
Abstract
Objective:
This study evaluates whether gaining Medicaid following the Affordable Care Act (ACA) expansion led to changes in the rate of acute diabetes complications diagnosed in primary care settings, relative to in inpatient, emergency department (ED), or urgent care (UC) settings.
Methods:
This retrospective cohort study used Medicaid administrative claims data linked to electronic health records for 3767 patients, aged 19 to 64 years, who experienced acute preventable complications of diabetes between 2014 and 2019 diagnosed in inpatient, ED, UC, or primary care settings in the state of Oregon. These patients were classified as either continuously Medicaid-insured or having gained Medicaid.
Results:
Annual rates of acute complications diagnosed in primary care and inpatient/ED/UC settings increased for both continuously [Adjusted Rate Ratio (aRR) = 2.20, 95% CI = 1.65-2.91] and newly Medicaid-insured patients (aRR = 2.67, 95% CI = 2.05-3.47) after the ACA. Among newly Medicaid-insured, annual rates of abnormal blood glucose diagnosed in primary care settings significantly increased with time while those diagnosed in inpatient/ED/UC decreased (2014 vs 2016 aRR = 3.36, 95% CI = 1.60-7.09).
Conclusion:
We found a significantly greater rate of abnormal blood glucose diagnosed in primary care clinics among patients who gained Medicaid post-ACA and a corresponding decline in diagnosis in inpatient/ED/UC settings.
Keywords
Introduction
The prevalence of diabetes mellitus has risen over the past 2 decades and is expected to continue to rise. 1 In 2021, 38.4 million individuals had a diagnosis of diabetes—corresponding to 11.6% of the US population. Diabetes is a leading cause of morbidity, disability, impaired quality of life, and mortality. 2 Diabetes is characterized by hyperglycemia, usually due to progressive loss of insulin secretion from beta cells superimposed on a background of insulin resistance, resulting in insulin deficiency. 3 This pathophysiology may lead to widespread acute complications that can profoundly affect the health and well-being of patients with diabetes. With rising prevalence, there is an overwhelming need for increased access to affordable care for patients with diabetes.
Decades of research have demonstrated that diabetes affects racial and ethnic minority and low-income adult populations in the U.S. disproportionately. 4 These patients face barriers to accessing diabetes care—many lack adequate insurance coverage, do not have access to at-home health monitoring devices, and face food insecurity, increasing their risk for developing diabetes and health complications from diabetes. Furthermore, lack of adequate insurance coverage often leads individuals to seek care in emergency departments (ED) rather than in primary care settings. In 2020, there were approximately 17 million ED visits for adults with diabetes, making it the second most prevalent chronic disease among ED patients.2,5 Additionally, lack of or limited access to primary care clinics presents a barriers to continuity of care, health maintenance education, and effective communication with a single provider, increasing risks for acute diabetes complications. 6
The Patient Protection and Affordable Care Act (ACA) has improved access to healthcare for people with diabetes.7 -10 The ACA made it illegal for insurers to deny coverage or charge higher premiums to people with pre-existing conditions like diabetes, which helped millions of Americans gain coverage without discrimination based on health status. 11 Gaining insurance led to improved access and utilization of primary care clinics and preventive services. 12 Further, 1 previous study found a significantly greater rate of primary care visits for abnormal blood glucose (ABG) in patients receiving care in community-based health clinics (CHCs) in Medicaid expansion states, relative to CHC patients in non-expansion states starting in 2014. 13 The evidence suggests that people without adequate health insurance coverage may forego or delay their care, resulting in higher ED use. However, this study relied on primary care clinic electronic health records (EHR) data only and cannot inform whether corresponding changes in visits for preventable acute diabetes complications are shown in inpatient or ED settings. The present study uses Medicaid administrative claims data linked with EHR data to evaluate whether gaining Medicaid following ACA-related expansions led to changes in the rate of acute diabetes complications diagnosed in primary care clinics relative to inpatient, ED, or urgent care (UC) settings. We hypothesize that those who gained Medicaid following the ACA will demonstrate an increased rate of diagnoses in primary care clinics relative to other settings.
