approach and lack of time led to the MICM physician not seeing the whole, and it made it harder for the nurses to create safe health care. It created frustration for the nurses, since they expected that the MICM physician should know how to conduct a home visit in their role: … the older person needs you to take things a bit calmer and you need to take it slow … but [the MICM physician] come out and it's like a small tornado and then [the nurse] have to go back and confirm if [the patient] understood everything, and they almost never did. (Nurse 11)
The nurses indicated that MHCP meetings conducted in consensus with the patient from a holistic perspective supported the provision of health care. Nurses expressed that some MICM physicians conducted the MHCP meetings in a way that made the MHCP less useful, since the MHCP at times was unsuccessful in considering the patient holistically. The perceptions of what had been discussed in the meeting could at times differ between the MICM physician, and the patient and their next of kin, which the nurses indicated depended on the MICM physician’s ability to express themselves. The nurses noticed that patients became irritated when they read the MHCP because they felt that the MICM physician had made decisions over their head, and trust was impacted.
A sense of powerlessness toward organizational prioritization
The MICM led to continuity for the nurses when they had the same MICM physician. Having the same MICM physician facilitated the building of a continuous trusting relationship, especially when the primary health care organization prioritized employing tenure physicians for the position. Nurses expressed that when the organization prioritized the MICM, the patient and their next of kin felt safe, since they knew the MICM physician. Feeling safe seemed to have a positive impact on the patients’ health and well-being. The nurses indicated that changing MICM physician created uncertainty and instability for the patient and their next of kin, as well as for themselves.
The nurses expressed that organizational prioritization could be an obstacle to working efficiently in the MICM. A sense of powerlessness arose in trying to have their voices heard, and there was a lack of mutual trust between the nurses and the primary health care organization. When employing a tenure MICM physician was not prioritized but instead locum physicians were employed, the nurses indicated that they often met with different physicians. When locum physicians were involved, matters regarding patients continuously had to be postponed, since they preferred not to make long-term decisions. This lack of continuity reinforced the nurses’ feelings of being the center of the MICM. They felt responsible for providing quality health care to the patient in the MICM, while feeling that their participation was limited in forming and developing the MICM. Patient admission to the MICM is based on prioritization in the primary health care organization in each municipality. The nurses indicated that patients admitted to the MICM were provided with safer health care.
The organization was perceived as prioritizing and endorsing MHCP meetings. Due to the need to prioritize MHCP and the MICM physicians’ fully booked schedules, it was difficult for the nurses to have the MICM physician conduct acute home visits. As a consequence, patients had to be sent into the emergency ward, which made the nurses feel powerless and lowered their work satisfaction. In some municipalities, the lack of access to an MICM physician made it impossible to prioritize MHCP instead of acute home visits. The nurses’ working conditions were influenced by time limitations because this led to stress and conflicts among the nurses in planning the MICM physician's time: The way we have it now, it's hard to manage the yearly checkups because there's a lack of time, and … you always have to do the acute. (Nurse 6)
The lack of access to each other's documentation, which is related to being part of a different organization, made the nurses feel less safe. The nurses also expressed a lack of medical equipment during MICM physicians’ home visits, since none of the organizations in the MICM prioritized buying them.
The team is key to quality health care
The nurses acknowledged that they could not conduct patient health care alone and that mutual trust needed to be formed with several professions from other fields. Teamwork was key to ensuring that the patients and their next of kin received quality health care. According to the nurses, the teams consisted of nurses, occupational therapists, physiotherapists, care administrators, and assistant nurses. The MICM physicians rarely collaborated with professionals other than the nurses, making them an outsider in the team:
The work around the patient cannot be done alone
Teamwork was key to ensuring quality health care for the patients, according to the nurses. The work around the patients admitted to home health care could not be carried out by nurses only. In some municipalities, there were organized meetings where the nurse met with the other team members regularly. One of the benefits of the team meeting was that different perspectives on patients’ situations were obtained from the professions in the team. It's about all professions … sitting multiple people and hearing the information at the same time, you can catch different questions that many I can't answer but another professional can. (Nurse 10)
In municipalities where team meetings did not exist, the nurses created other types of collaborations to create mutual trust with the other professions. Instead of teamwork, individual relationships were created between the nurses and select professions. The nurses expressed wanting organized team meetings: … we have requested to have more of those types of meetings, but we haven't really gotten to that … yeah I don't know what to blame really lack of time maybe. (Nurse 14)
The nurses felt they had a good relationship with the professionals in other disciplines, and that there was a mutual trust between them in the teamwork. The nurses highlighted that health care in the home was advanced, and it required good communication within the team to ensure quality of care.
