
Abstract
Background:
The COVID-19 pandemic has posed significant global health challenges, requiring mass vaccination to reduce severe illness and mortality. Despite strong evidence supporting booster dose safety and efficacy, uptake remains low due to widespread hesitancy. This study aims to comprehensively explore the factors contributing to first COVID-19 booster vaccine hesitancy among the general population in Morocco.
Methods:
A cross-sectional study was conducted among 574 participants from primary healthcare centers in Fez, Morocco, between April 2022 and April 2023. Data were collected using a structured questionnaire based on the WHO SAGE framework, assessing socio-demographic, contextual, individual, group, and vaccine-specific determinants. Statistical analyses included chi-squared tests and multivariate logistic regression (P < .05).
Results:
Hesitancy toward the first booster dose was reported by 66.2% of participants. Vaccine-specific concerns were the strongest predictor (Adjusted Odds Ratio [AOR] = 27.6; 95% Confidence Interval [CI] = [11.1-68.3]; P < .001), followed by contextual factors (AOR = 7.8; 95% CI = [4.0-15.4]; P < .001) and individual/group determinants (AOR = 3.0; 95% CI = [1.6-5.6]; P = .001). Younger age (<46 years, AOR = 3.0) and lower income (AOR = 5.9) also increased hesitancy.
Conclusion:
Booster dose hesitancy in Morocco is driven by vaccine-specific concerns, contextual influences, and individual beliefs. Addressing these factors through targeted communication, trust-building strategies, and inclusive public health policies is essential to increase booster uptake and strengthen national pandemic response efforts.
Introduction
Coronavirus disease 2019 (COVID-19) is a highly contagious infection caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). 1 The global impact of COVID-19 has posed a significant threat to public health worldwide. As of January 5, 2022, the virus had spread to over 232 countries, infecting 298 582 789 individuals and causing 5 526 511 deaths. 2 In response, COVID-19 vaccination has emerged as a key strategy for mitigating the pandemic by reducing mortality and the severity of disease.3,4 Furthermore, the decline in immunity over time, whether following natural infection or vaccination, combined with the ongoing emergence of SARS-CoV-2 variants with potential for immune escape, underscores the need for booster doses of COVID-19 vaccines.5,6 Studies have shown that immunity wanes 4 to 6 months after the initial vaccination series, and receiving a booster dose significantly enhances immune responses compared to full vaccination with 2 doses.5,6 It induced higher seroconversion rates of antibodies and more significant neutralization antibody titers against various SARS-CoV-2 variants. Additionally, the booster vaccination resulted in a more robust cellular immune response, which is essential for long-term protection immune responses in healthy adults.7,8
Despite the robust evidence supporting the safety and efficacy of COVID-19 booster doses, their uptake has been hindered by widespread vaccine hesitancy.9,10 As of January 5, 2022, approximately 3 914 691 098 individuals worldwide had received full vaccination, while only 562 million had received a booster dose.4,11 Research indicates that willingness to accept a COVID-19 booster dose varies considerably across countries and is shaped by multiple factors.12,13 Socio-demographic characteristics, including gender, age, education, income, occupation, and marital status, play a pivotal role.12 -15 Furthermore, individual-level factors, including perceived risks and benefits of vaccination—such as protection against severe illness, reduced transmission, and the ability to return to normal life—strongly influence attitudes toward booster uptake. Trust in the efficacy and safety of vaccines, history of COVID-19 infection, and overall health status further contribute to these decisions. 16 Contextual factors are equally important and include regional and geographic disparities, the accessibility and clarity of health information, public skepticism, trust or mistrust in institutions, belief in conspiracy theories, and perceptions of various vaccine brands or technologies.17,18
In Morocco, by January 5, 2022, 22 956 802 people had received both doses of the COVID-19 vaccine. However, a significant proportion (70%) of individuals were hesitant about accepting the first booster dose despite the availability of a free vaccine. 19 Given this reality and the lack of sufficient data on the factors contributing to COVID-19 booster hesitancy in Morocco, it is crucial to conduct an in-depth investigation into the determinants of this hesitancy. Understanding these factors will be essential for developing well-informed vaccination campaigns and strategies to promote vaccine uptake.20,21 This study aims to comprehensively explore the factors contributing to first COVID-19 booster vaccine hesitancy among the general population in Morocco.
