
Abstract
Introduction/Objectives:
New variants of the SARS-CoV-2 virus that causes COVID-19 will continue to develop and spread globally. The Omicron variant identified in November 2021 has many lineages. Variants spread quickly and can infect previously vaccinated individuals, prompting the Centers for Disease Control and Prevention to update vaccination recommendations. While ~230 million Americans received the initially-recommended vaccine sequence, booster uptake has been much lower; less than half of fully vaccinated individuals report receiving a booster. Racial disparities also mark patterns of COVID-19 vaccination booster uptake. This study explored willingness and motivations to get a COVID-19 booster among a diverse sample of participants.
Methods:
We used convenience sampling to recruit participants 18 years of age or older who attended a community vaccine event. We conducted informal interviews during the recommended 15-min post-vaccination wait time with 55 participants who attended vaccine events at Marshallese and Hispanic community locations and comprised the recruitment pool for individual interviews. Using a qualitative descriptive design, we conducted in-depth follow-up interviews with 9 participants (Marshallese n = 5, Hispanic n = 4) to explore willingness and motivations to get boosted. We used rapid thematic template analysis to review informal interview summaries and formal interviews. The research team resolved data discrepancies by consensus.
Results:
Participants reported high willingness to get boosted, especially if boosters were recommended in the future to protect against serious illness and mitigate the spread of COVID-19. This finding underscores how essential including recommendations to get a COVID-19 booster from trusted sources in health messaging and educational campaigns may be for increasing booster uptake. Participants described their preference for receiving future COVID-19 boosters, reporting that they would attend similar vaccine events, especially those held at faith-based organizations and facilitated by the same community partners, community health workers, and research staff. This finding shows how community engagement can overcome barriers to vaccination (ie, transportation, language, and fear of discrimination) by providing services in preferred community locations with trusted community partners.
Conclusions:
Findings document high willingness to get a COVID-19 booster, emphasize the role of recommendations from trusted sources in motivating booster uptake, and highlight the importance of community engagement to address disparities in vaccination coverage and reach.
Keywords
Introduction
The emergence of the Omicron SARS-CoV-2 variants, which spread quickly and can infect previously vaccinated individuals, prompted the Centers for Disease Control and Prevention (CDC) to update COVID-19 vaccination recommendations.1,2 An updated bivalent booster to protect against the original virus and the Omicron variants became available on September 2, 2022; the CDC recommends that people ages 5 years and older receive 1 updated booster if it has been at least 2 months since they received their last COVID-19 vaccine dose. 2 Although almost 230 million Americans received the initially recommended vaccine sequence, booster uptake has been much lower. 3 Less than half (48.5%) of fully vaccinated individuals have received a booster dose, and variation exists across geographic location, occupation, and sociodemographic characteristics. 4 Racial disparities also mark patterns of COVID-19 vaccination booster uptake. In multiple population-based surveys, white adults were up to twice as likely to receive a bivalent booster shot as Hispanic, Black, or Native Hawaiian/Pacific Islander (NHPI) adults.3,5 Lower vaccination coverage rates among minority populations exacerbate persistent disparities in adverse COVID-19-related outcomes for these vulnerable communities.6,7
Arkansas, a southern state with low vaccine coverage, has also experienced significant COVID-19-related disparities, especially among racial and ethnic minority communities. The state is well below the national average of 81.15% for COVID-19 vaccination coverage, with only 57.1% of the state’s population fully vaccinated (ie, received the required number of doses for each specific COVID-19 vaccine but not a booster). 8 The racial and ethnic diversity of the Arkansas population has grown by 10% from 2010 to 2019. 9 Northwest Arkansas is home to a diverse population that includes prominent Marshallese Pacific Islander and Hispanic communities whose members faced significant COVID-19-related disparities such as hospitalization and death. 10 After a site visit in June and July 2020 to investigate these substantial disparities, the CDC reported that 45% of all adult COVID-19 cases in Northwest Arkansas identified as Hispanic, and 19% identified as Pacific Islander, despite accounting for 17% and 2.4% of the region’s population respectively. 11 An interdisciplinary research team from the University of Arkansas for Medical Sciences (UAMS) engaged their existing community-based participatory research (CBPR) collaborative to leverage its capacity to address these COVID-19 disparities with a comprehensive strategy to support community members through the pandemic. 12 The CBPR collaborative is focused on improving community health outcomes and reducing health disparities through research and program implementation.