The MICM physician as part of the team and yet an outsider
The nurses noticed that collaboration was good between MICM physicians and all health care professionals, although it was limited with any professionals other than the nurses. The MICM physician was seen by the nurses as part of the team, but they indicated that it was rare for the MICM physician to participate in the teamwork: It would be the most optimal way of working to have the entire team in one place. (Nurse 2)
In some municipalities, collaboration was non-existent. The nurses thought this could be remedied by an organized team meeting that included the MICM physician. They wanted the MICM physician to participate in the teamwork. The nurses thought it would give the whole team, including the MICM physician, an additional perspective. They also expressed that mutual trust could be built among all the professionals if they frequently met. Currently, the MICM physician was described by the nurses as more of an outsider or a consultant than a team member.
Increased possibilities for involving the patient and their next of kin
The MICM provided increased possibilities for the patient to be viewed as a person in a context, according to the nurses. They expressed that the patient felt safe in expressing their perspective on their health care in the MICM. The nurses’ approach to promoting the patient's and their next of kin's participation became the key to them being included in decision-making in their health care.
Being a guest in the workplace environment
Upon entering the patient's home, the nurse became a guest in their own work environment. Giving health care to the patient as a guest entailed that the health care was provided on the patient’s terms and conditions. The nurses expressed that the patients had more power in their homes, as opposed to traditional health care environments: When you step into someone's home, you always have to consider that you’re a guest in the home, all the time. I don't go in on my premise, I go in on theirs, the patient's and the next of kin's, at all times. (Nurse 10)
According to the nurses, it was easier for the MICM physician to come to the patient to make the MHCP than for the patients to go to the primary health care center, and the home was a safe place that facilitated discussing sensitive topics. The nurses experienced that the patients felt privileged to have an MICM physician come to their homes. The home environment increased the possibility for the patient and their next of kin to take part in planning their health care, which was seen by the nurse as positive and contributed to their work satisfaction. It's a lot of fun working in home health care really, and caring for the patients in the home. It's different from a hospital … it feels very meaningful. (Nurse 15)
Being in the patients’ homes enhanced the insight into the patients’ everyday lives and shortened the time needed for the nurses to get to know them, which made the nurses feel safer in providing the health care. The nurses expressed that the patients often felt lonely, unsafe, and worried in their home situation, living with health problems, but trusting health care helped increase their sense of well-being. When the patients were contented with the health care received, it increased the nurses’ work satisfaction.
The key to patient and next of kin participation is the nurses’ approach
The nurses’ approach to include the patient in their health care was key to the patient's and their next of kin's participation in providing, forming, and developing the health care. Some of the nurses expressed that their work was grounded in how crucial the patient's consent was in all aspects of health care. The nurses indicated that the next of kin often expressed feelings of safety about the health care given within the MICM when they were invited to participate in the provision of health care and the MHCP meetings: The next of kin is really a part of care giving … they’re a part of the whole. (Nurse 2)
Differing opinions between MICM physicians, nurses, patients, and their next of kin made it complicated to plan and execute health care, but it was ultimately still the patients’ decision in most cases. Next of kin were often more questioning than the patient, which was seen by the nurses as positive and contributed to safer health care when creating the MHCP. Another approach regarding patient participation was being flexible, and accommodating compromise. Some nurses expressed that they presented the options for the patients in a way that would direct the patient to a solution that the nurse thought was the safest. Other nurses stated that the patients did not participate in their health care at all and were not asked to participate in decision-making: Yes sometimes we’ve discussed whether [the patients] participate at all. (Nurse 10)
The nurses felt that it took time to build trust with the next of kin, and that trust was an area they actively had to work on. A lack of trust arose between the nurse and the next of kin when the next of kin expressed that health care did not meet the patient's needs. The nurses claimed that next of kin were often grateful for the health care their loved ones received, and the nurses perceived them as feeling safe in the MICM.
Discussion
The nurses in this study experienced that working in interdisciplinary teams to provide health care for older persons within their homes was valuable and entailed having access to competences from several professionals. Previous studies have claimed that interdisciplinary teams improve the efficiency of care for frail older persons, 21 and are indispensable for ensuring quality care. 22 The MICM nurses shared a similar experience, and they expressed that the work around the patient could not be done alone. The nurses described that the decision paths became shorter within the MICM interdisciplinary team, since the persons in the team knew each other and had built trust. Studies have shown that having good one-on-one relationships could deepen collaborations within an integrated team, 9 and knowing one's colleagues could create a feeling of stability, which leads to a sense of safety. 23 Joined care meetings offer the first step toward creating interdisciplinary integrated care, 9 and all members of the interdisciplinary team needed to invest time in the meetings to create a trusting relationship. 10 This could be a possible way to improve the MICM, since the results of this study show that the team around the patient consisted of several professionals, but that the MICM physician was most often not included in the team meetings. In their elaboration of the work they did within the team, the nurses explained that teamwork around the patient consisted of the personnel employed by the municipality, but the MICM physician seemed to be an outsider who worked almost solely with the nurse.
