
Abstract
Human immunodeficiency virus (HIV) infection is now preventable with pre-exposure prophylaxis (PrEP) drugs, however, barriers to PrEP implementation include primary-care physician (PCP) knowledge-gap and lack of comfort prescribing and managing PrEP. We hypothesized that integrating HIV-PrEP education during medical-residency would help address these problems and developed a 40-minute case-based lecture focused on the 2021 United States Preventative Services Taskforce (USPSTF) oral HIV-PrEP guidelines and integrated this into our residency’s core curriculum. We analyzed data from physician-trainees who voluntarily completed a pre- and post-lecture survey measuring HIV-PrEP “knowledge” and “self-assessed readiness to independently initiate and manage PrEP.” Independent group analysis was completed via the Mann-Whitney U and Pearson Chi-square 2-sided test with P-value <0.05 deemed significant. Of the total of 189 residents invited to the lecture, 130 (69%) completed the pre-survey while 107 (57%) completed the post-survey. Per knowledge-assessment: the median number of correctly answered questions rose from a pre-lecture baseline of 4/9 (44%) to 8/9 (89%) following the education intervention (P < .001). When asked about comfort initiating and managing HIV-PrEP on their own, 7/130 (5.4%) responded in agreement pre-lecture, but this rose to 55/107 (51.4%) post-lecture (P < .001). Our study revealed PrEP training during residency was effective per stated objectives and may be an important tool to increase PrEP delivery/uptake to achieve the target goals for the National HIV/AIDS Strategy.
Keywords
Introduction
Infection with the human immunodeficiency virus (HIV) is preventable with use of HIV pre-exposure prophylaxis (PrEP) medications. When taken as prescribed, PrEP reduces the risk of HIV transmission by 99% through sexual contact and at least by 74% through intravenous drug use (IVDU).1,2 In the USA, the Food and Drug Administration has approved oral TDF/FTC (Truvada), TAF/FTC (Descovy), and more recently intramuscular cabotegravir for HIV-PrEP purposes; however research has identified individual, structural, and health-systems barriers that contribute to suboptimal PrEP delivery and uptake. 3 Together, these barriers contribute to ongoing new HIV infections in the USA with 37 968 new cases reported in 2019, with the greatest incidence in sexual and racial minorities.4,5
The focus of this study is to address modifiable factors within the health-system, in particular provider-level barriers to HIV PrEP uptake. In the USA, despite widely published HIV-PrEP management guidelines, barriers frequently cited by primary care physicians (PCP) include PrEP knowledge-gap and lack of comfort prescribing and managing PrEP. 6 A 2017 study comparing practicing PCP and HIV specialists in 10 USA cities with the greatest HIV prevalence showed that fewer PCPs than HIV specialists had heard of PrEP (76% vs 98%), felt familiar with prescribing PrEP (28% vs 76%), or had prescribed it (17% vs 64%). 7 A 2022 published survey of 351 general health providers in the Southeastern US, a region disproportionately affected by the HIV epidemic, supported a need for provider training as the average PrEP knowledge scores were 2.6 out of 5 and was negatively associated with increasing numbers of years providers worked in their clinical role. The study also reported significantly low provider self-efficacy scores with PrEP initiation as it pertains to medication prescribing and insurance navigation. 8 Conversely, other studies have linked factors such as increased knowledge with greater PrEP prescribing behavior and/or intention/willingness to prescribe PrEP by healthcare providers serving at-risk adolescents or adults.9-11 Unfortunately this has not systematically transformed the PrEP education offerings available to primary care physicians who are often at the frontlines of community health with great access to individuals who may be eligible for HIV pre-exposure prophylaxis.
