
Abstract
Objectives:
Medical facilities have been required to effectively utilize insufficient human resources in many countries. Therefore, we qualitatively and quantitively compared physicians’ working burden, and assessed advantages and disadvantages of the single- and the multiple-attending physicians systems in inpatient care.
Methods:
In this cross-sectional study, we extracted electronic health record of patients from a hospital in Japan from April 2017 to October 2018 to compare anonymous statistical data between the single-attending and multiple-attending-physicians system. Then, we conducted a questionnaire survey for all physicians of single and multiple-attending systems, asking about their physical and psychiatric workload, and their reasons and comments on their working styles.
Results:
The average length of hospital stay was significantly shorter in the multiple-attending system than in the single-attending system, while patients’ age, gender, and diagnoses were similar. From the questionnaire survey, no significant difference was found in all categories although physical burden in multiple-attending system tended to be lower than that in single-attending system. Advantages of multiple-attending system extracted from qualitative analysis are (1) improvement of physicians’ quality of life (QOL), (2) lifelong-learning effect, and (3) improving the quality of medical care, while disadvantages were (1) risk of miscommunications, (2) conflicting treatment policies among physicians, and (3) patients’ concern.
Conclusions:
The multiple-attending physician system in the inpatient setting can reduce the average length of stay for patients and also reduce the physical burden on physicians without compromising their clinical performance.
Keywords
Introduction
Attending physicians are responsible for the overall care of patients in both inpatient and outpatient settings. Under the multiple-attending-physicians system, 1 patient is assigned to a team of physicians who are authorized to make patient-care decisions. In contrast, inpatient medical care in Japan has historically been provided under a single-attending-physician system wherein 1 representative physician works with patients as the sole attending physician. Under this system, a single physician often bears responsibility for the management of a patient’s condition even if another on-duty physician was working within the medical facility during holidays or after hours. A multiple-attending-physicians system is a system in which multiple attending physicians are responsible for a single patient, and although the attending physician changes on a daily basis, they share responsibility for the patient and participate in decision making as a team.
Since the physician population is aging especially in rural areas, 1 medical institutions need to secure adequate human resources. Although the employment of primary care physicians has been identified as a potential solution to this issue, 2 those in rural areas have a high burnout rate and proactive measures to mitigate this risk are important.3-5 As a demand for reform in physicians’ working style across Japan, the Panel on the Reform of Physicians’ Work Style under the Ministry of Health, Labour, and Welfare proposed some measures to reduce the length of hours that physicians can work at medical facilities. For example, (1) not being obligated to provide advice to non-emergency patients on holidays or during after-hours, (2) reducing their post-night-shift duties, (3) having mandatory holidays, and (4) introducing a multiple-attending-physicians system. 6
The advantages and disadvantages of single and multiple attending-physician systems have not been investigated sufficiently. According to a cross-sectional questionnaire survey in Japan, departments with multiple attending physicians had shorter overtime hours than those with single attending physicians, and there was no difference in job satisfaction. 7 In contrast, studies from German general practitioners in solo and group practices revealed a higher prevalence of emotional exertion, depersonalization, and little self-accomplishment among physicians in group practices compared to solo practices. 8
Therefore, the present study attempted to compare the clinical performance of physicians in inpatient care between the single and the multiple-attending-physicians systems, cross-sectionally. Furthermore, we also conducted a questionnaire survey on physicians who have worked under each attending-physicians system to qualitatively analyze their work burden and identify the advantages and disadvantages.
Methods
The present study was performed at the Hino Hospital, which was the only medical institution in the town of Hino (3278 individuals, 49.0% aged above 65 years in 2019), in the southwestern area of Tottori prefecture, Japan. As of 2017, the Hino Hospital had 99 beds in 2 wards with 10 full-time physicians (5 for Internal Medicine, 2 for Surgery, 1 each for Orthopedics, Ophthalmology, and Pediatrics) and 6 part-time general physicians in the Department of General Medicine working. A different general physician was in charge of the inpatient treatment for each day under the multiple-attending-physicians system rotating daily within the wards where internal medicine physicians engaged in their practice.