Methods
This retrospective cohort study uses EHR data linked to Oregon Medicaid claims. The EHR data are from the Accelerating Data Value Across a National Community Health Center Network (ADVANCE) of CHCs. 14 ADVANCE data are from the OCHIN (not an acronym) network. OCHIN offers a fully hosted and tailored instance of OCHIN Epic practice management and EHR solutions. The data are centralized and standardized in the ADVANCE data warehouse using the PCORnet common data model. There were 111 clinics in the OCHIN network in Oregon included in the present study. EHR data were necessary to determine insurance status and patient characteristics. The study period is 2014 to 2019. The years 2012 and 2013 were utilized to determine insurance status prior to 2014.
Medicaid enrollment, outpatient, and inpatient administrative claims data are from the Medicaid Management Information System of the Oregon Health Authority. Patient-level linkages were created between the EHR and Medicaid data using each individual patient’s Oregon Medicaid identification number, a unique identifier appearing in both data sources.
The sample was selected using EHR and Medicaid claims data. Using EHR data, patients were included if they were age 19 to 64 years (adult Medicaid eligibility), had a diagnosis of diabetes, and had at least 1 ambulatory visit at one of the Oregon OCHIN clinics between 2012 and 2019. The years 2012 and 2013 were utilized to determine insurance status prior to 2014. Patients who were pregnant between 2012 and 2019 or who had Medicare coverage were excluded as these patients have different care needs and/or coverage benefits. Using the claims data, we selected patients who had at least 1 diagnosis of an acute diabetes complication (in any setting). The sample included 3767 adult Medicaid-eligible patients with diabetes.
Medicaid coverage status was determined using EHR-based billing data and Medicaid enrollment data and categorized as continuously Medicaid insured and newly Medicaid insured (gained Medicaid coverage) after the 2014 ACA, when Oregon expanded Medicaid to adults with incomes at or below 138% of the federal poverty level (FPL). Newly insured patients (n = 3023) included those who were uninsured prior to 2014 and were enrolled in Medicaid between 2014 and 2019. To determine whether these patients were uninsured prior to 2014, we selected those with no record of Medicaid enrollment and/or who had no insurance at all visits in the EHR in 2012 and/or 2013. Continuously insured patients (N = 744) were those enrolled in Medicaid prior to and after 2014.
The main outcome was rate of acute diabetes complications diagnosed in 2014 through 2019. Medicaid claims were used to identify acute diabetes complications diagnosed in inpatient, ED, UC, and primary care settings. Acute complications were identified using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) and ICD-10-CM codes. We followed Wharam’s et al 15 classifications and included preventable acute complications that would primarily be diagnosed in outpatient settings. Acute complications were classified into 12 categories: abnormal blood glucose; acute kidney failure; cardiac arrest; congestive heart failure; glaucoma; hyperkalemia; hypertensive emergency; hypotension or shock; infections; myocardial infarction or transient coronary artery ischemia; non-cardiac, non-cerebral artery complications; and stroke, transient neurological deficit, or cerebral artery occlusion.
Acute complication diagnoses had to occur on or after the diagnosis of diabetes and were counted as distinct complications if the interval between diagnostic encounters was at least 10 days to reduce duplicate entries. If an acute complication was diagnosed in multiple settings on the same date or within 10 days, they were assigned to the setting with highest level of care or urgency following this ranking order: inpatient, ED, UC, and primary care.
The main independent variable was the setting in which the acute complications were diagnosed. The setting was categorized as a binary indicator: inpatient, ED, UC versus primary care.
Characteristics of patients with diabetes included the following sociodemographic and health-related factors: sex, age (19-44 and 45-64), race and ethnicity (Hispanic, non-Hispanic black, non-Hispanic other, non-Hispanic white, and missing), federal poverty level (≤138% FPL and >138% FPL), body mass index (<25 and ≥25 kg/m2) at last visit in the study period, ever prescribed insulin, glycosylated hemoglobin (HbA1c) following Centers for Medicare & Medicaid Services quality metric 16 to determine uncontrolled status (average HbA1c >9.0 over the study period), Charlson comorbidity score, and number of ambulatory visits over the study period.