Our literature review of the availability of formal PrEP medical training in the USA revealed a scant and non-uniform process driven primarily by individual academic training programs. A 2021 study that attempted to survey all 141 USA medical schools for PrEP training activity yielded a 50.4% (n = 71) program participation rate with only 38% (n = 28) of respondents endorsing having some form of PrEP training. 12 There is less literature on the widespread practice of PrEP education after medical school (ie, residency/fellowship); perhaps the best nationwide survey came from a 2018 survey of family medicine residency programs which revealed that 52% of its 246 programs had “some PrEP training” with only 13.8% of these reporting significant PrEP training. 13 Nevertheless, some published observational studies and training pilots have shed a positive light on the utility of adopting an HIV-PrEP training intervention. For example, a 2016 survey of 229 internal medicine residents at five tertiary academic medical centers (Johns Hopkins Hospital, Johns Hopkins Bayview Medical Center, Yale School of Medicine, University of Washington, and The Ohio State University) showed that only 25% (n = 51) of residents had received prior PrEP training. Compared to those without PrEP training, those previously trained performed significantly better on knowledge scores, were more likely to prescribe PrEP, and had higher comfortability screening, educating, and monitoring a patient on PrEP. 14 A 2018 pilot of a brief focused PrEP education intervention at the University of South Carolina medical program also yielded trainees with significantly higher knowledge scores and greater comfort recommending PrEP. 15
With these positive trends, we sought to add to the body of literature by designing, implementing, and reporting training outcomes from an HIV-PrEP education intervention within our large urban academic training program which is located in Cleveland, within Cuyahoga County, Ohio. Cuyahoga County has one of the highest new HIV diagnosis rates in the state of Ohio prompting our intervention. 16 We postulated that standardizing and integrating HIV-PrEP training during medical residency would prepare trainees with the knowledge and confidence to initiate and manage PrEP in the community.
Methods
Design and Intervention
In this cross-sectional study, our study investigators developed a case-based 40 minute lecture and generated a 10 minute, 10 questions survey based on the 2021 United States Preventive Services Taskforce (USPSTF) HIV-PrEP guidelines (see Supplemental Table 4 below for full survey). Course content educated trainees on how to: (a) competently screen for patients at high risk of HIV acquisition including sexually active adolescents, men or women with sexually transmitted infection (STI) in past 6 months, men who have sex with men (MSM), persons engaging in sex without condoms with persons of unknown HIV status, HIV sero-discordant couples, and persons who inject drugs and share needles, (b) initiate and/or refer to start TDF/FTC (Truvada) or TAF/FTC (Descovy), and (c) manage HIV-PrEP long term within the outpatient setting. The survey questions were investigator generated and were based on the 2021 USPSTF PrEP guidelines content and it was designed to measure our 2 primary outcomes. Nine questions surveyed HIV-PrEP knowledge and one question assessed self-reported readiness to independently initiate and manage PrEP, a proxy for provider confidence. We incorporated these into a 1-hour long HIV PrEP course and integrated this into both the internal medicine and pediatric residencies’ core ambulatory curriculum schedule. Lecture attendance was mandatory for its educational benefits, however trainees could voluntarily consent to participate or decline in taking the online survey questionnaire in the first 10 min before the 40 min lecture and also again in the last 10 min after lecture was completed. The PrEP class was taught remotely due to social-distance requirement in a virtual classroom format in 8 group sessions between March and May 2022 such that each rotating physician-trainee could attend the lecture once. PrEP lectures were taught by the first author (M.O.O), a dual board-certified Internal Medicine and Pediatrics physician and Pediatric infectious disease fellow, and the University Hospitals’ HIV-PrEP navigator (F.A).
Inclusion and Exclusion Criteria
A total of 189 pediatric, internal-medicine, and combined internal medicine-pediatric (Med-Peds) residents across all training levels were electronically invited to participate in the pre/post surveys. Inclusion criteria encompassed all residents actively enrolled in the pediatric, internal medicine, and Med-Peds residency program between the March and May 2022 period. Excluded were non-residents (ie, medical students, fellows, attendants, and independent practitioners), other specialties, and any residents who opted out of the survey.
Primary Outcomes
For HIV-PrEP knowledge: the total number of correctly answered questions were tallied and compared between pre and post-test groups. Data was analyzed by the overall group and by 2 subgroups: the “Pediatric + Med-Peds” group which comprised of the categorical pediatric and the minority group of Med-Peds trainees who completed their PrEP class together and the “ Internal Medicine” group who comprised the categorical adult internal medicine group. The null hypothesis was that there would be no difference in pre/post knowledge outcomes with this education intervention. Unpaired independent group analysis was completed via an independent Mann-Whitney U 2-sided test (due to non-normal distribution) with P-value of less than 0.05 considered significant to reject the null of no difference.