In this cross-sectional study, we defined single-attending physician as solo attending physician who was in charge of, decided and treated all clinical issues by oneself, including off-duty hours and weekends, whereas multiple-attending physician as 2 or more physicians shared their responsibilities and clinical workloads for patients. We obtained anonymous statistical data from electronic medical records from April 2017 to October 2018. We collected information regarding patients’ age, sex, length of hospital stay, living area, and status before admission.
Next, we performed a qualitative study to determine the physicians’ clinical competence and physical and psychiatric burden of work under the 2 systems and also compared the advantages and disadvantages of both systems. Physical burden refers to the sense of physical burden felt as a result of the attending physician’s work, while psychiatric burden refers to the stress and distress related to the responsibilities as an attending physician. We surveyed 11 physicians, including 6 general physicians and 5 internal medicine physicians. The participants were physicians working at Hino Hospital, the same physicians included in the quantitative survey. At the start of this study, written informed consent was obtained from all subjects, and allowed that they could withdraw their consent or ask questions at any time. Two group of physicians were completely separated and not duplicated. The questionnaire contained physicians’ identification (age, post-graduate year, sex, and the former experience of the multiple-attending-physicians system) and items about their current working conditions (Table 1) that were assessed using a visual analog scale (VAS). 9
The Questionnaire About Physicians’ Current Working Conditions.

They also provided reasons and comments for each item, and these texts were analyzed qualitatively by thematic analysis. 10 The generated themes were grouped into categories according to the similarity of content. Data analysis was performed collaboratively by 3 main authors (DP, DS, and TH) and triangulated with the other authors.
We employed a mixed methods approach in this study because we wanted to explore, through qualitative research, the background and reasons for the differences between the 2 systems of attending physicians that would be revealed by a quantitative study.
This study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Hino Hospital ethics committee (No. 2019-3).
Statistical Analysis
All data were expressed as mean and standard deviation, or median and range. For comparison between 2 groups, continuous variables were analyzed using the Student’s t-test and categorical variables were analyzed using the chi-square test. To calculate the effect size, Cohen’s d was calculated from the mean and standard deviation of 2 continuous variables. Using G*Power software, a sample size was calculated to detect differences in outcomes between the 2 systems of attending physicians. With an effect size of 0.5, alpha error of .05, and a power of 0.8, 128 inpatients were considered necessary. Also, the VAS was analyzed using the Wilcoxon rank-sum test. All analysis was performed using the STATA version 15 (STATA Corp. TX) and Microsoft Excel version 16.26 (Japan Microsoft Corp., Tokyo, Japan).
Results
The baseline data of working physicians and inpatients under the single- and the multiple-attending-physicians systems are shown in Table 2. There were no significant differences in physicians’ age, gender, and post-graduate-year between the 2 systems. The numbers of inpatients under the single-attending-physician system and the multiple-attending-physicians system were 592 and 263, respectively. There were no significant differences in patients’ age and gender, however, hospitalization days under the single-attending-physician system were significantly longer than those under the multiple-attending-physicians system. The effect size for the difference in hospitalization days was 0.24. Significant differences in living areas and status before admission were also observed between the 2 systems (P = .006 and .0014, respectively). Patients living in Kofu town (north of Hino), or nursing homes or geriatric facilities were significantly more under the multiple-attending-physicians system than under the single-attending-physician system.
Baseline Data of Physicians and Inpatients Under the Single-Attending-Physician System and the Multiple-Attending-Physicians System.

Data are presented as number (%) or mean ± SD (range). P values are based on Student’s t-test or chi-square test, as appropriate.
The frequency of inpatients’ diseases under the 2 systems is shown in Table 3. Pneumonia and heart failure were the most frequent under the 2 systems, and 8 out of the top 10 diseases were similar under the 2 systems. Therefore, no differences in the diseases of patients were observed between the 2 groups.
