
Abstract
Introduction:
The COVID-19 pandemic has disproportionately affected some New York City (NYC) neighborhoods that primarily consist of Black, Indigenous, and Latinx residents. In comparison to the rest of NYC, these neighborhoods experienced high hospitalization and COVID-related death rates, which has been attributed to a longstanding history of structural racism and disinvestment. While stay-at-home orders were implemented to reduce the spread of COVID-19, this may have also affected access and utilization of non-COVID related healthcare services. This study aims to assess the prevalence of and reasons for the disruption of non-COVID related healthcare services during the first 18 months of the pandemic.
Methods:
From September 30, 2021 to November 4, 2021, the NYC Health Department administered the COVID-19 Community Recovery Survey to a subset of residents who were part of the NYC Health Panel a probability-based survey panel. This cross-sectional survey, which included closed and open-ended questions, was either self-administered online or completed via CATI (Computer Assisted Telephone Interviewing) in English, Spanish, and Simplified Chinese. Descriptive statistics were used to summarize responses and unweighted, weighted, age-adjusted percentages, and 95% Confidence Intervals (CIs) were calculated.
Results:
With a response rate of 30.3% (N = 1358), more than half of participants (54%) reported disruption to either routine physical healthcare or mental health services. Concern about getting COVID-19 (61%), stay-at-home policies (40%), belief that care could safely be postponed (35%), and appointment challenges (34%) were among reasons for delaying routine healthcare. Concern about getting COVID-19 (38%) and reduced hours of service (36%) were primary reasons for delaying mental healthcare. Reported reasons for the sustained delay of care past 18 months involved COVID concerns, appointment, and insurance challenges.
Conclusions:
Due to the pandemic, some disruption to healthcare was expected. However, most study participants either avoided or experienced a delay in healthcare. The delay of non-COVID related healthcare throughout the pandemic may result in the further widening of the health inequity gap among NYC residents dealing with a higher chronic disease burden before the start of the COVID-19 pandemic in March 2020. Findings from this study can support equitable COVID-19 recovery, and guide efforts with health promotion.
Introduction
To mitigate COVID impact early in the pandemic and the subsequent COVID-19 case surges, public health messaging advised avoiding unnecessary healthcare visits to reduce transmission of COVID-19 and ensure the capacity of healthcare facilities.1 -3 Additionally, health service providers were advised to implement social distancing policies and operate remotely as much as possible.4,5 The New York State on PAUSE (Policies that Assure Uniform Safety for Everyone) executive order to close all non-essential businesses went into effect in March 2020, which emphasized the need to stay home until stay-at-home orders were lifted in May 2021. 6 While these measures are credited with reducing the spread of COVID-19 infection, there may have been unintended consequences on healthcare access and utilization for routine and preventative physical and mental healthcare beyond intended emergency measures. 7 For example, according to a survey conducted in August 2021, 28% of New York City (NYC) residents who had regular visits with a healthcare provider for hypertension prior to March 2020 had either reduced the frequency or stopped receiving care. 8 The survey also found that since March 2020 about 40% of NYC residents postponed cancer screenings and 13% delayed needed mental health treatment. Missed or delayed healthcare, especially during a pandemic, can have negative health implications among already vunerable populations living in NYC.
To gain a better understanding of the impact COVID-19 had within specific NYC neighborhoods and to support place-based approaches to recovery, the COVID-19 Community Recovery Survey was administered. Previous studies have measured changes in medical care during the pandemic using electronic health records (EHR), insurance claims data, and national surveys using a representative sample.9 -11 This paper adds to the literature by investigating the estimated magnitude and common barriers to the delay in routine physical and mental health care among residents of historically disinvested NYC neighborhoods.
Methods
Study Location
When compared to other U.S. states, districts, and territories, New York City (NYC) has been disproportionately affected by the COVID-19 pandemic. 12 On the neighborhood level, infection, hospitalization, and death due to COVID-19 have been especially prevalent in communities with primarily Black, Indigenous, and/or Latinx residents.13,14 The pandemic also exacerbated social and economic conditions, with Black and Latinx NYC residents reporting higher rates of unemployment and difficulty paying for food and housing expenses in comparison to their White counterparts. 15 These inequities are attributable to structural racism, and other systems of oppression, including pervasive community disinvestment through the application of austerity measures.