Materials and Methods
Study Population and Area
This cross-sectional study was conducted in Fez, Morocco, with participants recruited from all primary healthcare facilities between April 9, 2022, and April 27, 2023. The study targeted individuals aged 18 and older and employed a face-to-face data collection approach. The sample size was determined using a simple random sampling approach, with the formula n = P(1 − P) Z2α/i2. In this formula, n represents the sample size, z indicates a 95% confidence level (z = 1.96), P denotes a prevalence rate of 30.72 %; P is the global average hesitancy rate regarding the COVID-19 booster vaccination according to a systematic review (including a total of 42 studies representing 25 countries), 17 and i signifies a precision of 4%. As a result, the calculated sample size was 512 individuals.
Data Collection
Data were gathered through a structured questionnaire consisting of 40 questions: 9 assessing sociodemographic and clinical characteristics, and 31 focused on factors influencing COVID-19 Vaccine Booster Hesitancy, with responses recorded as “Yes” or “No.” The questionnaire was developed by the Laboratory of Epidemiology, Clinical Research, and Community Health, based on an extensive review of the literature and the WHO’s Strategic Advisory Group of Experts (SAGE) Working Group Determinants of Vaccine Hesitancy Matrix.22,23 The determinants were categorized into 3 categories: (1) contextual factors, (2) individual and group factors, and (3) vaccine-specific issues.
Study Variables
Sociodemographic Characteristics
The sociodemographic characteristics of the participants include gender (male or female), age (categorized based on the median into 2 groups: <46 or ≥46 years), marital status, level of education, profession, status as a healthcare professional, and income. The clinical characteristics cover the personal history of chronic diseases (Yes/No).
Additionally, participants’ vaccination status regarding COVID-19 vaccination is categorized into 2 groups: those who are hesitant about the first COVID-19 booster dose (those who received the first 2 doses of the vaccine on time and are hesitant to get vaccinated with the third dose of the vaccine) and those who are not hesitant (fully vaccinated with all 3 doses on time). 22
Context-Related Determinants
These determinants examine public opinion on various contextual factors influencing the COVID-19 vaccination decision in Morocco. Key questions (9 items) include whether the urgent rollout of a free vaccine is an effective strategy in controlling the pandemic and if the Moroccan population is perceived as fully participating in the national vaccination campaign. It also explores the role of media and social media in building vaccine confidence and whether the Ministry of Health’s communications have adequately addressed public concerns. Other questions assess the sufficiency of locally available information on the vaccination strategy, the perceived influence of the health pass on vaccination decisions, accessibility to vaccination sites, the practicality of the vaccination process, and the level of trust in vaccination site personnel.
Individual and Group-Related Determinants
This set of questions focuses on the personal beliefs and social influences that may impact an individual’s vaccination decision. Topics (12 items) include perceptions of COVID-19’s severity, commitment to preventive measures (like physical distancing and mask-wearing), and personal or close experiences with COVID-19 infections or related fatalities. Questions also examine past experiences with adverse vaccine reactions, personally and within social circles, and whether these experiences affected attitudes toward COVID-19 vaccination. Additional questions assess the level of belief in vaccination’s role in achieving herd immunity, the sense of civic duty among the target population for vaccination, confidence in the vaccine’s effectiveness within one’s social network, and whether household members express hesitancy toward vaccination.
Vaccine/Vaccination-Specific Determinants
This category explores beliefs about the COVID-19 vaccine (10 items), including perceptions of its rapid production and distribution timeline. It includes questions on whether individuals have delayed vaccination to observe outcomes in others and whether they believe the vaccine provides personal and community protection against the virus. Trust in the vaccine’s safety, concerns over serious side effects, and confidence in its efficacy are also evaluated. Additionally, the importance of booster doses, particularly the third dose, is addressed to understand views on their role in enhancing immunity. Finally, it examines whether individuals have received information from healthcare professionals involved in the vaccination program regarding the necessity of COVID-19 vaccination.
Coding of Determinants
Responses to questions within each determinant group were assigned a value of 1 for answers indicating vaccine hesitancy and 0 for those opposing it. The final score for each determinant group was calculated by summing the values of individual responses. These total scores were subsequently categorized into 2 groups: those suggesting a tendency toward vaccine hesitancy and those not indicating such a tendency, based on the median score. Specifically, a score greater than 2 for contextual determinants, greater than 7 for individual and collective determinants, and greater than 6 for vaccine-specific determinants was considered indicative of a tendency toward vaccine hesitancy. This approach enabled an objective distinction between participants exhibiting higher and lower levels of vaccine hesitancy within each determinant group.