Ranking and the Frequency of Inpatients’ Diseases.
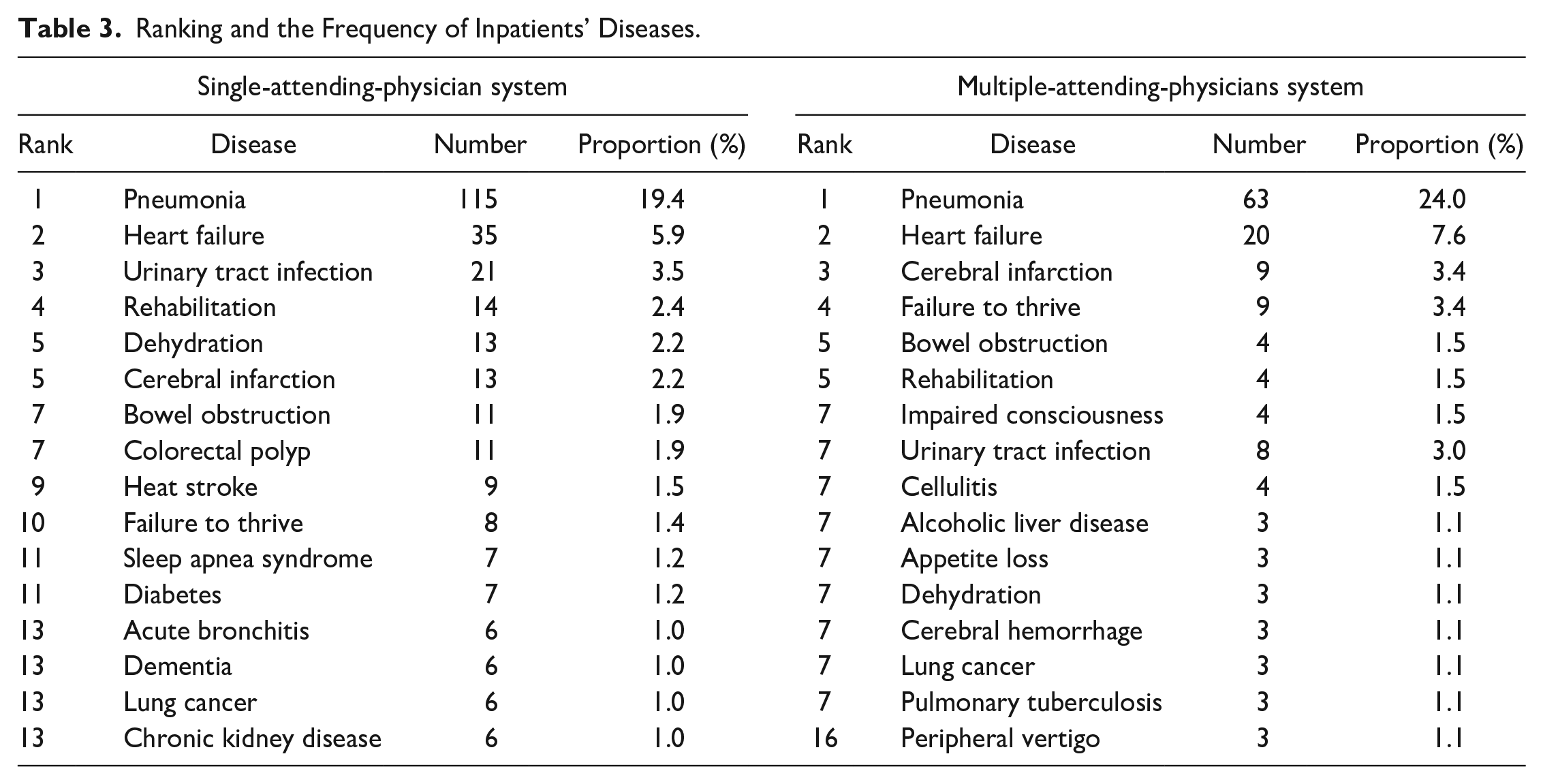
Figure 1 illustrates the degrees of physicians’ working conditions assessed by a visual analog scale. All the 11 physicians engaged under the single or multiple- attending-physicians system answered the questionnaire. The results of the questionnaire survey showed that there was no significant difference between the 2 groups in all categories. However, physicians under the multiple-attending-physicians system tended to have less off-duty working hours and less physical work burden, while the psychiatric work burden under the 2 systems seems almost equal.