To address these longstanding neighborhood-based health inequities, the NYC Department of Health and Mental Hygiene (NYC Health Department) operates the Bureaus of Neighborhood Health (BNH), which are located in, and seek to center and serve residents of historically disinvested neighborhoods in North and Central Brooklyn, South Bronx, and East and Central Harlem (Figure 1). Most of these residents identify as Black, Indigenous, and/or Latinx. Prior to the pandemic, residents of the Brooklyn, Bronx, and Harlem BNH catchment areas experienced higher rates of chronic diseases compared to NYC averages. 16 These neighborhoods were also disproportionately impacted by the COVID-19 pandemic. From February 2020 to October 2021, the age adjusted hospitalization rates within the BNH Brooklyn (1352/100 000), Bronx (1712/100 000), and Harlem (1306/100 000) catchment areas were all higher than overall NYC rates (1105/100 000). 17 During the same time period, all 3 BNH areas demonstrated higher age-adjusted death rates (Brooklyn BNH: 387; Bronx BNH: 444; Harlem BNH: 325 vs NYC: 271/100 000 people).

Geographical map of the bureaus of neighborhood health (BNH) catchment areas in New York City.
Study Design and Participant Recruitment
The COVID-19 Community Recovery Survey is a cross-sectional survey, which was fielded from September 30, 2021, to November 4, 2021, and was either self-administered online or completed via CATI (Computer Assisted Telephone Interviewing) with a trained NYC Health Department interviewer over the phone. Study participants were recruited from the NYC Health Panel (formerly known as Healthy NYC), a probability-based survey panel of 13 014 adult New Yorkers at least 18 years old. The NYC Health Panel was established in the spring of 2020, supplementing existing population-based health surveys and conducting surveys in-house instead of contracting with a vendor, which allowed for quicker access to data. 18 Sampling and recruitment methodology of the panel has already been detailed and can be found in Dasgupta et al. 19
NYC Health panelists were eligible to take part in the COVID-19 Community Recovery Survey if they lived in 1 of the 3 BNH catchment areas at the time of registration in the NYC Health Panel. Specifically, participants had to live in 1 of 12 Community Districts or 1 of 25 ZIP code tabulation areas which define the geographic boundaries of the catchment areas, resulting in 4478 eligible panelists. All eligible panelists were sent invitations by mail, email, and text, with each participant receiving between 3 and 6 contacts. Of the 4478 eligible panelists, 1358 unique participants completed the COVID-19 Community Recovery survey, for a response rate of 30.3%, which factors in the number of invitations sent to eligible panelists. The survey was offered in 3 languages, specifically, English, Spanish, and Simplified Chinese (Mandarin and Cantonese by phone), and participants received a $10 gift card for their time.
Research Ethics
This study was approved by The New York City Department of Health and Mental Hygiene (NYC DOHMH) Institutional Review Board (IRB; #21-053). After being informed on the purpose of this study, online participants gave their explicit consent by checking the box that affirmed they have read and understood the information presented to them on the electronic consent form. Participants who completed the survey by phone provided verbal consent. Personal information was anonymized and all methods were performed in accordance with the relevant guidelines and regulations.
Measures
The survey included 6 sections: impact of the COVID-19 pandemic on general healthcare, prescriptions, and mental health; attitudes toward COVID-19 vaccines and knowledge of NYC COVID-19 testing services; perceived community resilience and assets needed for recovery; trust in local government; social determinants of health; and linkage to their local BNH. Participant demographics were collected during the NYC Health Panel registration in September 2020 or May 2021, with additional measures collected at the time of the survey.