The MICM has its foundation in person-centered care. 24 Nurses expressed that working in the patient's home offered increased opportunities to see the patient as a person, and that it made learning to know them easier. Creating the MHCP together with the MICM physician as well as the patient and their next of kin was considered a way of capturing the patient's narratives. It was also a way of creating common goals, which are two of the three cornerstones of the person-centered care approach.13,14 None of the nurses brought up partnership with the patient as a part of the MICM, which is the third cornerstone of the person-centered philosophy. The nurses stated that some of the MICM physicians were attentive toward the patient's own narrative. However, the nurses also said that there were MICM physicians who were inattentive and made decisions against the will of the patient and next of kin. On such occasions, there was a risk of the MICM becoming patient-centered instead of person-centered. The difference between the two approaches is that the goal of patient-centered care is to create a functional life for the patient within their diagnoses, while person-centered care focuses on creating a meaningful life for the person with and outside of the care. 25 The results of this study imply a need to acknowledge and further explore the pervasiveness of person-centered care in the MICM organization. Person-centered care might need increased priority in the organization, perhaps through education in the person-centered approach, which is essential for the successful and sustainable implementation of person-centered care. 26 An alternative could be to give additional time to the MICM physician within the MICM, since the nurses expressed this as being an obstacle for working preemptively and planning the health care along with the patient. This can be seen in the light of a previous study 26 that claimed that it is important to ensure sufficient staff levels and professional competence in the workforce to safeguard person-centered care practices. It can also be suggested that organizations should prioritize employing MICM physicians who are interested in the health care of older persons. The MICM physician should also be interested in collaboration with the municipality team, since the MICM physician's ability to view the patient holistically impacts the way they work with the patient as a whole. Person-centered care has been shown to increase work satisfaction, employee productivity, and organizational commitment for employees in long-term care. 15 This partly aligns with the results of this study, which shows that nurses’ work satisfaction was influenced by being able to work for the patient holistically. The nurses expressed that when the patients were seen as a whole, the health care became safer, and trust was built among the professionals as well as with the patients and their next of kin.
Methodological considerations
Credibility, dependability, and transferability are three aspects of trustworthiness that can be measured in qualitative research.17,27 These aspects were used to secure and validate the findings in this study. The choice of participants can be considered a strength of the study's credibility, since the participants all worked in municipalities that had implemented the MICM at least six months prior to the study. The study's credibility was also strengthened by the close-to-the-text way of working with the data throughout the analysis, as well as by the back-and-forth analysis between the coauthors. The participants did not provide feedback on the findings, which can be seen as a limitation.
Dependability is described as the stability of the findings over time. 27 The data were collected in two parts to reach saturation, and no differences were observed in the findings from the different sets of interviews. The interviews in 2020 were conducted after restrictions from the COVID-19 pandemic had been implemented. Although COVID-19 has had an impact on home health care in many respects, the impact on the MICM was minor and hence did not seem to have an impact on the results.
The transferability of the findings of this study to similar or other contexts with regard to their generalizability is up to the reader. The participants were deemed as a relevant group to address the aim of how nurses experienced working within the MICM because of their experience, occupation, and workplace. The nurses’ experiences varied depending on where they worked. However, because of the different experiences, the findings show a range of how the MICM can be perceived, its strengths and weaknesses, and how to develop and improve the MICM from the nurses’ perspective.
Conclusion
A trusting collaboration with an MICM physician created work satisfaction for the nurses working within the MICM, when the health care became person-centered. The right members of the team are paramount to ensuring that the MICM functions as intended, and to facilitate building mutual trust between the health care professionals and the patient and their next of kin. The MICM is grounded in person-centered care. However, the extent to which this foundation permeates the MICM seems in part to depend on the MICM physician's ability to work with the patient as a whole, the possibility of creating a coherent team and having enough time, which is set by the prioritization from the organization. Exploring the experiences of other health care professionals working within the MICM, as well as the experiences of patients and their next of kin on receiving care within the MICM, can therefore ensure capturing the views of those whom the MICM affects the most. Nurses working within the MICM expressed that they did not want to go back to the way they worked before, and they acknowledged that the MICM was preferred to the previous way of working. The most prominent suggestion for improvement was increased time for the physician within the MICM.
Footnotes
Acknowledgements
The authors would like to thank the participating nurses. They would also like to thank the master students who participated in the data collection process.
Ethical approval statement
The project was approved by the Ethical Review Authority (Dnr 1020-17; 2019-02563; 2020-04324), and conducted according to the ethical guidelines of the Declaration of Helsinki.
Author contributions
The first author was responsible for the data analysis and drafted the manuscript. The second and last authors designed the study. The first, second and fourth authors collected the data. All authors contributed to the analysis and the intellectual content of the manuscript.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from The Kamprad Family Foundation for Entrepreneurship, Research & Charity in Sweden (20190175). It was also supported by the School of Health Sciences, University of Skövde, Sweden; the Skaraborg Institute for Research and Development; The foundation in memory of Gösta Svensson.
Supplemental material
Supplemental material for this article is available online.