
Abstract
Introduction:
The COVID-19 pandemic has had profound impacts on people with diabetes, a group with high morbidity and mortality. Factors like race, age, income, Veteran-status, and limited or interrupted resources early in the COVID-19 pandemic compounded risks for negative health outcomes. Our objective was to characterize the experiences and needs of under-resourced Veterans with type 2 diabetes during the COVID-19 pandemic.
Methods:
We conducted semi-structured qualitative interviews (March through September 2021) with U.S. military Veterans with diabetes. Transcripts were analyzed using a team-based, iterative process of summarizing and coding to identify key themes. Participants included Veterans (n = 25) who were mostly men (84%), Black or African American (76%), older (mean age = 62.6), and low-income (<$20 000/year; 56%). Most participants self-reported moderate (36%) or severe (56%) diabetes-related distress.
Results:
Shutdowns and social distancing negatively impacted Veterans’ social, mental, and physical health. Veterans reported feeling increased isolation, depression, stress, and unmet mental health needs. Their physical health was also negatively affected. Despite pandemic-related challenges, Veterans adapted with new technological skills, appreciating their families, staying active, and relying on their religious faith.
Conclusions:
Veterans’ experiences during the pandemic revealed the importance of social support and access to technology. For those without social support, peer support could protect against negative health outcomes. Emergency-preparedness efforts for vulnerable patients with type 2 diabetes should include raising awareness about and increasing access to technological resources (eg, Zoom or telehealth platforms). Findings from this study will help tailor support programs for specific populations’ needs in future health crises.
Introduction
The COVID-19 pandemic has had profound societal impacts with stay-at-home orders, business closures, fears of infection, and shifts from in-person to online resources increasing social isolation.1,2 Likewise, disruptions to medical services have decreased access and healthcare utilization. 3 Such changes resulted in physical, social, and mental health repercussions.
Some populations were disproportionately affected by the pandemic because of their demographic characteristics or health-related factors. Underserved Veterans like African American and Hispanic, older, or low-income individuals had significantly higher rates of hospitalization, morbidity, and mortality from COVID-19.4 -6 With these groups already experiencing poorer access to healthcare, this unequal impact exacerbated health disparities. 7 Moreover, individuals with chronic medical conditions—including type 2 diabetes—had increased fears of and greater risk for COVID-19 infection, morbidity, and mortality.8 -10
Veterans, especially those with type 2 diabetes, who were African American, older, or low-income, were particularly susceptible to the pandemic’s effects. 11 Compared to the general population, Veterans were twice as likely to test positive for COVID-19. 12 Veterans also have poorer overall health and health behaviors, including higher rates of smoking, diabetes, cardiovascular disease, and mental health conditions. 13 These pre-existing conditions placed Veterans at greater risk for mental and physical health complications during the pandemic.
The pandemic also negatively affected social health or social support in these populations. Social support is the instrumental, informational, or emotional assistance individuals receive that helps promote healthy behaviors, resulting in improved overall wellness.14,15 For those with diabetes, social support can improve adherence to and motivation for diabetes self-management. 16 Social ties and feelings of belongingness can also increase an individual’s sense of self-esteem, self-worth, and confidence—all of which improve mental health.14,15 Because of its protective effects on physical and mental health, social support is especially important during adverse events. According to the stress-buffering theory, for example, social support provides both tangible and psychological resources that decrease the negative effects of stress. 17
Other studies have addressed access to health care during the pandemic from largely quantitative approaches. 3 In the current study, we sought to learn more about Veterans’ unmet needs and coping strategies during the COVID-19 pandemic in their own voices through qualitative interviews. These interviews build on existing research by providing more contextually rich insight into the experiences of those who were particularly vulnerable to the pandemic’s impact. Specifically, we take a phenomenological approach to explore the pandemic’s effects on the social support, mental health, and physical health of African American and Hispanic, older, and low-income Veterans with type 2 diabetes. Characterizing Veterans’ needs and coping strategies provides real-world insight into how best to support Veterans at-risk for health inequities during future public health crises.