Statistical Methods
Data entry was performed using Microsoft Excel 2013, and statistical analyses were conducted with SPSS (Statistical Package for the Social Sciences), version 26. Descriptive statistics were used to summarize the data: categorical variables were expressed as percentages, while continuous variables were presented as means with standard deviations. The primary dependent variable in this study was COVID-19 vaccine booster dose hesitancy. Independent variables included a range of sociodemographic characteristics—such as gender, age, marital status, educational level, profession, healthcare professional status, and income—as well as scores related to contextual determinants, individual and group determinants, and vaccine-specific determinants.
Bivariate analyses were conducted using chi-square tests to assess differences between vaccine-hesitant and non-hesitant groups across sociodemographic characteristics and determinant scores. Multivariable logistic regression analysis was then employed to investigate the association between vaccine booster dose hesitancy (dependent variable) and a set of independent variables, enabling the identification of factors significantly associated with the outcome after adjusting for potential confounders. Variables with a P-value <.20 in the bivariate analysis were included in the regression model, and the confidence level was set at 0.05 to determine statistical significance.
Ethical Issues
Data collection was conducted anonymously, and participation was entirely voluntary, with no incentives offered to participants. Before taking part in the study, all participants provided written informed consent by signing a consent form. Confidentiality was ensured throughout both the data collection and analysis phases. The study received ethical approval under approval number 01/22.
Results
Sociodemographic and Clinical Characteristics
This study included 574 participants, of whom 74.4% (n = 427) were women, with a mean age of 45.73 ± 16.95 years. Over half of the participants were married (57.8%, n = 332), 67.8% (n = 389) were literate (ie, individuals who had completed at least 1 level of formal education, whether primary, secondary, or higher), and 39.5% (n = 227) were employed, including 19.2% (n = 110) working in the healthcare sector. Among the participants, 23.2 % (n = 133) reported a monthly income of 3000 DHS or more, and 40.6% (n = 233) had chronic illnesses (Table 1). Regarding COVID-19 vaccination, 66.2% (n = 380) expressed hesitancy toward receiving the first booster dose, while 30.8% (n = 194) were not hesitant (having completed the 3-dose vaccination schedule on time).
Sociodemographic and Clinical Characteristics (N = 574).

Abbreviation: N, number.
Determinant Scores
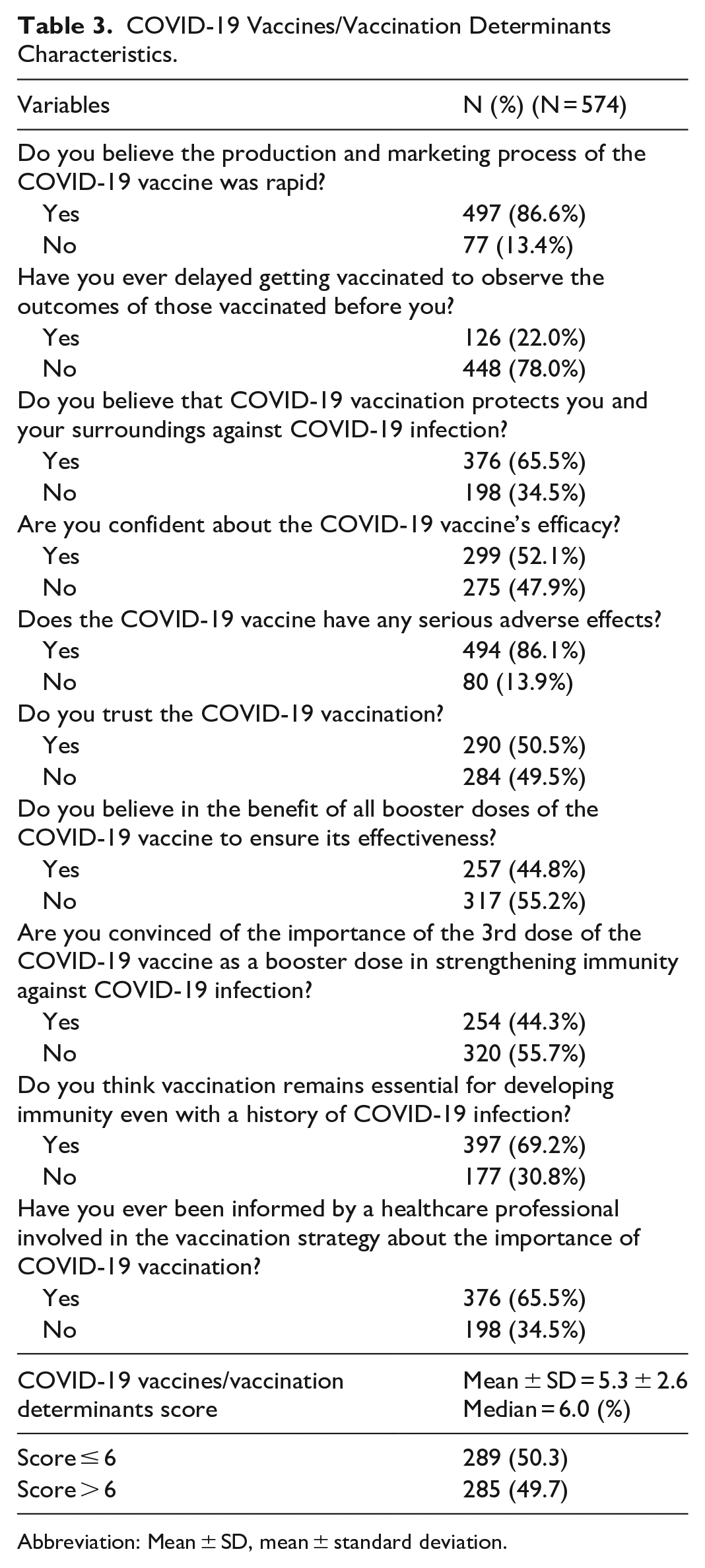