Analysis
We summarized the characteristics of the patient population overall. To model rates of acute diabetes complications diagnosed in 2014 through 2019 by setting, we performed generalized estimating equation (GEE) modeling, assuming a negative binomial distribution, incorporating a log link function with clustering on patients to account for the correlation of visits within patients using an exchangeable working correlation structure. GEE regression models included a main effects and interactions between categorical time and indicators for care settings. GEE models also included variables for patient self-reported race and ethnicity, age, sex, federal poverty level, patient geographic location (urban, suburban, and rural), Charlson score, body mass index, insulin prescription, and uncontrolled diabetes. Similar GEE models were applied for abnormal blood glucose complications. All models were stratified by insurance status (continuously and newly Medicaid-insured). We displayed unadjusted rates and model adjusted rates of acute diabetes complications by insurance status, care setting, and year. Statistical tests were performed with a 2-sided α = .05. Analyses were conducted using R Core Team (2021) and Stata version 17.0 (StataCorp 2021).
The study’s protocol was approved by Institutional Review Board
Results
Table 1 shows the descriptive characteristics of patients with diagnosed diabetes-related acute complications. The patient population was aged 45 to 64 years (73%), most had BMI ≥ 25 kg/m2 (85%), had controlled diabetes (66%), and resided in urban areas (68%).
Characteristics of 3767 Patients With Diabetes With Acute Complication During the Study Period 2012 to 2019 Receiving Care in 111 Oregon Community Health Centers.
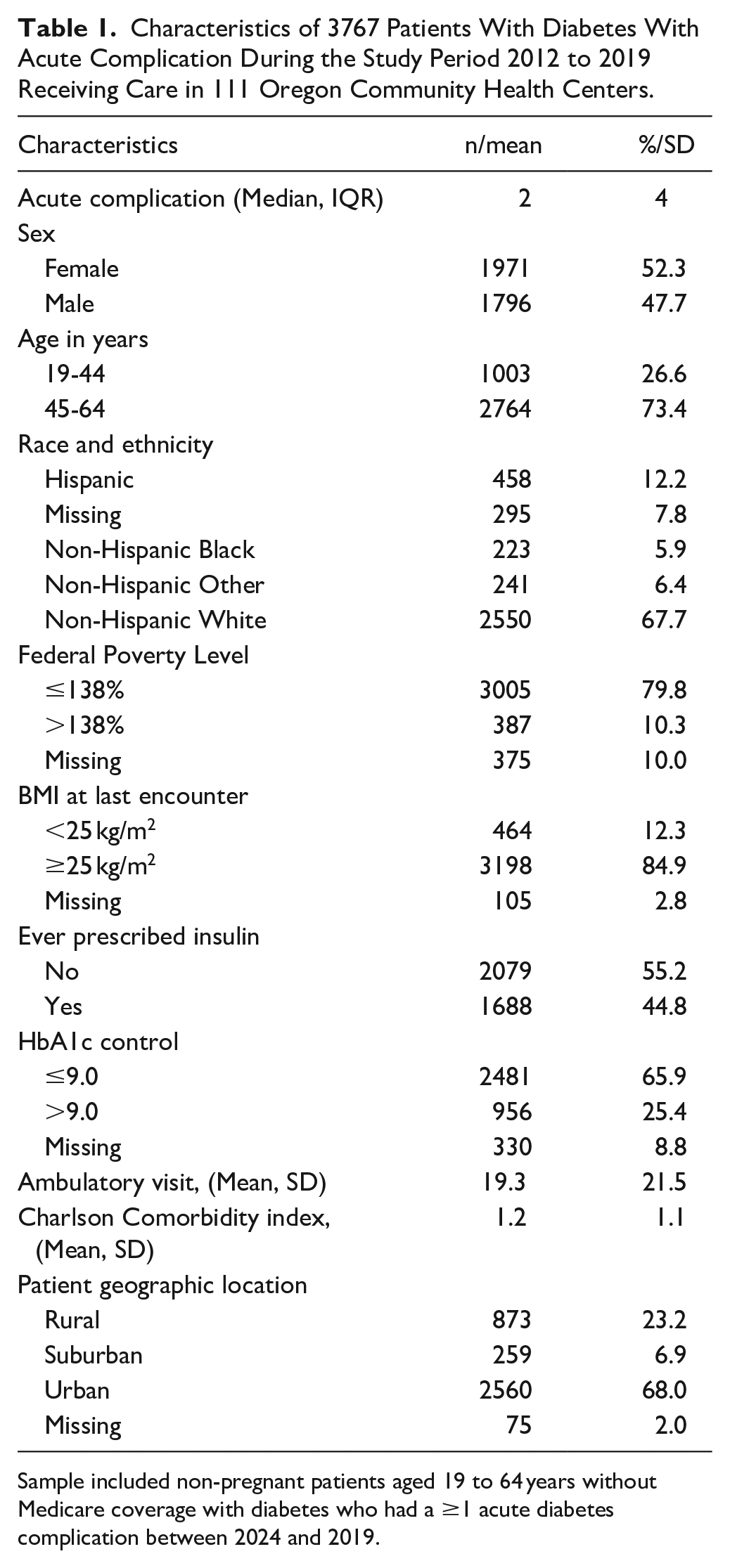
Sample included non-pregnant patients aged 19 to 64 years without Medicare coverage with diabetes who had a ≥1 acute diabetes complication between 2024 and 2019.