Methods
Participants were recruited through the VeteraN SuPport and REsources for Diabetes (iNSPiRED; NCT04041375) study, a U.S. Veterans Health Administration-sponsored clinical trial targeting diabetes-related distress in Veterans with type 2 diabetes. Diabetes-related distress is the psychological distress resulting from having or managing diabetes. 18 Veterans enrolled in iNSPiRED received a 3-month peer-led resource navigation and coaching intervention or usual care. Eligibility criteria included self-reported type 2 diabetes, access to a telephone, and at least moderate diabetes-related distress based on the 2-item Diabetes Distress Scale. 18 A subsample of iNSPiRED participants was recruited for semi-structured telephone interviews focusing on Veterans who were members of a community disproportionately affected by COVID-19 (ie, age >60, annual income <$20 000, or a racial or ethnic minority). We purposively sampled women Veterans. All study activities were reviewed and approved by the Baylor College of Medicine Institutional Review Board (H-48449) and the Michael E. DeBakey Veterans Affairs Medical Center Research and Development Committee. Interviews were conducted from March to September 2021.
Data Collection
The research team developed a semi-structured qualitative interview guide with input from a Community Advisory Board of Veterans, healthcare providers, and community-based organization representatives that serve older adults and individuals with diabetes. Questions focused on how the pandemic impacted ability to meet basic, medical, and mental health needs; experiences with social distancing; challenges accessing services; resources and sources of support; and unmet needs. Interviews lasted 60 min on average. Participants received $50 for their time. Interviews were audio-recorded and transcribed verbatim.
Prior to their interviews, participants took the Pain Management Collaboratory’s (PMC) Coronavirus Pandemic Measure survey. 19 We use the PMC and demographic data from the parent study to describe the sample (see Tables 1 and 2). We include diabetes-related distress measured by the 17-item Diabetes Distress Scale, depression measured by the Patient Health Questionnaire-8, and anxiety measured by the Generalized Anxiety Disorder-7 scale.20-23
Participant Characteristics (n = 25).

Based on Diabetes Distress Scale-17 score.
Generalized Anxiety Disorder-7 scale cutoff score of 10.
Patient Health Questionnaire-8 cutoff score of 10.
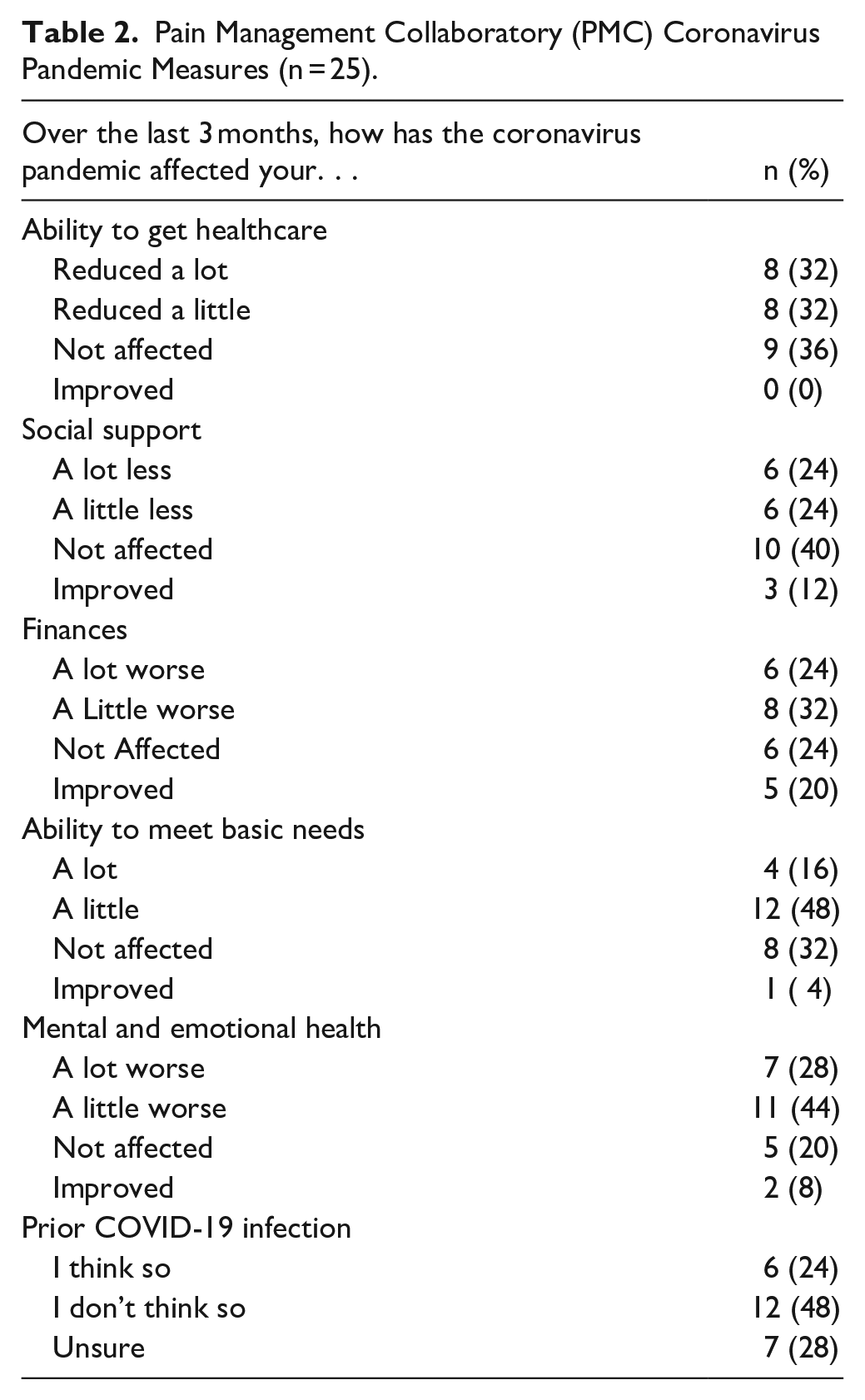
Pain Management Collaboratory (PMC) Coronavirus Pandemic Measures (n = 25).
Data Analysis
Qualitative data analysis followed a team-based, iterative process. 24 Using 5 interview transcripts, coders identified an understanding of the general experiences of participants to develop the codebook. Using PowerPoint, we created a quotation inventory and an interview profile for each participant. Quotations from the total sample of interviews were then sorted into common topics, resulting in the identification of themes described below.
Results