Measures presented in this paper focus on results related to the impact of the pandemic on routine care and mental healthcare including questions about delayed physical and mental healthcare during the pandemic, type of delayed care, and reasons for delayed care.20,21 A series of questions were created which included questions that were adapted from a pre-existing NYC Health Department survey assessing delayed care, and newly developed questions—all underwent cognitive testing.20,21 The delay of routine physical health care was defined by the following question: “Since March 2020, when the COVID-19 pandemic began in NYC, have you avoided or delayed any routine physical health care such as an annual check-up, care for a chronic condition, cancer screenings, pre- or post-natal care, regular vaccinations or dental care?” Those who responded “yes” were then asked to identify the types of care they missed from a response list, with the option of writing-in a response. They were then prompted to identify reasons for delayed care from a list, with the option of writing-in a response. There were questions asking those who had delayed care whether they had received the care they needed by the time of the survey in October 2021, followed by an open-ended question asking those who had not yet received care to explain why not. Adapted from the Olmstead County COVID-19 Impact Survey and the aforementioned NYC Health Department survey, avoiding or delaying mental healthcare was determined by the following question: “Since March 2020, when the COVID-19 pandemic began in NYC, was there a time when you needed mental health care but did not get it or delayed getting it?”20,22 Mental healthcare was further defined as counseling, therapy, medication management, social work services, peer supports, and substance use disorder treatment. Similar to routine physical healthcare questions, those who responded “yes” had to identify a reason for missed or delayed care and report whether they were currently receiving the needed mental healthcare.
Weighting and Analysis
Survey data were weighted to the residential adult population in the defined geographic area of interest using 2015 to 2019 American Community Survey (ACS) 5-year estimates at the ZIP Code Tabulation Area (ZCTA) level, and Public Use Microdata Area (PUMA) level to match the total number of households in the BNH catchment areas as well as the distribution of demographic characteristics. The sum of the survey weights equals 1 056 184, which is the 2019 estimate of the total residential adult population in the BNH geographic catchment area.
Descriptive statistics were used to summarize responses. For dichotomous and categorical variables, unweighted, weighted, age-adjusted percentages, and 95% Confidence Intervals (CIs) were computed. Using deductive and inductive coding approaches, open-ended responses about reasons for continued delayed care was initially coded separately by a primary and secondary analyst who then met to discuss any disagreements in coding. A final review of coding was conducted by a third analyst. A new variable was then created to include the final counts of both the closed-ended and open-ended responses. Quantitative analyses were conducted in SAS Enterprise Guide 7.115 and SAS-Callable SUDAAN. Microsoft Excel was used for open ended response coding and to create figures and tables.
Results
Of the 4478 invited panelists, 1358 unique participants completed the COVID-19 Community Recovery Survey (1181 online and 177 by phone), for a response rate of 30.3%.
Study Population
Demographic characteristics of all survey participants are presented in Table 1. There were 1358 survey participants living in the Brooklyn (30%), Bronx (32%), and Harlem (39%) BNH catchment areas. Most participants were aged 25 to 64 years (75%), and 39% were Latinx, 33% were Black, 20% were White, 6% were Asian, and 4% were either multi-racial or identified as another race. Most participants identified their gender as a woman (72%), and about 45% were from multi-lingual or non-English speaking households. Fifty-two percent of participants were living below the 200% federal poverty level and 92% had health insurance.
Characteristics of COVID-19 Community Recovery Survey participants, N = 1358.

The acronym FPL stands for Federal Poverty Level.
Denotes that data should be interpreted with caution. Estimate is unstable because the standard error represents more than 30% of the estimate.
Delayed or Avoided Routine and/or Mental Healthcare
Between March 2020 and October 2021, 54% of all participants reported delaying or avoiding either their routine physical healthcare visit or needed mental health services, which is reflected by an approximate 559 258 people living across the BNH areas (Table 2). Among those who reported some disruption, 11% reported delaying both, representing 107 008 BNH residents.
Delayed Routine Physical and Mental Healthcare Among COVID-19 Community Recovery Survey Participants, N = 1358.