For HIV-PrEP self-assessed readiness: To assess this, physician-trainees where asked to select a response to the statement “I feel comfortable initiating and managing HIV Pre-Exposure Prophylaxis on my own” using options: “Agree,” “Neutral,” or “Disagree.” Responses were compared pre and post training intervention.
Analysis
Analysis was achieved using the IBM SPSS Statistics for Windows, version 28.0 (IBM Corp., Armonk, NY, USA). For the primary outcomes of HIV PrEP knowledge and readiness to prescribe PrEP, the dichotomous responses were compared and analyzed pre and post lecture using a Pearson Chi-square 2-sided test with P-value of less than 0.05 considered significant to reject the null of no difference from the education intervention. Furthermore, we generated an unadjusted odds ratio via binary logistic regression to determine if readiness was dependent on the 2 trainee groups: “Pediatric + Med-Peds” and “Internal Medicine.”
Data Analysis and Privacy
The survey was disseminated, and data collected and managed, using REDCap, an electronic data capture tool, hosted at University Hospitals with the support of the CTSC grant (1UL1 RR024989 from NCRR/NIH).17,18 The study was approved via the regulatory University Hospitals IRB. Data sharing is available upon request.
Results
Overall Group Characteristics
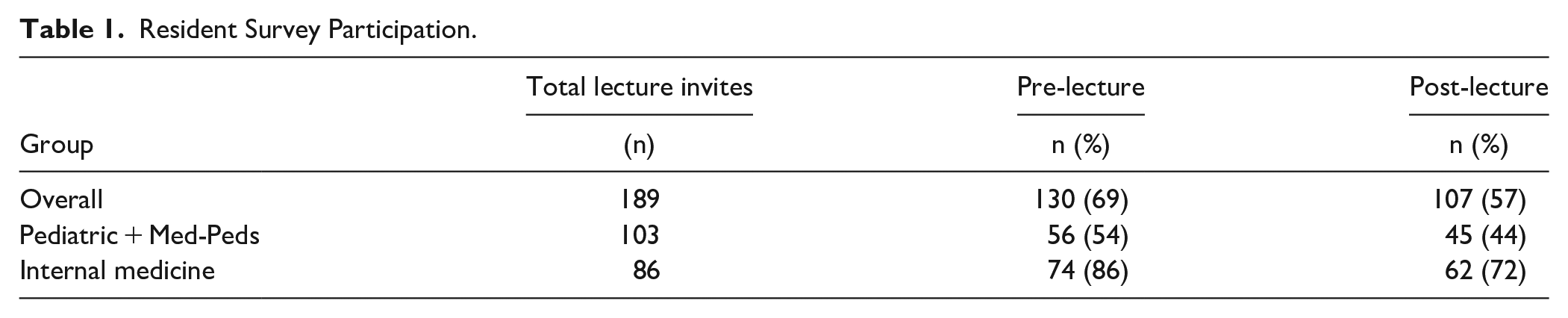
For this study, of the total of 189 pediatric, internal-medicine, and Med-Peds residents, 130 (69%) completed the pre-survey while 107 (57%) completed the post-survey. Table 1 shows the overall participation rate and by specialty grouping.
Resident Survey Participation.
Outcome I: HIV-PrEP Knowledge
The median number of correctly-answered questions in the overall pre-lecture group was 4/9 (44%). Following the education intervention, this significantly rose to 8/9 (89%) in the post lecture group (P < .001, U = 378). The median correctly-answered scores significantly rose as well across each subgroup after the education intervention. (Table 2).
Mann Whitney U Comparison of Correct Answers Pre and Post Lecture (Range 0-9).

Outcome II: Self-Assessed HIV-PrEP Readiness
When asked to respond to the statement “I feel comfortable initiating and managing HIV Pre-Exposure Prophylaxis on my own,” only 7/130 (5.4%) resident pre-lecture could confidently respond in agreement. However, after the education intervention, this significantly increased to 55/107 (51.4%; P < .001, χ2 = 64.341) as shown in Table 3. Further sub-analysis was conducted using binary logistic regression to determine if confidence was dependent on trainee group. Despite prior demonstrated similar knowledge-gain post-lecture, this analysis showed that the “Pediatric+Med-Peds” group reported significantly lower self-efficacy in initiating and managing PrEP compared to the “Internal Medicine” trainees, likely suggesting lower confidence among “Pediatric+Meds-Peds” trainees in this domain (unadjusted OR = 0.383, 95% CI: 0.174-0.845, P = .017).