Twenty-five Veterans completed the telephone interview. We summarize participant characteristics in Table 1. Participants included Veterans (n = 25) who were mostly men (84%), Black or African American (76%), older (mean age in years = 62.6), and low-income (<$20 000/year; 56%). Nearly all participants had moderate (36%) or severe (56%) diabetes-related distress. Many also had clinically significant anxiety (36%) and depression (44%) symptoms. Most (84%) participants reported receiving at least one COVID-19 vaccination. On the PMC survey, participants reported reduced access to healthcare, decreased social support, worsened finances, decreased ability to meet basic needs, and worsened mental and emotional health during the pandemic (see Table 2). A quarter (24%) thought they had been sick with COVID-19 at some time during the pandemic, and a third (28%) were unsure.
Disconnected: Pandemic Shutdowns, Distancing, and Precautions
Veterans shared how social health was the keystone of their pandemic-related mental and physical health. Social isolation was particularly common among Veterans—especially those living alone—who relied on their families for social support. Susan’s (62, Black) comment nicely illustrates how she became increasingly sad and disconnected from her family without the option for in-person visits early in the pandemic:
I don’t mind being here by myself. I’m used to it. But when you can’t get out and be around your family, that gets a little depressing sometimes. I couldn’t be around my grandkids, and I just had to get used to just being here [alone], and I’ve never been actually by myself like this before in the past because someone was always around or coming over. But then when the pandemic came, everything stopped.
Unable to see her 9 grandchildren in person, Susan became increasingly sad and disconnected from her family.
Veterans with other family members in the home also saw the consequences of pandemic shutdowns. William (54, Black) acknowledged the stress social distancing had on him but was more worried about the effects of isolation on his children. Compared to their pre-pandemic social lives when they would have frequent visitors, William recounted having only 3 in the past year. “It was really tough for the kids,” who complained about not being able to see other family members or neighbors. The result was “stressful” and “emotional.” Tired of being stuck in the house, their big yard and walks were not enough to relieve the stress for William or his family. William acknowledged the “mental toll” of not knowing when the pandemic would end and when life might go back to normal.
Senior center and church closures greatly impacted Veterans’ social lives, too. Mary (67, Black) expressed how the pandemic had a “great effect” on her social life as her senior center shut down. She was cut off from her “little bit of socializing” (eg, field trips and meals) during March closures—“they shut it down—totally and completely.” Veterans also missed attending church services. Michael (67, Black) stopped going to in-person services to help slow the spread of COVID-19. As a church deacon, he mourned his inability to “be at my post.” Altogether, Veterans were denied opportunities to connect.