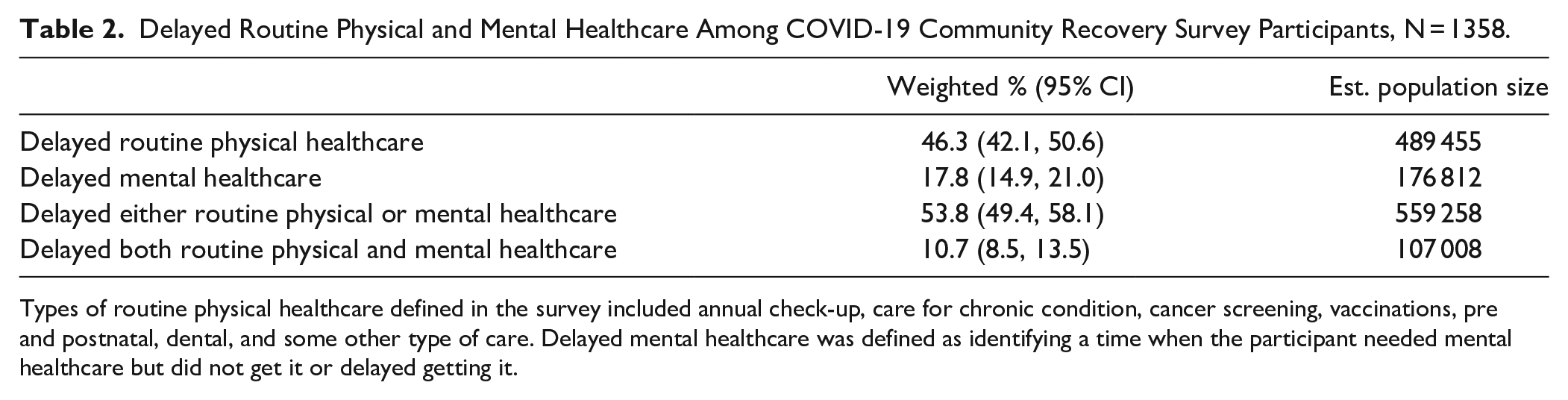
Types of routine physical healthcare defined in the survey included annual check-up, care for chronic condition, cancer screening, vaccinations, pre and postnatal, dental, and some other type of care. Delayed mental healthcare was defined as identifying a time when the participant needed mental healthcare but did not get it or delayed getting it.
Delayed or Avoided Routine Healthcare
Forty-six percent of survey participants had reported avoiding or delaying routine care since the COVID-19 pandemic began, which represents around 489 455 residents (Table 2). There were similar findings of missed routine care across all 3 BNH areas. Among survey participants who delayed routine healthcare, the most common types of delayed care were annual check-ups (78%) and dental appointments (75%; Figure 2). Approximately 33% of those who delayed routine healthcare had delayed a cancer screening, with breast cancer being the most common type (59%). Thirty-four percent of survey participants delayed regular care for a chronic condition, including high blood pressure, diabetes, heart disease, asthma, HIV, or cancer. Routine vaccinations (eg, influenza, pneumonia, or shingles vaccines) were delayed by 37% of survey participants and 12% delayed their perinatal care. Twenty-five percent reported delaying other types of care (eg, gynecology, optometry, podiatry, and physical therapy).

Types of delayed routine physical care among survey participants in the COVID-19 Community Recovery Survey, N = 1358.
When asked to explain reasons for avoided or delayed care, 61% of survey participants mentioned concerns about getting COVID-19 (Table 4). The next most common reason cited was following instructions or guidance to stay home (40%), followed by their provider’s office either being closed or having a reduced schedule (36%). Thirty-five percent of survey participants believed that their routine healthcare could safely be postponed. Some found that there were no available appointments from their provider when they sought out care (34%), which impacted more than 164 000 BNH residents (not shown). Twenty-one percent of survey participants felt that offered telehealth options did not work for them, 14% of residents delayed care due to cost, while 6% cited other reasons.