Results related to current working situations assessed by VAS.
In Tables 4 and 5, we described the advantages and disadvantages of 2 systems extracted from the data of qualitative survey. The analysis of the free description of the 11 physicians from single and multiple-attending-physicians systems showed that the multiple-attending-physicians system had 3 advantages: (1) improvement of physicians’ quality of life (QOL), (2) lifelong-learning effect, and (3) improvement of the quality of medical care (Table 4). The 3 disadvantages which were identified included: (1) risk of miscommunications, (2) conflicting treatment policies among physicians, and (3) patients’ concern (Table 5).
Advantages of Ward Management Under the Multiple-Attending-Physicians System.

Disadvantages of Ward Management Under the Multiple-Attending-Physicians System.

Furthermore, the category “improvement of physicians’ QOL” included 2 themes: secured time and risk diversification, and the category “improving the quality of medical care” included 4 themes: team communication, skill compensation, standardization of medical care, and prevention of medical errors. There were conspicuous opinions that the multiple-attending-physicians system provides learning opportunities, especially for physicians who are not confident about their skills, provides time support, and contributes to improving the medical care level for patients.
Regarding the disadvantages of the multiple-attending-physicians system, the category “risk of miscommunications” included 4 themes: physician-patient relationship, communication among physicians, inter-professional work, and difficulty in patient understanding. The category “conflicting treatment policies among physicians” also included 3 themes: disagreement regarding the treatment plan, power relationship among physicians, and lack of leadership. The risk of miscommunications is a problem highlighted not only in the communication between physicians sharing patients’ information but also in communication with all related individuals such as patients and nurses. Some physicians complain about stress due to conflict regarding the treatment plan. In case there is a power gradient due to age or social position, the power relationship may interfere with appropriate clinical practice. The third category “patients’ concern”, especially patients’ unfamiliarity with the culture of the multiple-attending-physicians system, can be considered as a problem peculiar to Japan where the single-attending-physician system is recognized as natural by patients and co-medical staff like nurses. Some physicians worry about patients’ feelings for this unfamiliar style of clinical practice.
Discussion
So far, only a few studies have reported the effects of the multiple-attending-physicians system, and most of them have emphasized the diagnostic accuracy regarding the interpretation of skin lesions or X-ray films.11-15 In the present study, we obtained data on not only on the average length of hospital stay in the single and multiple-attending-physician systems, but also on the physical and psychiatric burden on physicians in Japan.
In the present study, the length of hospital stay was significantly lower in the multiple-attending-physicians group than the single-attending-physician group. The effect size was somewhat smaller at 0.24, but was sufficient to suggest a difference in the number of days of hospitalization by the 2 systems. In the multiple-attending-physicians system, the sharing and discussion of patient information within the attending team may have reduced unnecessary tests and treatments and even facilitated early discharge from the hospital, leading to the decrease in length of hospital stays.
There were no significant differences in patients’ age, sex, and disease variations between the 2 attending-physician groups. Although the number of inpatients differed between the 2 attending-physician groups, the workload per actual working physician was hardly comparable for the following reasons: (1) each physician in both groups had many tasks other than inpatient care, such as participation in outpatient and branch clinics, endoscopy/other procedures and clinical internship (100 students per year), (2) since the multiple-attending-physicians group started their inpatient care in April 2017, the number of admitted patients was initially small.