Self-Assessed HIV-PrEP Initiation and Managing Readiness Pre and Post Lecture.

Discussion
The Joint United Nations Program on HIV and AIDS published its global mission of getting every country and every community on track to end AIDS as a public health threat by 2030. 19 Central to achieving this mission, communities must have access to preventative tools such as HIV-PrEP and the medical providers that manage these medications. However, within the USA, we find that PCPs often cite HIV-PrEP knowledge deficit and lack of comfort managing PrEP as a barrier to implementing PrEP which limits vital access. Our literature review of PrEP education offerings in medical schools and beyond showed that HIV PrEP training is inadequate and non-uniform. This likely explains our baseline survey findings of a somewhat low HIV-PrEP based knowledge (median correct score 4/9, 44%) coupled with an even lower confidence in PrEP initiation and management (5.4%). This pattern possibly reflects the known rising provider-awareness but low prescribing PrEP behavior described in the literature.3,6-8,20
Moving beyond this status quo to graduating well informed and confident general providers suggests a need for an educational intervention. Our study demonstrated that incorporating HIV PrEP curriculum during medical residency is feasible and beneficial with good planning. With a single and short focused 40 minute training intervention, we significantly increased residents’ HIV PrEP knowledge (median correct score 8/9, 89%) and self-efficacy to initiate and manage HIV-PrEP (51.4%) post intervention. This validates an increasing number of studies with similar positive rise in HIV-PrEP knowledge and prescriptive behaviors with educational intervention.13,15,21,22 With this growing body of evidence, we believe that there should be consideration of the routine inclusion of HIV-PrEP education as part of graduate medical education (GME) during medical residency. The medical-residency period is ideal as this setting is readily amenable to both classroom and practical training opportunities. Furthermore, given its requirement for independent clinical practice, residency easily captures all matched trainees who may have lacked prior HIV-PrEP training during medical school. If utilized, the medical residency training period can be a fertile preparative ground to empower future physician-graduates with the HIV-PrEP knowledge and the confidence they need in the fight to eradicate new HIV transmission in the community.
Our training outcomes additionally revealed some opportunities for improvement. We found that while residents’ HIV-PrEP knowledge significantly rose to a median knowledge score of 8/9 (89%) post intervention (Table 2), this was accompanied by a relatively low self-efficacy score of 51.4% in initiating and managing HIV-PrEP post intervention (Table 3). To increase self-efficacy/confidence, our literature review findings suggest that offering adult learners practical interactive experiences through hands-on or precepting opportunities can help enhance learning; and when compared to traditional didactic teaching alone, is more effective in changing physician practice performance.23,24 Today, experiential learning is a well-integrated foundational technique for building clinical competencies in medical education. This approach can be equally applied during HIV-PrEP training by scheduling learners to precept in HIV-PrEP clinic rotations and by pairing learners with Infectious Diseases doctors who manage PrEP. In his review of medical education literature Tolsgaard et al, 25 demonstrated that the social interactions and observation with feedback opportunities between a learner and a more knowledgeable peer can positively impact learners’ new knowledge gain, self-efficacy and motivation, which in turn may affect subsequent learning and performance. Finally, a 2014 to 2018 survey of current and former family-medicine residents revealed that the majority (84%) rated precepting as the most effective tool for building their competence. 22 In retrospect, given our disparate final scores in knowledge and self-efficacy outcomes, we believe our training intervention could have potentially benefited by incorporating a practicum approach/element.