Sustained Delays in Routine Healthcare
Fifty-five percent of survey participants who reported delaying a cancer screening still had not received a needed cancer screening by October 2021 (Table 3). Of those who delayed a vaccination, 56% still hadn’t received it. The prevalence of sustained delay in needed care was similar among those who needed dental care (57%), which represents more than 203 000 BNH residents. Of those who reported delaying an annual check-up, 42% hadn’t received it, and among those who hadn’t received care for a chronic condition, 31% hadn’t received it at the time of the survey. The most common reasons for continued delay of care among survey participants were challenges with appointment availability (21%), concerns about getting COVID-19 (18%), and navigating health insurance (12%). Other reasons included their busy schedule (10%), cost (9%), and finding a new provider (8%) (Table 4). While 26% of study participants cited other reasons, 9% of survey participants did report that they had scheduled an appointment for their delayed care or were planning to schedule 1 soon.
Sustained Delay of Routine Physical and Mental Health Care Among COVID-19 Community Recovery Survey Participants Who Reported Delaying Care, N = 759.

Authors’ analysis of sustained or continued delay of routine physical and mental healthcare among COVID-19 Community Recovery Survey participants more than 18 months after the start of the pandemic (March 2020). Each sustained delay of health care type has a different N, since it corresponds to the number of participants who reported missing care earlier in the survey.
Denotes that data should be interpreted with caution. Estimate is unstable because the standard error represents more than 30% of the estimate.
Reasons for Delayed Care and Continued Delayed Care, by Care Type Among COVID-19 Community Recovery Survey Participants.

Authors’ analysis of the selected reasons for delayed routine physical and mental healthcare among COVID-19 Community Recovery Survey participants. Variations between reasons for delayed routine physical and mental healthcare were due to slight variations to questionnaire items.
Denotes recurrent responses that were written in by participants and not an original questionnaire item.
Denotes that data should be interpreted with caution. Estimate is unstable because the standard error represents more than 30% of the estimate.
Reporting standards not met. The standard error represents more than 50% of the estimate. Sustained delay of healthcare reasons data was collected through open-ended questionnaire items, coded, and aggregated by the most commonly reported.
Delayed or Avoided Mental Healthcare
Eighteen percent of survey participants had reported avoiding or delaying mental healthcare since the COVID-19 pandemic began, which represents about 176 812 people (Table 2). This prevalence was similar across all 3 BNH areas. Among those who delayed needed mental healthcare, the most common reason was concern about getting COVID-19 (38%), similar to those who delayed or avoided routine care (Table 4). Many survey participants reported delaying needed mental healthcare because of reduced hours or office closures (36%). Approximately 12% avoided or delayed mental healthcare due to transportation issues, 9% of participants reported that they were offered a telehealth visit, but that did not work for them, and 26% reported other reasons. Around 7% and 6% of participants provided write-in responses about cost-related challenges and challenges finding a provider, respectively, as reasons for delayed care. However, these were responses written in by participants and not included as answer choices and may therefore be underestimated.
Sustained Delays in Mental Healthcare
We found that 52% of those who delayed needed mental healthcare still had not received care by October 2021 (Table 3). Lack of health insurance coverage (20%) or the availability of providers (21%) were the primary reasons for sustained delayed mental healthcare throughout the pandemic (Table 4). Several participants also experienced challenges in getting an appointment (12%). Others stated that they did not seek mental health services because they planned to resolve their mental health issues without a provider (9%). Financial barriers, such as the high cost of co-pays, were also reported (7%). Only 2% of those who continued to delay mental healthcare cited concern about getting COVID-19 as a reason for the delay, unlike those who delayed routine healthcare.
Discussion
During March 2020 through October 2021, access to and utilization of non-COVID related health care had been greatly impacted among BNH residents. These findings are consistent with those of other studies conducted during the pandemic. A representative survey found that 41% of US adults missed medical care between the months of March and July 2020. 11 The same study revealed that about 29% of US adults missed either an annual check-up or preventative healthcare visit, such as screenings, vaccinations, etc., which is not unusual given that people across the country were responding to their states’ stay-at-home orders. With the exception of emergency care, many direct healthcare services were curtailed during the earlier stages of the pandemic. 11 However, our study results revealed a high prevalence of delayed routine healthcare among residents living in the BNH areas more than 18 months into the COVID-19 pandemic.