Recent research has documented participant willingness to get a COVID-19 booster and its association with various social determinants of health (eg, zip code, employment, and educational attainment) and other sociodemographic variables (eg, gender, race, and ethnicity).4,5,13-15 However, gaps in our understanding of booster uptake remain, with no qualitative studies focused on participants’ perceptions of the factors related to their willingness to get a COVID-19 vaccine booster or studies documenting these factors among diverse racial and ethnic groups, such as Marshallese and Hispanic populations. Identifying these factors is critical to designing health communications and vaccination programs that meet the needs and concerns of disproportionately impacted communities. To fill these gaps, our exploratory study aimed to understand the willingness to get a COVID-19 booster shot among a diverse racial and ethnic sample of participants in Arkansas.
Methods
Setting and Intervention
The COVID-19 pandemic disproportionately impacted members of the Marshallese and Hispanic communities of Northwest Arkansas, who experienced significant COVID-19-related disparities in illness, death, and hospitalization. 11 The largest population of Marshallese in the continental United States (US) is found in Northwest Arkansas, and the Hispanic community comprises more than 15% of the area’s population.11,16
The existing CBPR collaborative was leveraged to facilitate community-based COVID-19 vaccination outreach events in community faith-based organizations (FBOs).16-18 This CBPR research collaboration engaged community partners in developing a comprehensive strategic pandemic response of community outreach that included health education, testing, contact tracing, case management, and quarantine support before vaccine development.12,16 The CBPR collaborative has engaged Marshallese and Hispanic community leaders, non-profit organizations, and FBOs to address community-identified health priorities since 2012. Beginning in 2012, the research team initiated a CBPR approach, building trust with community stakeholders by engaging them in all aspects of the research process and incorporating cultural knowledge, practices, and values into research design, implementation, evaluation, and dissemination of findings.18,19
A 2020 CDC assessment among Marshallese and Hispanic community members identified language and a lack of information as barriers to vaccination. 10 The CBPR partners developed culturally and linguistically appropriate COVID-19 vaccine and vaccination informational materials and used multiple dissemination strategies like infographics, social media posts, local radio and news broadcasts, and direct community outreach by bilingual (Marshallese and English or Spanish and English) staff, bilingual community health workers (CHWs), and community partners. 12 Transportation and lack of access to COVID-19 vaccine sites were other barriers community members reported, 9 of which prompted the CBPR collaborative to implement vaccine events in community locations (churches, community centers, and job sites) as well as a drive-thru option at a health system location to increase reach. 12 Bilingual CHWs and research staff facilitated these vaccine events and provided interpretation at each stage of the vaccination process. Additionally, the CBPR collaborative secured extramural funding to integrate research projects into the vaccine events to assess participants’ COVID-19 vaccine attitudes and behaviors and conduct an implementation-focused analysis of the community vaccine events quantitatively with surveys and qualitatively through participant interviews and focus groups.
Study Design, Aims, and Approach
The study aimed to understand participants’ willingness to receive a COVID-19 booster dose and explore factors that motivate participants to get boosted using a qualitative descriptive design.20-22 Community stakeholders contributed to developing study aims and design, facilitating participant recruitment and promoting vaccine events, hosting vaccine events, facilitating data collection, and providing regular feedback to the research team. The UAMS Institutional Review Board approved all study materials and procedures (IRB #262917).
Participant Recruitment
Potential participants for individual interviews were approached at community faith-based vaccine events held at Marshallese (n = 4) and Hispanic (n = 2) churches and a local FBO that provided social, health, and material support services to the community (n = 1) from July 2021 to September 2021. During the recommended 15-minute post-vaccination wait time when vaccine side effects were being monitored, bilingual Marshallese and Hispanic study staff conducted informal interviews about the vaccination experience with 55 participants who had received at least 1 dose of a COVID-19 vaccine in their initial series. These 55 participants comprised the recruitment pool for the individual interviews. Participants who agreed to be contacted to participate in a longer, semi-structured interview were contacted by bilingual study staff via email or phone in their preferred language (Marshallese, Spanish, or English) and invited to participate. Before the interview, participants who chose to participate were provided with a study information sheet to review and given time to ask questions. Participants provided verbal and written consent in their preferred language, and consent was recorded in REDCap.23,24 Participants who completed an individual interview were given a $40 gift card for remuneration.