Based on the VAS analysis, there was no significant difference in the indicator of working conditions or burdens between the 2 groups. However, it is possible that the multiple-attending-physicians group may have fewer working hours and less physical workload but may experience some difficulty regarding understanding the patients’ disease status, physician-patient relationship, imbalances due to workload, and inter-professional relationships than the single-attending-physician group. Notably, the single-attending-physician system tended to be more physically stressful for the physicians. On the other hand, both the groups had similar scores on psychiatric burden. The multiple-attending-physician system may have less burden of overtime work than the single-attending-physician system, but there are more difficulties in understanding patients and cooperation among other professionals, which may have been offset and resulted in equal psychiatric burden.
Thus, the present study showed that the multiple-attending-physicians system has the advantages of (1) improving the physicians’ QOL, (2) lifelong learning effect, and (3) improving the quality of medical care. Its disadvantages include (1) the risk of miscommunications, (2) conflicting treatment policies among physicians, and (3) patients’ concern (unfamiliarity with the multiple-attending-physician system). While improving the physicians’ QOL is the most important benefit, the effects on enhancing life-long learning, which is generally related to physicians’ burnout, 16 suggests that the multiple-attending-physicians system may be a means to prevent physicians from dropping out in the long term. Furthermore, from the decision-making perspective, the involvement of multiple physicians can minimize sanctioning and reduce emotional distress among physicians. 17
On the other hand, there were ambivalent aspects regarding communication and the prevention of mistakes. Multiple rotations of physicians will inevitably increase the number of handovers between physicians, which could increase the risk of miscommunications, and the reduced duration of hospital stay per physician may cause communication troubles with patients and co-medical staff. At the same time, it is indicated that careful observation of patient management by multiple physicians can prevent mistakes and improve the level of overall medical care. In order to explore above-mentioned issues in more depth, an exclusively qualitative methodology, for example, one-to-one interviews with the physicians of both attending systems.
A cross-sectional study demonstrated that with more physicians, the accuracy in clinical practice under the team approach will improve. 11 However, several studies indicate that the involvement of multiple professionals in a patient’s care could cause confusion and frustration among physicians, patients, and co-working staff in inpatient care, especially in ICU and end-of-life care.18-22 Management of the end-of-life decision-making varied in relation to multiple and shifting attending responsibilities, and some patient’s families and clinicians were confused about who was making patient care decisions and with whom they should confer. 18 Many patients were unable to name anyone when asked to identify an inpatient physician in charge of their care, 21 and nearly 50% of responding attending physicians knew dying patients for less than 48 hours. 22 According to the present study, this might be just a matter of traditional culture or depend on the severity and urgency of the situation, such as the ICU and acute care hospital. To tackle this problem, the standardization of the handoff process is important since only a few physicians engage in the appropriate handoff process. 23
The limitations of this study are, first, that the data were obtained from a single center, therefore, generalizability of the analysis conducted between 2 physician system might not be significant. Second, although the 2 attending-physician groups in this study worked in common practice areas, we did not collect data from patients and co-working staff. Third, in addition to the number discrepancy of inpatients between 2 groups, physicians from each group had different department background, which might affect the interpretation of the results to some degree. Despite the several research limitations, this is one of the few studies that identified the advantages and disadvantages of the 2 attending-physician systems. Further studies should include the 2 attending-physician systems in the same department or use a larger sample size in a multicenter setting and investigate the satisfaction of patients and healthcare professionals other than physicians in the case of the multiple-attending- physicians-system. Similarly, research should be conducted on the burden of physicians and the quality of care in outpatient settings in Japan.
In conclusion, we have acknowledged that the multiple-attending-physicians system may shorten the average length of hospital stay of patients and also may reduce the physical burden of physicians without compromising their clinical performance. Further future research will be needed on the multiple-attending-physicians system’s potential to improve physicians’ quality of life, promote lifelong learning, and improve the quality of medical care, which may contribute to maintaining medical services at local medical facilities.
Footnotes
Acknowledgements
The authors would like to thank Mr. Ryosuke Kawamoto and Hino Hospital staffs who supported us in completing this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.