The findings reveal that 54.7% (n = 314) of respondents scored above the median value of 2 for contextual determinants, suggesting that these factors may exert a significant influence on hesitancy toward the COVID-19 vaccine booster dose (Table 2). In relation to vaccine-specific concerns, 50.3% (n = 289) of respondents scored at or below the median value of 6, indicating a relatively lower level of hesitancy concerning these particular issues (Table 3). Furthermore, 52.4% (n = 301) scored above the median value of 7 for individual and group determinants, suggesting that hesitancy toward the COVID-19 vaccine booster dose is notably associated with personal and group beliefs or experiences (Table 4).
Contextual Factors Characteristics.

Abbreviation: Mean ± SD, Mean ± standard deviation.
COVID-19 Vaccines/Vaccination Determinants Characteristics.
Abbreviation: Mean ± SD, mean ± standard deviation.
Individuals and Group Factors Characteristics.

Abbreviation: Mean ± SD, mean ± standard deviation.
Associated Factors With the COVID-19 Vaccine Booster Dose Hesitancy
Bivariate analysis identified significant factors associated with the COVID-19 vaccine booster dose hesitancy, including female gender (69.8% of hesitant participants, n = 298, vs 55.8% of non-hesitant participants n = 82; P = .002), age under 46 years (80.8% of hesitant participants n = 223 vs 52.7% of non-hesitant participants n = 53; P < .001), unmarried status (71.5% of hesitant participants n = 173 vs 62.3% of non-hesitant participants n = 125; P = .022), lack of income (70.7% of hesitant participants n = 312 vs 52.7% of non-hesitant participants n = 70; P < .001), literacy (71.7% of hesitant participants n = 279 vs 54.6% of non-hesitant participants n = 101; P < .001), employment as a healthcare professional (81.8% of hesitant participants n = 90 vs 62.5% of non-hesitant participants n = 290; P < .001), and absence of chronic illness (71.3% of hesitant participants n = 243 vs 58.8% of non-hesitant participants n = 137; P = .002; Table 5).
Associated Factors With COVID-19 Vaccine Hesitancy: Results of Bivariate Analysis.

Abbreviation: Mean ± SD, mean ± standard deviation.
Scores for contextual determinants were strongly correlated with the COVID-19 vaccine booster dose hesitancy; participants scoring above 2 were significantly more likely to be hesitant (91.4% of participants with score >2, n = 287, vs 35.8% of participants with score ≤2, n = 93; P < .001). Individual and group determinants also influenced hesitancy; those with scores above 7 were much more likely to be hesitant about the COVID-19 vaccine booster dose (89.4% of participants with score >7, n = 269, vs 40.7% of participants with score ≤7, n = 111; P < .001). The strongest association appeared in the COVID-19 vaccine/vaccination-specific determinants; participants scoring above 6 were almost universally hesitant (96.9% of participants with score >6, n = 280, vs 35.1% of participants with score ≤6, n = 100; P < .001; Table 5).