Figure 1 shows the unadjusted annual rates of acute complications per 100 patients diagnosed in inpatient/ED/UC versus primary care stratified by patients who gained Medicaid coverage (Panel A) and those that were continuously insured by Medicaid (Panel B). Among those who gained Medicaid, more acute complications were diagnosed in primary care clinics than in inpatient/ED/UC settings [Adjusted Rate Ratio (aRR) = 2.67, 95% CI = 2.05-3.47; Table 2]. Similarly, those continuously insured by Medicaid had more acute complications diagnosed in primary care clinics than in inpatient/ED/UC (2019 aRR = 2.20, 95% CI = 1.65-2.91). The number of diagnosed acute complications significantly increased overtime regardless of settings (Table 2).

Annual rate of acute diabetes complications by insurance status, care settings, and year.
Adjusted Rate Ratios of Acute Diabetes Complication Diagnosed in Primary Care Versus Inpatient/ER/UC From 111 Oregon Community-based Health Centers.

Adjusted for sex, age, race/ethnicity, FPL, BMI, Charlson comorbidity score, uncontrolled diabetes, insulin prescription, patient geographic location. Bolded are significant at p < .05.
Figure 2 shows the unadjusted annual rate of abnormal blood glucose complications per 100 patients diagnosed in inpatient/ED/UC versus primary care stratified by gained Medicaid coverage (Panel A) and continuously insured by Medicaid (Panel B). The trend in abnormal blood glucose complications being diagnosed in primary care among those who gained Medicaid significantly increases with time while the trend for inpatient/ED/UC decreases from 2014 to 2016 and then stabilizes (Figure 2). Among those who gained Medicaid, starting in 2016, the increase in abnormal blood glucose complications diagnosis was significantly greater in primary care setting than in inpatient/ED/UC (2016 gained Medicaid aRR = 3.36, 95% CI = 1.60-7.09; Table 2). Among those continuously insured by Medicaid, the rate of abnormal blood glucose diagnosed in primary care significantly exceed the rate of diagnosis in inpatient/ED/UC only in 2018 and 2019 (Table 2).

Annual rate of abnormal blood glucose complications by insurance status, care settings, and year.
Discussion
We found that individuals who gained Medicaid following ACA expansion in Oregon had an increase in abnormal blood glucose complications diagnosed in primary care settings and a decline in abnormal blood glucose complications diagnosed in inpatient/ED/UC settings, supporting our hypothesis. This change could suggest more frequent primary care visits and continuity with a single health care provider, which can more consistently track diabetes progression, further preventing acute complications. Continuity of care allows patients the opportunity to build a trusting relationship with their primary care provider, establishing a level of care that would be otherwise impossible to achieve in a single inpatient, UC, or ED visit. This ongoing therapeutic relationship offers significant positive health outcomes, where patients may be encouraged to have regular visits with their primary care provider, follow up about possible concerns, and have opportunities to inquire and be educated about how to better manage their diabetes and to identify complications early. 17 Furthermore, the positive effects of high-quality continuity of care on the treatment outcomes of patients with diabetes depends on the level of disease severity. 18 Therefore, providing high quality continuity of care by a primary care provider, when the disease severity is low, may be critical for ensuring optimal positive effects during the chronic disease progression.