Our study strengths include our residents’ robust participation rate and a simple curriculum design based solely on the freely available online CDC HIV-PrEP guidelines. As far as we know, our study represents the first to investigate HIV-PrEP training outcomes within such a large group of exclusively medical-residents who are training in a high HIV transmission region in the USA. Our study has a few weaknesses: it utilizes an unpaired analysis design, relies on a self-assessed report of self-efficacy which can introduce bias, and was conducted at a single institution which may affect generalizability. However, we submit that our study population is representative, and our training design is simple and easily replicable across most academic institutions. Finally, while this study focuses on improving provider-level barriers, there are also other important patient-level and structural barriers that may additionally impede PrEP uptake that should not be overlooked. For example, a recent 2023 publication of a cross-sectional survey of 134 primary care providers in rural and suburban practices in a large Pennsylvania academic institution cited that the largest barrier to PrEP prescribing was the “lack of PrEP training and education”, however, it also included lack of patient insurance coverage for PrEP-related care, and lack of organizational level support such as access to clinic guidelines and protocols and costs, as well as staffing and time constraints to provide necessary risk reduction and PrEP adherence counseling. Facilitators of PrEP prescribing endorsed by these same health providers included use of order set in the electronic medical record (EMR) that guided recommended PrEP testing, peer and clinical pharmacist support, and access to guidelines and protocols. We believe that this article appropriately advocates for a multifaceted approach to enhancing PrEP delivery that goes beyond isolated provider knowledge acquisition. 26
Further research is still needed to investigate the cost of incorporating HIV PrEP training during medical residency in the USA. Anticipated burdens include need for trained faculty and support staff to teach this course and support new trainees and PrEP patient enrollees, as well as the need to allocate protected time and PrEP clinics to train residents. More research is also needed to demonstrate the short and long term efficacy of this educational intervention on trainees’ PrEP practice behavior before and after graduating from residency. Finally, more research is needed on how best to integrate HIV-PrEP training into continuing medical education (CME) and incentivize the practice of HIV-PrEP competencies in the current working pool of independent primary care providers, non-physicians and midlevel providers already serving in the community.
In conclusion, our study results support that PCPs’ knowledge-deficit and lack of comfort prescribing HIV-PrEP are modifiable factors in the comprehensive approach to enhance HIV PrEP delivery and uptake. Academic programs can offer HIV-PrEP focused classroom and practicum training opportunities during medical residency to prepare future medical providers with the recommended HIV-PrEP competencies to reduce new HIV transmission in the community. Increasing the knowledge of HIV and prevention strategies among the health workforce is an actionable item listed in the National HIV/AIDS Strategy Federal Implementation Plan. 27 The cost of instituting HIV preventative training interventions during medical residency should be weighed with the potential innumerable benefits of realizing a healthier society with less incidence of HIV/AIDS and its associated morbidity and mortality.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319231207313 – Supplemental material for Integrating HIV Pre-Exposure Prophylaxis (PrEP) Education During Medical Residency: Training Outcomes and Suggestions for Learning Effectiveness
Supplemental material, sj-docx-1-jpc-10.1177_21501319231207313 for Integrating HIV Pre-Exposure Prophylaxis (PrEP) Education During Medical Residency: Training Outcomes and Suggestions for Learning Effectiveness by Matilda Olajumoke Ogundare, Fiona Allan, Ankita P. Desai, Sahera Dirajlal-Fargo, Nori Mercuri Minich and Barbara M. Gripshover in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The Pediatric and Internal-Medicine Departments Leadership and 2021 to 2022 Chiefs for helping coordinate the system-wide curriculum, Sheree Hemphill for REDCAP database design, UHCMC/RBC Pediatric Infectious Disease Scholarly committee for research support, and the participating physician-trainees at UHCMC/RBC in the study.
Author Contributions
Matilda Olajumoke Ogundare: Contributed to project and curriculum design, IRB application, course implementation, data collection, analysis, and manuscript write up. Fiona Allan: Contributed to curriculum design and course implementation. Nori Mercuri Minich: Contributed to analysis and write up contributions. Mentor 1: Barbara M. Gripshover: Contributed by supervising and providing input to project and curriculum design, IRB application, course implementation, data collection, analysis, and manuscript write up. Mentor 2: Ankita Desai: Contributed by supervising and providing input to project and curriculum design, IRB application, course implementation, data collection, analysis, and manuscript write up. Mentor 3: Sahera Dirajlal-Fargo: Contributed by supervising and providing input to project and curriculum design, IRB application, course implementation, data collection, analysis, and manuscript write up.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.