Isolated from family and social functions, many felt lonely and helpless but cautious to ask for aid. Recognizing the precariousness of the pandemic, local family members and neighbors either stepped up to help Veterans or kept their distance. Admitting he may not reach out as much as he needs to, Thomas (76, Black) depended on his son “‘cuz he’s the only one I can reach. And he’s the only somebody I know that would drop his hat and get here.” Understanding the need for social and physical distancing, however, Veterans’ family members stayed away until vaccinations were more widely available and trusted. Donald’s (71, white) adult grandson, for example, was not allowed to visit until he was vaccinated. Christopher (49, other) was also worried about his mother. Despite being “hard not to see her for a long time,” he “stayed away just to make that sure she is well” due to her age.
Veterans’ Mental and Physical Health
Veteran perceived that the COVID-19 pandemic also greatly affected their mental health and, at times, exacerbated their physical health problems. Veterans reported feelings of sadness, depression, or heightened stress due to social distancing and isolation. Brian (54, Black) observed he would “get more depressed with the pandemic going on than from having diabetes.” In describing herself as the kind of person who does not break easily, the pandemic cast a “shadow” over Mary. She became depressed and increasingly confused at home alone.
Given their diabetes and diabetes-related distress, Veterans were acutely aware of the effects of the pandemic on their bodies. Alongside Jeffrey’s (59, Black) inability to see his daughter—a nurse who worked in a COVID-19 ward—news of COVID-19 deaths led him to reflect on his own diabetes and vulnerability to the virus wherein he became very emotional and admitted feeling hopeless. Pre-pandemic, Jeffrey was able to “stabilize” his mental health, but as the pandemic distanced him from his daughter, he lapsed in checking his blood sugar, too. Given their diabetes diagnoses, many Veterans mentioned the ups and downs of their diabetes management during the pandemic. Embarrassed to admit it, Joseph (63, white) also noticed the effects of pandemic stress on his sexual health having had trouble becoming aroused. He said sitting around during the pandemic was “not good for his physical or mental health.” Joseph sought help for his condition but the medication his doctor prescribed was not effective.
Veterans, however, were not without resources to combat their mental health issues. Even as the pandemic disrupted mental health services and appointments were deferred, Veterans sought help for their mental health from online, social, and professional resources. David (53, American Indian/Alaska Native), for example, used a mental health phone app as support. William shared mental health assistance information with his Veteran peers—“a lot of us we talk, and we learn what we can do.” Timothy (54, Black), however, was frustrated being put on hold while attempting to reach his VA psychiatrist. When the VA shut down because of COVID-19, he felt he had to “just deal with” his mental health. He elaborated how:
Most of the time you call them when it’s too late [to reach out for help]. . . . You[‘re] depressed, you’ve already screamed at your family. . . . There are times that I raise my voice more than I should because I’m supposed to be on some medication for my mental health.
Timothy further admitted it is not easy for members of traditionally under-resourced communities to seek help “because Blacks and other minority people think that seeing a psychiatrist is stupid,” how “they don’t see the benefit,” and they would “rather pay a bill than go see a psychiatrist.” Even without the stress of the pandemic, Jeffrey admits that talking about one’s mental health is a “hard subject” despite regularly scheduled video appointments with his psychologist. These Veterans’ experiences illustrate the multiple effects of the pandemic on their social, mental, and physical well-being.
Veterans’ Adaptation, Appreciation, Coping, Reliance, and Resilience
Despite the hardships of the pandemic and their health conditions, underserved Veterans found ways to improve their situations. They adapted by virtually connecting with friends and family, appreciated their partners, coped with boredom by staying active, relied on their religious beliefs, and were resilient by reframing their outlooks on pandemic life given their military experiences.
Adaptation
Without in-person connections, Veterans turned to phone calls and video conferencing (eg, Zoom) to keep up their spirits and stay connected with family and friends—though they sometimes needed help setting up the new technology. Larry (73, Black) especially appreciated the opportunity to interact with his grandchildren on Zoom, and Susan found “the Zoom thing” helpful to curb her sadness. Using video conferencing provided opportunities for Veterans to attend events like church services and birthday parties. Jennifer (43, other) recalls how much she enjoyed Zoom calls:
I have a lot of friends and family that don’t really live here. We all learned how to do Zoom meetings and get-togethers through the Internet. Even my grandma! We[‘ll] keep doing the video calls [after the pandemic]. We did girls’ night out as well with my friends from everywhere—well, “girls’ night in,” that’s what we call it.