Beyond the immediate benefits for patients, this may also suggest that providers have expanded capacity or participation in Medicaid following the expansion and are meeting increased demands for care. Studies in this area show an association between expansion and increases in primary care appointment availability. 19 Evidence also demonstrated improvements in receipt of checkups, care for chronic conditions, and quality of care, even in areas with primary care shortages, suggesting that insurance expansions can have a positive impact in areas with relative shortages.7,8,12,20
Further, the ACA insurance reforms were expected to have positive implications for hospital finances; in particular, state expansion of Medicaid programs held the promise of reducing hospitals’ uncompensated care costs by expanding health insurance to many previously uninsured individuals who used ED and inpatient care as their primary source of care. 21 Switching care from ED to primary care settings is also cost saving for the Medicaid program. Previous studies have shown that the influx of Medicaid-insured patients following the ACA expansion did not lead to overuse of care. 22 These studies show a pent-up demand for care in outpatient settings immediately following the Medicaid expansion that plateau quickly and remain lower than care used by continuously insured Medicaid patients. Removing financial barriers to care increases access to preventive and chronic care management and could reduce the incidence or severity of diabetes complications. Early detection and adequate treatment of acute complications are anticipated to be less costly than the treatment of uncontrolled diabetes and multiple new chronic conditions. 23
These population health benefits, however, may be reversing themselves in expansion states following the mass disenrollment (AKA: unwinding) of Medicaid coverage. As of May 1, 2023, states began ending pandemic-related continuous coverage for people requiring eligibility redetermination and leading to more than 25 million people being disenrolled to date. 24 Alarmingly, a new study found that among socioeconomically disadvantaged patients with diabetes who lost Medicaid coverage, nearly half stayed uninsured and only 11% enrolled in private plans. 25 It is unknown what impact this “unwinding” of Medicaid coverage will have on patients’ ability to manage their diabetes; however, it can be expected to lead to an uptick in hospital’s uncompensated care costs and an increase in ED usage.
Several limitations must be acknowledged. The Centers for Disease Control and Prevention 2 report that nearly 1 in 4 individuals with diabetes are undiagnosed. This study may underestimate the rate of patients with diabetes and/or of diabetes-related complications. Furthermore, a chronic metabolic syndrome such as diabetes, may present with comorbidities that extend beyond the acute complications used in this study, and would therefore be related to the alternative diagnosis, rather than being a direct acute complication of diabetes. For instance, congestive heart failure and cardiac arrythmias may be acute complications of COPD, a common comorbidity of diabetes. Another limitation of note is an increase in awareness of abnormal blood glucose levels in 2015. In 2015, the U.S. Preventive Services Task Force (USPSTF) strongly suggested that the regulation of abnormal blood glucose levels serves as a benefit of early detection, and therefore treatment. 26 This change in awareness may have led to improved documentation of abnormal blood glucose complications in the medical record, which could overestimate the effect observed in this study. Lastly, our study is limited to the state of Oregon, findings may not be generalizable to other states.
In conclusion, these results show a shift in abnormal blood glucose being diagnosed in primary care instead of inpatient/ED/UC post-Medicaid expansion. This study aligns with numerous other studies demonstrating the positive impact of the ACA on health outcomes.
Footnotes
Acknowledgements
The authors acknowledge the significant contributions to this study provided by collaborating investigators in the NEXT-D3 (Natural Experiments in Translation for Diabetes 3.0) Study. The research reported in this work was powered by PCORnet®. PCORnet has been developed with funding from the Patient-Centered Outcomes Research Institute® (PCORI®) and conducted with the Accelerating Data Value Across a National Community Health Center Network (ADVANCE) Clinical Research Network (CRN). ADVANCE is a Clinical Research Network in PCORnet® led by OCHIN in partnership with Health Choice Network, Fenway Health, University of Washington, and Oregon Health & Science University. ADVANCE’s participation in PCORnet® is funded through the PCORI Award RI-OCHIN-01-MC.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was jointly supported by the Centers for Disease Control and Prevention (CDC) and National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), grant (U18DP006536). The content is solely the responsibility of the authors and does not necessarily represent the official views of the CDC or NIDDK.
Ethical Approval
The study’s protocol was approved by Oregon Health and Science University’s Institutional Review Board (ID# IRB00011858).
Data Availability
Raw data underlying this article were generated from multiple health systems across institutions in the ADVANCE Network; restrictions apply to the availability and re-release of data under organizational agreements.