Data Collection
Study staff initially conducted 55 informal interviews with participants to explore their motivations for attending the community vaccine events offering free initial COVID-19 vaccinations held in Marshallese and Hispanic community locations. Before the start of data collection, a qualitative research expert provided informal interview training to bilingual study staff who conducted informal interviews from July to September of 2021. Informal interviews were brief and conversational, with an average length of 3 to 5 min. For consistency across informal interviews, a semi-structured interview guide was used and focused on why participants attended the event, how they decided to get (initially) vaccinated, barriers/facilitators they experienced in attending the event, how to improve future events, and their general perceptions about COVID-19 vaccines (see Figure 1). Staff members were instructed to allow the conversation to “go where the participant takes them” by following participant cues.

Semi-structured interview guide questions that were used to facilitate formal, individual participant follow-up interviews.
Study staff who have completed community health worker training as well as qualitative research methods training and have over 5 years of experience facilitating qualitative research with Marshallese and Hispanic community members conducted the individual follow-up interviews with 9 participants (Marshallese n = 5 and Hispanic n = 4) between July 19, 2021 and September 1, 2021. Staff conducted interviews via phone, via Zoom, or in person based on participants’ preferences, and they used a semi-structured interview guide to ensure consistency across interviews. The research team used items from the Behavioral Risk Factor Surveillance System survey 25 to collect participants’ socio-demographic characteristics such as age, educational attainment, employment, and salary. Participants were interviewed before the COVID-19 booster rollout. Participants were asked if they would be willing to take future recommended additional COVID-19 vaccine boosters and, if so, what they would want the experience of getting a booster to be like. Interviews were facilitated in the participants’ preferred language and varied in length, ranging between 11 and 41 minutes.
Qualitative Data Analysis
Informal interviews were summarized in written memos by interviewers. After the first 2 events, interviewers participated in debriefs with research staff and reviewed informal interview summary memos. The formal individual interviews were recorded, professionally transcribed verbatim, translated into English by Marshallese and Hispanic certified translators, and de-identified for analysis. Bilingual study staff who facilitated the interviews checked interview translations for accuracy before analysis. The analysis team used rapid thematic analysis of the informal interview summaries and the formal interviews that followed a modified Framework approach.26,27 Two researchers with qualitative expertise began initial coding by reading all transcripts and incorporating emergent codes into a coding template. The analysis team met regularly and discussed discrepancies in data interpretation, which were reviewed, debated, and resolved by consensus. The analysis team wrote, reviewed, and discussed coding memos summarizing and interpreting data in an iterative process to reduce potential bias and ensure scientific rigor and intercoder reliability. 28 To identify patterns and outliers, coded data was summarized and imported into a visual chart with a column for each theme and a row for every participant. Illustrated quotes were identified and incorporated into the coding framework and final templates. Before conducting the individual interviews, the analysis team conducted a rapid content analysis to code the informal interview summaries, and the coded summaries were used later for data triangulation to verify that data saturation had been reached with the formal interviews and that no additional codes had emerged. The analysis team presented the initial coding framework, emergent themes, and findings at weekly analysis meetings attended by the authors. As part of the larger study, 6 qualitative researchers completed confirmation coding by critically reviewing all data, templates, and coding memos and discussing and resolving discrepancies in data interpretation by consensus. The analysis team identified 2 primary themes: (1) participants’ willingness to receive future recommended COVID-19 boosters and (2) recommendations for future booster experience. Emergent subthemes for each primary theme are also presented below.