Logistic regression revealed that the COVID-19 vaccine booster dose hesitancy was significantly associated with multiple factors. Vaccine-specific concerns were the most impactful, with a vaccine score (AOR = 27.6; 95% CI = [11.7-68.3]; P < .001) showing the strongest link to hesitancy. Contextual determinants followed, with a contextual score (AOR = 7.8; 95% CI = [4.0-15.4]; P < .001), and individual and collective determinants also played a role (AOR = 3.0, 95% CI = [1.6-5.6]; P = .001). Sociodemographic characteristics were influential as well, mainly being under 46 years of age (AOR: 3.0; 95% CI = [1.7-5.5]; P < .001) and lack of income (AOR = 5.9; 95% CI = [2.7-12.6]; P < .001; Table 6).
Associated Factors With COVID-19 Vaccine Hesitancy: Results of Logistic Regression.

Abbreviations:
Discussion
Our study aimed to comprehensively explore the factors contributing to first COVID-19 booster vaccine hesitancy among the general population in Morocco. The findings revealed that 66.2% (n = 380) of participants hesitated to receive the first booster dose, while 30.8% (n = 194) completed the 3-dose vaccination on time. Studies examining public attitudes and hesitancy toward the first booster dose across diverse populations and cultural contexts have reported varying rates, with a global average of 30.72%.17,24 Notably, hesitancy increased slightly over time, rising from 29.46% in 2021 to 33.55% in 2022. 17
The results reveal several factors contributing to the reluctance to receive the first booster dose. Factors related to the vaccine and the vaccination process were significantly associated with hesitancy. This is a salient finding, as it underscores that hesitancy is not solely attributable to individual beliefs but is also considerably influenced by specific apprehensions regarding the vaccine and its administration. However, these findings require cautious interpretation due to wide confidence intervals for some estimates. Significant concerns included skepticism about the vaccine’s rapid development (86.6%, n = 497) and fear of severe side effects (86.1%, n = 494). Confidence in the vaccine’s efficacy was also a critical determinant (52.1%, n = 299). These findings align with previous research showing that vaccine safety and efficacy concerns significantly affect uptake, even when clinical evidence supports the booster’s safety, as seen in a systematic review of 30 studies that found only minor increases in adverse events after the third dose, similar to those seen after the primary series. 25 Concerns about side effects, both short-term and long-term, are significant factors in vaccine hesitancy, with many individuals fearing potential harm. Common side effects, such as fever, fatigue, and pain at the injection site, are typically mild and temporary. However, the fear of rare but severe reactions strongly influences vaccination decisions. Research shows similar results, and addressing these concerns through clear communication about the safety and benefits of the booster dose can help reduce hesitancy. 26 To maximize communication effectiveness, employing a range of dissemination channels and tailoring messages to the specific concerns of distinct population subgroups is essential.
Additionally, limited awareness of the need for booster doses to optimize vaccine efficacy emerged as a significant barrier, with 44.3% (n = 254) of participants expressing skepticism. Similar findings from other research indicate that skepticism about the value of booster doses can negatively affect vaccination decisions. 27 This highlights the need for targeted public health messaging to reinforce the role of booster doses in sustaining immunity and controlling the pandemic. 27 To ensure effectiveness, such strategies should prioritize the use of accessible language and comprehensible formats, deliberately avoiding technical jargon and overly complex terminology.