Without the ability to see friends and family in person, Veterans turned to frequent phone calls or learned how to connect through Zoom calls when otherwise isolated.
Appreciating partners
For some, the pandemic was an opportunity to spend time with their partners. As Richard (68, other) commented, “it’s just me and my wife and that’s the way we want it.” John (68, Black) similarly reflected how the opportunity to spend time with his wife of 47 years was “splendid,” they “enjoy each other’s company.” Likewise, David liked that his wife was working from home now and noted that “her company was real good.” With the Veterans’ health conditions, spouses helped encourage good habits, too. Michael appreciated how he and his wife (who also has diabetes) “work together” by taking their medicine at the same time which “kind of motivate[s] me to take care of her, so I take care of myself.” For some Veterans, the pandemic was a chance to appreciate the company of loved ones who, in turn, became key sources of support.
Coping with boredom
Getting out of the house was an important way to stay mentally healthy—or at least a way to curb boredom. Given stay-at-home orders, and to avoid risk of exposure to COVID-19, some Veterans took solitary approaches to cope with their boredom by reading, writing, or woodworking. Others ran errands, and, when available, attended in-person church services or frequented local senior centers—despite the health risks. Getting out of the house in these various ways was important to the health of Veterans.
In need of reasons to get out of the house, participants went on trips to the grocery store, ran errands, or went on walks in their neighborhoods. To avoid going “stir crazy,” David would join his wife on her outings. Similarly, Richard, an avid motorcyclist, would hop on his bike with his wife to go to stores, commenting, “We’re old, but we still ride!” Beyond spur-of-the-moment outings, others would plan—though the precautions they took were often unclear. On alternating Sundays, Kenneth (71, Black) would “sit around and gossip” with his sisters. Mary frequently drove others to the grocery store or doctor’s appointments because to her it was important to do “something for somebody. That made [the pandemic] better for me to be able to help some other people” and encourage those who were “downer.” Opportunities to get out were something to look forward to. (When going to stores, most Veterans noted they would wear masks though it was often unclear if they wore them around family members.)
Relying on religion
Religion and church services were prominent outlets for participants that helped assuage worries and health concerns during the pandemic. Some Veterans attended services online or via TV, though Christopher described his difficulty focusing when not in-person and how little he gets out of online services. Without in-person services and in lieu of some health services, Veterans relied on their independent beliefs. Joseph elaborated on how he evaded suicidal thoughts during the pandemic because “God put a specific thing on that. If you kill yourself, you will not come up there and see [God].” Like Joseph, Robert (74, Black) took his faith seriously and turned to his beliefs to aid his mental health during the pandemic:
I am a Christian. And I truly believe in Jesus Christ. . . . I believe that Jesus would help me, which he did. He helped me in prayers and together with the family prayers, we all kept that mental deal that God is in control. No matter what goes on, he’s still in control.
Similarly, Ronald (75, Black), turned to prayer when stressed or anxious saying, “When I get a little upset, I howl to Jesus, and then I feel better.” Their religious beliefs thus helped participants assuage some mental health concerns and pandemic stressors.
Resilience through reframing
Veterans proved their resilience by reframing their thinking. For example, Richard provided the advice that:
You can help yourself. All you have to do is think of positive things. If the world is falling apart, look at the good side. There’s something good there. And I know there are some other people that are very troubled, and they need help, but . . . I’ve always thought things through. And I survived.
Veterans’ resilient attitude comes from their time in the military because, as Christopher described during his time in the Army, “they tell us, ‘hey, suck it up and drive on.’” Likewise, Ronald often reminds himself that “tomorrow is another day. Keep going.” Other participants found similar ways to reframe the stress of the pandemic.
Discussion and Conclusion
Findings from this study suggest the importance of maintaining support for social, mental, and physical health during the COVID-19 pandemic among low-income, older, or racial minority Veterans with type 2 diabetes and high diabetes-related distress. Veterans’ diabetes was not a leading factor to their pandemic stressors, but it was a contributor. Sudden closures because of the COVID-19 pandemic caused much disruption of Veterans’ social lives resulting in declining mental and physical health. Despite these conditions, Veterans adapted to new ways of communicating, appreciated those close to them, coped with isolation by staying busy, relied on their faith, and were ultimately resilient. Yet, questions remain: What can we learn from underserved Veterans’ experiences during the COVID-19 pandemic? And, what unmet needs should be addressed in the future?