Results
Participant Characteristics
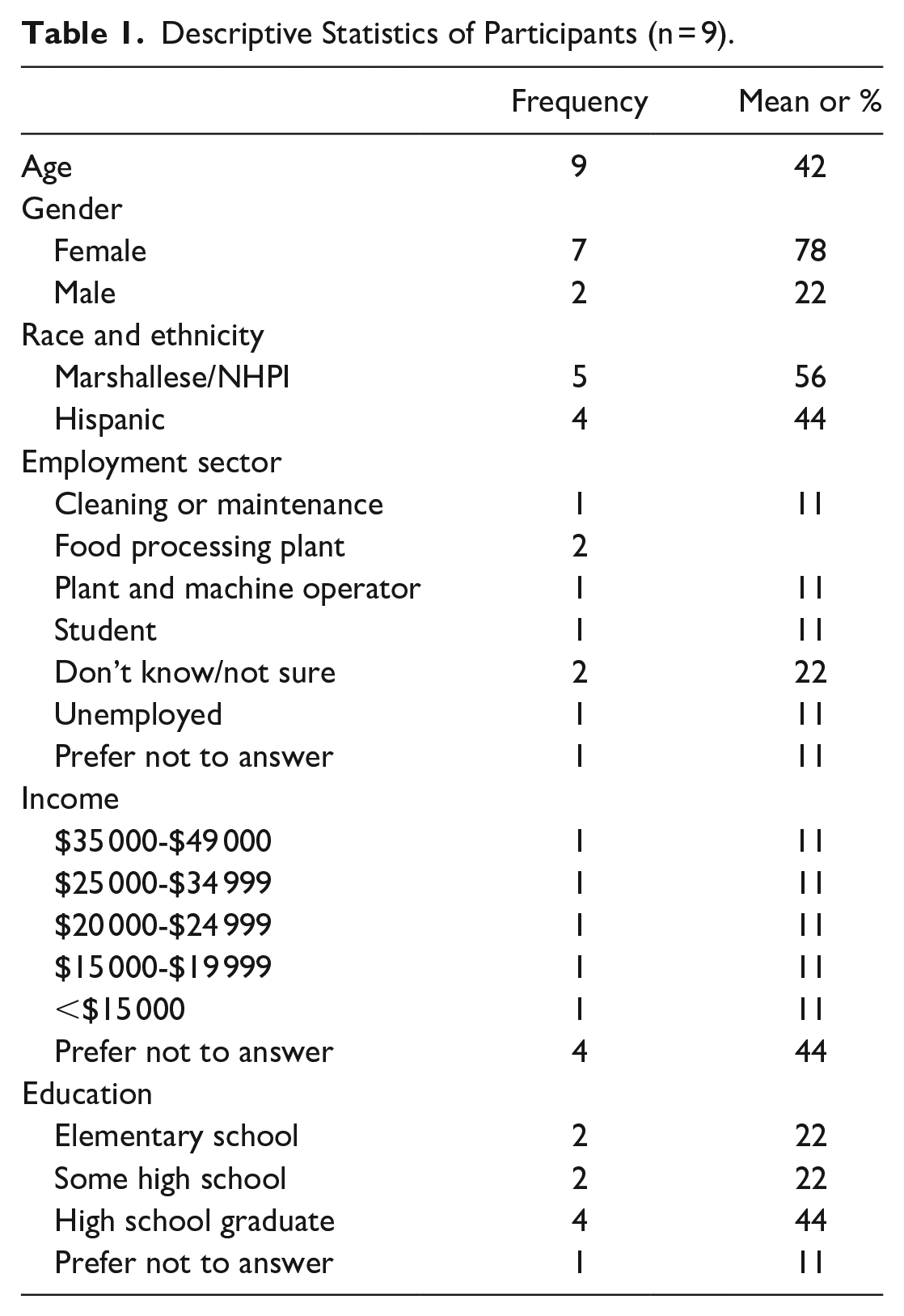
All 55 informal interviews were with participants who attended community vaccine events held in Marshallese and Hispanic communities. Among the 9 formal interviews, 5 participants (56%) identified as Marshallese Pacific Islanders, and 4 (44%) identified as Hispanic. Seven participants were female (78%), and the average age of participants was 42 years (Table 1).
Descriptive Statistics of Participants (n = 9).
Qualitative Findings
Participants discussed whether they would be willing to get a future COVID-19 booster and described their preferences for how they would like to receive their booster shot. The research team identified 2 emergent primary themes occurring across all interviews: (1) participants’ willingness to receive future recommended COVID-19 boosters and (2) recommendations for future booster experience.
Participants’ willingness to receive future recommended COVID-19 boosters
Participants unanimously reported they were willing to get a COVID-19 booster if it was recommended in the future. Researchers identified 3 emergent subthemes in this primary theme: (1) if a booster is recommended or “necessary” to protect against new variants, (2) boosters become routine like annual flu shots, and (3) previous vaccination experience reduces fear and encourages booster willingness.