Contextual influences also played a role in booster dose hesitancy. Specifically, public trust in government health authorities was a salient factor, with 45.5% (n = 261) of participants expressing reservations about the adequacy of official communication in addressing their concerns. Additionally, policy measures such as health pass requirements were shown to negatively influence the vaccination decisions of 22% (n = 126) of respondents. These findings are in accordance with global research demonstrating that public trust in institutions and the perceived credibility of vaccine-related information exert a substantial influence on vaccine uptake, and that a propensity toward conspiracy theories is associated with increased hesitancy.17,28 To effectively address these challenges, it is imperative that health authorities ground booster dose recommendations in robust scientific evidence, carefully considering both public health needs and the dynamic nature of the pandemic. Moreover, cultivating trust and reducing hesitancy necessitates clear, timely, and effective communication and the implementation of well-designed vaccination strategies. 29
Individual and collective determinants were also identified as significant factors influencing booster dose hesitancy. Prominent among these were personal beliefs concerning the perceived severity of COVID-19 (71.6%, n = 411), perceptions of vaccination as a civic responsibility (51.7%, n = 297), and beliefs regarding the role of vaccination in achieving herd immunity (66%, n = 379). Social influences, including vaccine hesitancy among family members (63.6%, n = 465) and prior adverse experiences with vaccination, whether personal (15.9%, n = 91) or vicarious (13.4%, n = 77), were also shown to contribute to hesitancy. These observations align with findings from previous studies,17,24,28 that have emphasized the importance of addressing not only individual apprehensions but also the broader social context in which vaccination decisions are made. This body of evidence suggests that public health campaigns should extend their focus beyond individual attitudes to encompass the social environments in which individuals are embedded to enhance booster dose acceptance and facilitate the attainment of herd immunity. 29
Furthermore, sociodemographic characteristics, such as age and income level, were found to be correlated with hesitancy. Younger individuals (under 45 years of age) exhibited higher levels of hesitancy, a finding consistent with other studies documenting generational differences in vaccine acceptance. Conversely, older adults (65 years and older) demonstrated lower hesitancy, likely reflecting their heightened perception of the risk of severe COVID-19 outcomes.14 -17,28 Lower income was also associated with reduced vaccination rates, a finding that agrees with prior research indicating that socioeconomic disparities frequently exacerbate health inequities, including inequities in access to vaccines.17,27,28 To effectively increase vaccine acceptance, public health efforts should prioritize the development of tailored awareness campaigns that target specific demographic groups, with a particular focus on younger individuals. Concurrently, ensuring equitable access to booster doses across all population segments is essential for improving vaccination coverage and mitigating health disparities.
This study stands out for its comprehensive analytical framework, which explores sociodemographic, contextual, individual, and vaccine-specific determinants of COVID-19 booster hesitancy. By adopting this multidimensional approach, the research provides a nuanced understanding of the complex interplay of factors affecting vaccine uptake. The robust sample size of 574 participants ensures the statistical power and reliability of the findings, allowing for generalizable conclusions within the Moroccan population. Furthermore, the data collection tool was rigorously developed based on the WHO SAGE framework and a thorough literature review, ensuring its validity and relevance. The diverse representation of participants, encompassing different age groups, income levels, education statuses, and healthcare roles, further strengthens the applicability of the results across various demographic segments.
Some limitations should be considered in this study. First, its cross-sectional design captures data at a single point in time, which may not fully reflect changes in attitudes over time. However, in an urgent context like the COVID-19 pandemic, where booster doses are crucial for controlling virus spread, this approach provides valuable insights into vaccine hesitancy. It also serves as a foundation for future longitudinal studies to track trends and assess intervention impacts. Although self-reported data may introduce biases, this limitation is partially mitigated by its widespread use in similar studies. Additionally, qualitative interviews could complement these findings, enhancing data validity. While this study did not extensively examine cultural and psychosocial factors, future research could address these dimensions using validated psychological scales and qualitative methodologies to gain a more comprehensive understanding of vaccine hesitancy.
Conclusion
This study highlights the main determinants of first COVID-19 booster dose hesitancy in Morocco, particularly vaccine-related fears, contextual mistrust, and personal or social beliefs. These findings underscore the urgent need for targeted, culturally sensitive public health strategies that build confidence in vaccines, improve awareness, and address socio-demographic disparities. Although specific interventions were not evaluated, our results provide a solid foundation for designing evidence-based communication campaigns and policy actions aimed at improving booster uptake. Promoting booster acceptance will be critical to strengthening collective immunity and enhancing preparedness for future public health challenges.
Footnotes
Acknowledgements
The authors thank all participants for their participation and contribution to this study.
Ethical Considerations
This study was approved by the Fez University Hospital Ethics Committee (Approval No.: 01/22) on April 6, 2022.
Consent to Participate
Written informed consent was obtained from all participants before their inclusion. Each received an information sheet outlining the study’s objectives, procedures, and benefits. Participation was entirely voluntary, with no compensation provided. As the study involved only individuals aged 18 years and older, parental consent was not required.
Consent for Publication
Not applicable. This study does not include any identifiable individual details, images, or videos that require explicit consent for publication.
Author Contributions
All authors contributed equally to this work and have read and approved the final manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are fully presented within the manuscript.