Delaying routine or preventative care can have important health consequences, for example, affecting BNH residents’ ability to properly manage their chronic conditions and leaving fewer opportunities for early detection of disease. 23
Additionally, the prevalence of avoided or delayed mental healthcare among BNH residents was higher when compared to city-wide estimates in August 2021. 8 This reflects the lack of resources and additional barriers that BNH residents disproportionately encounter, which prevents the engagement or re-engagement to clinical and mental health care. The mental health consequences of the pandemic and social distancing has been associated with the increased prevalence of anxiety and depression symptomology among NYC adults. 24 Additionally, rates of opioid-related overdose deaths in 2020 were at their highest historical level, which demonstrates the heightened level of need for adequate mental healthcare. 25
The most frequently reported types of delayed care (eg, annual check-up, dental care, and cancer screenings) illuminate an important emerging barrier of care. Many health services that traditionally relied on in-person direct interaction with clinical staff were frequently missed or delayed. Individuals were advised not to seek medical care except in emergency circumstances, for fear that healthcare services could rapidly be overwhelmed. This caused cancellations and delay of primary care visits and elective surgeries, and the reduction and/or redirection of the clinic staff who usually provided these services.2,26 Between April and May 2020, only about 14% to 20% of surveyed primary care providers in NYC reported keeping their small practices open for regularly scheduled services. 27 Findings such as these bear out those from our study that revealed that cancellations and the lack of available appointments after March 2020 impacted many BNH residents who sought out routine care.
Prolonged delay of care can result in long-term effects of the COVID-19 pandemic on individual and population health inequities. One study revealed that there have been substantial reductions in diagnoses of cardiovascular risk factors, chronic diseases and conditions, and certain tumors in 2020 compared with rates between 2017 and 2019. 28 While delayed diagnoses impact all NYC residents, it may be especially detrimental for those living in the BNH neighborhoods, since prior to the pandemic they have experienced a higher burden of chronic disease and other poor health outcomes, like obesity, diabetes, hypertension, and premature death rates for cancer. 16
The primary reasons for continued delayed care were related to concerns about COVID-19, challenges finding appointments, and challenges navigating insurance or not being covered by insurance. These findings highlight several important needs and lessons learned for recovery and response. As clinical and healthcare providers relied on various safety protocols to offer in-person visits, residents were still concerned about getting COVID-19. Persistently high case rates in BNH neighborhoods through October 2021 can explain this concern; with many of our BNH neighborhoods continuing to demonstrate higher than city-wide case rates through each wave (a surge of new COVID cases followed by declines). Findings from September 2020 revealed that more than 1 in 3 US adults reported delaying healthcare due to concerns about COVID-19 exposure or due to limited health services during the pandemic. 29 The sustained delay of routine care among BNH residents suggests that stronger methods of communication or outreach to each providers’ respective patient population was needed to re-engage people to care. There was also a need to reestablish patient confidence in the safety measures that were put in place to protect people from COVID-19 exposure and infection.
The lack of availability of appointments highlights the need for additional clinical and mental health services in BNH neighborhoods. Additionally, insurance-related challenges faced by BNH residents may be indicative of loss of employment or wages, high co-pays, and challenges finding in-plan providers for those who have insurance. Many people lost their employee-based health insurance coverage due to COVID-related unemployment or furloughs. 30 This led to a substantial increase in New York State Medicaid enrollment. 31 However, dealing with the complexity of navigating a new insurance plan along with searching for an in-network healthcare provider may have presented additional challenges to the re-engagement of care. These findings highlight the need for strong economic support and employment opportunities for residents in BNH neighborhoods as well as the need for health insurance navigation resources.
Furthermore, while BNH residents were offered virtual healthcare appointments, some noted that telehealth was not a viable option and contributed to the delay of care. While opportunities for telehealth services should have expanded healthcare access, 1 study revealed that Black NYC residents were less likely to use telehealth services when compared with other racial groups. 32 Other disparities in telehealth usage were found across different NYC neighborhoods, age groups, and socioeconomic status.32,33 This could be due to insufficient access to technology, incongruency with language between providers and patients, or a perceived decrease in the quality of care through telemedicine. Video visits require consistent and reliable access to both the internet and devices. An assessment of internet access found significant inequities across NYC with 16% to 33% of households across BNH neighborhoods lacking any internet access in 2018. 34 And while telehealth can be done at home using a phone-only visit, barriers to maintaining the same level of patient to provider privacy exist as well. These findings highlight the need for more equitable access to the internet, including broadband, devices for video visits, and phone services in under-resourced communities like the BNH neighborhoods.