If a booster is recommended or “necessary” to protect against new variants
Discussing their willingness to get a COVID-19 booster, participants stated, “Yes, if it’s necessary, I would do it” (54 year old Hispanic female) and “Yes, I have to take [the recommended booster] to prevent other virus [strains], so they will not affect us.” (57 year old NHPI female) A participant stressed they would get the booster if a medical professional recommended it: “There are things that cannot be controlled with 1 dose. I understand that. If I see it’s necessary, I’ll get it and make everybody else get it. I wouldn’t have a problem as long as it’s necessary.” (34 year old Hispanic female) Other participants said, “We will wait for them [medical professionals to] say we will need to get vaccinated again” (35 year old NHPI male) and “ if other viruses are [discovered], and we’re told to get vaccinated, well, I will take it again.” (22 year old NHPI female)
Boosters become routine, like annual flu shots
Participants often discussed their willingness to get COVID-19 boosters in the context of their previous experiences with the yearly flu vaccines. Some participants expressed their willingness to receive a COVID-19 booster annually, like a flu shot, if needed to protect against and prevent COVID-19 infection. One participant summarized, “Just like the flu shot, in years to come, if COVID vaccination are available yearly, then I’ll take it, to better protect ourselves.” (22 year old NHPI female) Another participant who did not get an annual flu shot said, “If they do [the COVID booster] like the one for the flu since this one is jumping all over among everybody, this one I would take it to prevent it from spreading because this thing jumps again and again and starts to mutate, so if we can prevent it by getting vaccinated each year, we should try to do it.” (59 year old Hispanic female) Other participants noted a positive personal experience with prior flu and COVID-19 vaccinations, influencing their willingness to get a booster. A participant explained, “I have taken my flu shot and the COVID-19 vaccines. Now, I won’t listen to any negative information about the vaccines. I will make sure I take all the vaccines that I need. There will be no question about it.” (54yr old NHPI female)
Previous vaccination experience reduces fear and encourages booster willingness
Vaccination events at well-known community FBOs were preferred locations for future COVID-19 boosters because participants said they felt comfortable and at ease there. Participants explained that getting a booster at a similar vaccine event could reduce participant fears since they know what to expect. Providing culturally and linguistically appropriate vaccine information at vaccine events with CHWs increased participants’ trust and may encourage a greater willingness to get a booster shot. Participants discussed the importance of CHWs who helped them navigate the process at the vaccination events. When describing how they would like to obtain a future COVID-19 vaccine, a participant summarized why they wanted to return to a similar vaccine clinic event: In the community where I went, because one, the language, and two, I feel more confident about communication. I know they can explain things to me. There are people who might understand the same that I do, and they may have the same doubt, and they have the same language, and I can start talking to more people from the community. To know, to understand. Instead of going to a place where I feel like a stranger and all that. I prefer [to get the booster] there. (34yr old Hispanic female)
Another participant explained that “If there are vaccines where I went [before], I [will] go there and get it again because I felt really comfortable as if I were at home. I was at ease. You don’t make people feel unwanted because of our race or whatever.” (59 year old Hispanic female) A participant echoed this desire to obtain their future booster at a similar vaccine clinic: “I think that the event where you were, I think it was very good there. I would say it’s better there so that we don’t feel embarrassed or get afraid to go somewhere else.” (54 year old Hispanic female)
Informal interview participants described the positive influence of others on their decision to get the COVID-19 vaccine with greater frequency than they reported deciding on their own to get vaccinated. Participants said family members, church leaders, friends, doctors, and co-workers encouraged them to get a COVID-19 vaccine; they reported that knowing others’ vaccination experiences helped to address their vaccine hesitancy.
Recommendations for future booster experience
Participants described their preferences for how they would like to receive future COVID-19 boosters. Researchers identified 1 emergent subtheme: future boosters should be distributed at community-based FBO events facilitated by the CBPR collaborative.
Future boosters should be distributed at community-based FBO events facilitated by the CBPR collaborative
Participants said they would be willing to get a COVID-19 booster at similar community events where information and vaccination are provided or facilitated by UAMS staff and community partners in vaccine events held in FBOs. A participant explained, “We will choose the same organization that came to conduct the vaccine event because they came to help us with other services, and they really did welcome us to the vaccine event. We like to do it where we know the people in that place, and we can get [the] right information about the vaccines or other questions we have.” (54 year old NHPI female) Another participant who received their COVID-19 vaccine at the event said, “I have records of my immunization with them, and that is where I choose to take my [future] vaccine.” (22 year old NHPI female)
Informal interview participants also recommended that the CBPR collaborative conduct future booster events at community FBOs for the convenience of the event, location, time, and ease of the process. Informal interview summaries showed no overarching barriers or suggestions for improving vaccine events and processes. However, there were recommendations for more community outreach, including booster vaccine events.