Our findings are in line with prior research that has found Veterans are a psychologically resilient population. 25 Indeed, we find that when faced with barriers to socializing, Veterans found ways to adapt. We add to extant literature showing how Veterans maintained social interactions through letter writing or using virtual platforms to connect with friends and family and coped by taking up new hobbies, spending more time outdoors, or using the increased alone time for self-reflection.1,25 -28 Veterans in the current study expressed a willingness to learn about new technology, especially if it helped them connect with friends and family.
Based on our findings, we provide the following suggestions to improve the experiences and health of Veterans and other vulnerable patients now, as the COVID-19 pandemic is ongoing, and during future public health crises, natural disasters, or other instances of delayed care.
First, there is a clear need to leverage peer support networks to mobilize and provide frequent check-ins as opportunities for Veterans to feel connected, heard. Actively using Veteran Service Organizations, for example, could ameliorate health issues early by connecting Veterans to providers and resources. This echoes recent calls to leverage the power of community health workers during a pandemic or other disaster, rather than sideline these important allied health partners. 29
Second, our findings reinforce the central role of access to technology to keep vulnerable patients connected to family, friends, and healthcare and community resources. Healthcare organizations and government agencies need to explore ways to improve patients’ access to technology and promote alternative pathways for communication within informal social support networks. Zoom or similar platforms and social media can connect vulnerable populations living in isolation due to rurality, lack (or cost) of transportation, or physical and mental ailments. Indeed, providers should use telehealth to improve access and connection to underserved patients. Relatedly, designing mental health phone apps or other virtual resources can fill gaps in care and provide support. Moreover, increasing Veterans’ awareness of the VA’s digital divide consult program can reduce barriers for Veterans needing telehealth. 30 Disparities in home broadband access and device ownership (smartphones, tablets, and computers) persist for those with annual household incomes less than $30 000 compared to those with higher incomes despite an increase across income groups. 31
Third, helping Veterans and other vulnerable patients have access to, and become more comfortable using, smartphones or other technologies is essential. Researching best practices for helping vulnerable groups learn how to use technology is imperative to ensuring equitable distribution of the benefits of digital resources. According to a U.S. Department of Education (2018) report, approximately 16% of U.S. adults are not digitally literate particularly those who are older, less educated, African American, Hispanic, or foreign-born. 32 Assistive technology could enable older adults and those with disabilities to engage with digital technology. 33 To this end, some communities may require targeted support. Given racial and cultural differences in mental health service use, mental health counseling may help improve perceptions about psychological services.
Strengths and Limitations
As with any study, we identify several limitations. Our sample was one of convenience and a product of purposeful sampling from those who completed the parent study. We are thus unable to generalize beyond the current sample to a larger Veteran population. Generalizability is rarely the goal of qualitative research, yet our findings add to a larger body of literature by providing the perceptions of Veterans themselves in their own words. We obtained a diverse sample of Veterans including many who are members of more than one group vulnerable to the effects of the pandemic.4 -6
Conclusion
Our analyses of Veterans’ experiences during the pandemic revealed the importance of social support and access to technology. For those without social support, peer support could protect against negative health outcomes. Emergency-preparedness efforts for vulnerable patients should include raising awareness about and increasing access to technological resources (eg, Zoom or telehealth platforms). Findings from this study will help tailor support programs for specific populations’ needs.
Footnotes
Acknowledgements
Special thanks to Marie Diaz for her contributions to the data analysis.
Prior Presentation
N/A
Disclaimer
This material is the result of work supported with resources and the use of facilities at the Michael E. DeBakey VA Medical Center. The views expressed in this article do not represent the views of the U.S. Department of Veterans Affairs or the United States government. Institutional Clearance: N/A
Individual Author Contribution Statement
TE collected the data. TMH, TE, NK, and GT analyzed the data. TMH and JT drafted the original manuscript. MK, TE, and GT designed this research, reviewed, and edited the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was provided by South Central Mental Illness Research, Education, and Clinical Center (MIRECC).
Clinical Trial Registration
N/A
Institutional Review Board (Human Subjects)
This study was approved by the Baylor College of Medicine Institutional Review Board (H-48449) and the Michael E. DeBakey Veterans Affairs Medical Center Research and Development Committee.
Institutional Animal Care and Use Committee (IACUC)
N/A
Data Availability Statement
N/A