Strengths and Limitations
This study had some limitations. While time periods were included in relevant questions to assist individuals in recalling sequences of events, responses might have been susceptible to recall bias. Also, social desirability bias could have been present, particularly with respect to those who spoke directly to an interviewer over the telephone. 35 Recruitment into the NYC Health Panel involved a hybrid approach with mailed physical letters, emails, and mobile-based text message to try to reach people in different ways and minimize recruitment bias. Although study participants were recruited from a probability-based sample, there may have been differences between the BNH area population and BNH residents who chose to be part of the NYC Health Panel, as well as the panel members who responded to this specific survey cycle. However, weighting was used to try to account for some of these differences. Additionally, this survey may not reflect the impacts of COVID-19 in different settings. For example, less than 1% of the panel participants reside within congregate settings (eg, nursing homes and dormitories), therefore this study may not reflect experiences of people in these settings, which were reported to be more severely impacted by COVID-19 than others. 36 Finally, due to small sample sizes this study has limited power to test for differences by age, gender, race, or other sub-groups for some variables.
Conclusions
Residents in historically disinvested neighborhoods, including the BNH catchment areas, experienced a great amount of disruption to their regular healthcare due to the COVID-19 pandemic. The vestiges of structural racism within the NYC neighborhoods like North and Central Brooklyn, the South Bronx, or East and Central Harlem were exposed by the high number of COVID-19 cases, deaths, and hospitalizations. Delayed healthcare may result in additional unintended consequences of the pandemic as new conditions may have been undiagnosed and the management of pre-existing conditions may have been disrupted, all further exacerbating the inequities in chronic health outcomes, and other health issues, that pre-date the pandemic. Diminished healthcare access has also been reflected among many urban cities and zip codes with a high Black and Latinx population.37,38
To increase healthcare access for these communities during COVID-19 recovery, it is essential to implement an equity-based approach that addresses the socio-economic barriers to healthcare. This study highlights opportunities for local health departments and healthcare institutions to reduce barriers to care by ensuring that facilities are adhering to federal and state safety guidelines. This can be achieved through the allocation of staff dedicated to patient safety and quality improvement. 39 A comprehensive assessment on the accessibility of telemedicine for both clinical and mental healthcare should be conducted to identify barriers and strategies for adoption by patients. Community-based education efforts, in partnership with local health providers, can reach out directly to residents to provide services which can facilitate a reintroduction to care, such as, health screenings, patient and insurance navigation services, distribution of PPE and information on COVID-19 safety, strategies that were implemented by the BNHs throughout the pandemic.
Footnotes
Acknowledgements
The authors thank Stephanie Arbelaez, Shelby Boyle, Brandon Brooks, Jae Eun Chang, Jaime Gutierrez, Lissette Paulino, Richard Sierra, Barbara Wong, and, as well as Sarah Dumas, Sharon Perlman, Leigh Reardon and rest of the NYC Health Panel team for their help with this study. The authors also want to thank Shadi Chamany, Nneka Lundy De La Cruz, Rachel Schwartz, Amber Levanon Seligson, and Beth Seltzer and for their input during the preparation of this paper. Finally, the authors acknowledge Michelle Morse, Zahirah McNatt, Padmore John, Anita Reyes for their support and leadership of the Bureaus of Neighborhood Health, Center for Health Equity and Community Wellness at the New York City Department of Health and Mental Hygiene.
Author Contributions
SD, CN, JP, RD, and LS planned and implemented the study. SD, CN, and FD performed the data analysis. The first draft of the manuscript was written by SD, CN, and JV and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a contract from the Centers for Disease Control and Prevention [Contract No. ELC CARE 6 NU50CK000517-01-09]. The funder had no role in the study and was not involved in the planning or implementation of the study, nor the analysis and interpretation of the data.