Discussion
This exploratory study documented willingness to receive a COVID-19 booster and recommendations for how future boosters could be administered among Marshallese and Hispanic participants in Arkansas. Marshallese and Hispanic participants reported a high willingness to get boosted, especially if COVID-19 booster shots were recommended in the future to protect against serious illness and mitigate the spread of COVID-19 infections. These findings are consistent with at least 1 study documenting a high willingness to take a booster dose. 14 However, a recent study with vaccinated US adults found that racial and ethnic minority respondents had lower booster uptake than White respondents. 5 A recent study assessing disparities in booster uptake among vaccinated US adults found lower booster uptake among female respondents, uninsured respondents, and respondents with lower-educational and income levels. 5
Boosted individuals are more likely to be male, to reside in the Northeast, and to work in hospitals. Black, Hispanic, and other/multiple race respondents are less likely to be boosted than White individuals.4,5,13 Studies assessing individuals’ willingness to get a COVID-19 booster show high intention; however, booster hesitancy is associated with low vaccine literacy, living in the South, and lower educational attainment.4,5,14 The literature shows booster acceptability increases for individuals who report having pre-existing conditions, living with vulnerable family members, and having COVID-19-positive friends or family members. 14 A randomized choice-based analysis of US adults evaluating the influence of contextual information about a novel variant found that the most important factors associated with increased willingness to receive a booster were vaccine efficacy, manufacturer, and the size of a financial incentive. 15
The study findings also highlight the importance of recommendations encouraging booster uptake, 15 especially from trusted sources for vaccine information such as health professionals, cultural and faith leaders, family members, friends, and co-workers that might encourage greater vaccine uptake.29-36 A recent study found that participants (n = 1594) who increased their trust in and consumption of official information sources, like healthcare providers and public health officials, were more likely to get a COVID-19 booster. 37 Our qualitative findings underscore how essential including recommendations to get a COVID-19 booster from trusted sources in health messaging and educational campaigns may be for increasing booster uptake.
Participants expressed willingness to receive a future COVID-19 booster if it could be given like an annual flu shot. This supports our previous research finding that participants who received an annual flu shot were less hesitant to get a COVID-19 vaccine. 38 Our findings highlight that provider recommendations of COVID-19 boosters to patients who routinely get a flu shot may increase vaccine uptake.
When asked how they would like to get a future COVID-19 booster, participants said they would like to receive any future boosters at similar community vaccine events, especially those held at FBOs and facilitated by the same community partners, CHWs, and research staff. This novel finding underscores the success of the CBPR collaborative’s strategic pandemic response to leverage its existing research and programmatic infrastructure in support of community members. 39 Our findings show how community engagement can overcome significant barriers to vaccination, like transportation, language, and fear of discrimination for participants, by providing vaccine services in preferred community locations with trusted community partners.
Limitations
The study has limitations. First, findings may not be generalizable due to the small sample size. However, generalizability is not the main objective of qualitative exploration. Our findings provide nuance and context from insiders’ perspectives about the willingness to receive a future COVID-19 booster and recommendations for booster rollout that can inform future research that seeks generalizability. Secondly, findings may not represent the diverse experiences and perceptions of the Marshallese and Hispanic communities. For example, only a few participants explicitly stated whose recommendation would increase their willingness to get a booster, which future research should work on clarifying and documenting. Using data source triangulation showed that formal interview findings corroborated informal interview summaries. Third, the location setting is a possible limitation as participants comprise a convenience sample drawn from community vaccine events offering free initial COVID-19 vaccination, which may make participants more likely to report willingness to receive a future booster in the same location. Despite these limitations, the study documents a high willingness to get the COVID-19 booster among Marshallese and Hispanic community members. The study findings highlight how community engagement could inform future community-based interventions to increase COVID-19 booster uptake and other routine vaccinations, such as flu, and improve health equity in vaccine coverage.
Conclusion
The study findings document high willingness among Marshallese and Hispanic participants to get a COVID-19 booster shot. Our findings emphasize the importance of recommendations from trusted sources to get a booster to protect from a serious illness. The study findings highlight potential opportunities for healthcare providers to recommend COVID-19 boosters to patients who routinely receive a flu vaccine. We also document the importance of community engagement to address disparities in vaccination coverage and vaccine reach.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support was provided by the Community Engagement Alliance (CEAL) Against COVID-19 Disparities (NIH 10T2HL156812-01); Rapid Acceleration of Diagnostics (RADx; NIH 3 R01MD013852-03S2); University of Arkansas for Medical Sciences Translational Research Institute funding awarded through the National Center for Advancing Translational Sciences of the National Institutes of Health (NIH; UL1 TR003107); and the Office of Minority Health of the U.S. Department of Health and Human Services (HHS; 1 CPIMP211231-01-00). Dr. Jennifer L. Vincenzo was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under award number KL2 TR003108. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funders.