
Abstract
In this practice note, we document the progression of the Community Vaccine Collaborative (CVC), on which we first published in 2021. The CVC convened to address deep COVID-19-related disparities affecting the Black, Latine, immigrant/refugee, and lesbian, gay, bisexual, transgender, queer, (questioning), intersex, asexual, and (agender; LGBTQIA+) communities. The COVID-19 pandemic is rooted in centuries of oppression and marginalization leading to inequities and required dedicated focus to support marginalized communities in times of crisis. The CVC comprises community members, community-based organizations, health care providers, researchers, health systems leaders, and public health practitioners (among others), all of whom are dedicated to promoting COVID-19 vaccine equity. As the pandemic shifts and changes, so too has our group, to remain relevant to community needs and priorities. This article details Year 2 of the CVC, focusing on how we have grown and sustained this unique partnership. We also share results from an evaluation of the CVC, documenting participation in the collaborative space and alignment with CVC core principles. Finally, we discuss next steps and implications for the CVC including our pivot from vaccines to community vitality as we expand and sustain our collaborative efforts to address the ongoing COVID-19 pandemic and intersecting public health crises.
Keywords
Assessment of Need
The COVID-19 pandemic compounded pre-existing inequities rooted in racism, xenophobia, transphobia, and classism, creating disproportionate health, economic, and social burdens for communities of color (particularly Black, Latine, and Indigenous; Acosta et al., 2021), people living in poverty, immigrant, refugees, non-English-speaking communities, and people identifying as lesbian, gay, bisexual, transgender, queer, (questioning), intersex, asexual, and (agender; LGBTQIA+; Azucar et al., 2022). Throughout the pandemic, community-based organizations played an instrumental role through resource distribution, vaccine clinics, and COVID-19 education and advocacy (Michener et al., 2020).
The Community Vaccine Collaborative (CVC) is a community–academic partnership that convened in July 2020 to promote COVID-19 vaccine equity. In March 2021, we published a Practice Note describing the CVC’s first year, capturing the CVC’s key principles, including dismantling power inequities, prioritizing community voices, building trustworthiness, and focusing on reciprocity (Scott et al., 2021). The goal of the current Practice Note is to describe our sustained and dynamic efforts during the CVC’s second year, present evaluation data, and discuss next steps in our work. The purpose for documenting this work a year later is to highlight the benefit of focusing on reciprocity, trustworthiness, and equitable compensation as guiding principles from the start, which has sustained this collaboration throughout a devastating public health crisis.
Advocacy Efforts
Speakers’ Bureau
The CVC hosts a program where community-based organizations can request community health workers and health care providers to present on COVID-19 vaccinations, testing, and education. We have hosted more than 100 events at a variety of settings including school board meetings, high schools, and community events and have presented in multiple languages including Swahili, Spanish, Nepali, Arabic, and Uzbek.
Workgroups
The initial CVC work groups consisted of the Trustworthiness group (discussing how researchers and health care providers can earn trust/become trustworthy) and the Community Outreach group (planning vaccine clinics and events). We expanded the workgroups to include a Youth Outreach group to tailor messaging and community building to youth, and an Immigrant and Refugee group, focused on the vaccination experience of non-English-speaking immigrant and refugee communities. We attempted to create a Rural Health group to address low vaccination rates in rural communities; however, this group has been slow to gain traction due to geographical constraints that affect relationship building and a shortage of community health workers in these areas.
Co-Created Research
While research was not the initial goal of the CVC, workgroups organically proposed ideas for projects aligned with our core principles. For example, the Immigrant and Refugee workgroup co-conducted multilingual focus groups on COVID-19 vaccination experiences and the Trustworthiness group co-created surveys to better understand trusted sources for COVID-19 information among Black and Latine adults. Our team paid attention to knowledge translation, leveraging social media, community-based events, infographics, academic papers, and webinars to disseminate our work.
CVC evaluation
To evaluate our space, the CVC co-created and distributed surveys to former and current CVC members and reviewed attendance records. The CVC includes 115 members, with 20 to 35 attending each meeting. Eighty completed the survey; Table 1 outlines evaluation results including demographics and adherence to core principles. Fifty-six percent of participants felt prepared to share COVID-19-related information; 38% felt moderately prepared; and 6% felt unprepared. Participants considered the CVC to be highly trustworthy, inclusive, equitable, and a space for mutual learning. The CVC evaluation was deemed as exempt by the University of Pittsburgh Institutional Review Board (IRB).
CVC Evaluation Results: Demographic Characteristics of Survey Respondents and Their Perspectives on Adherence to CVC Core Principles
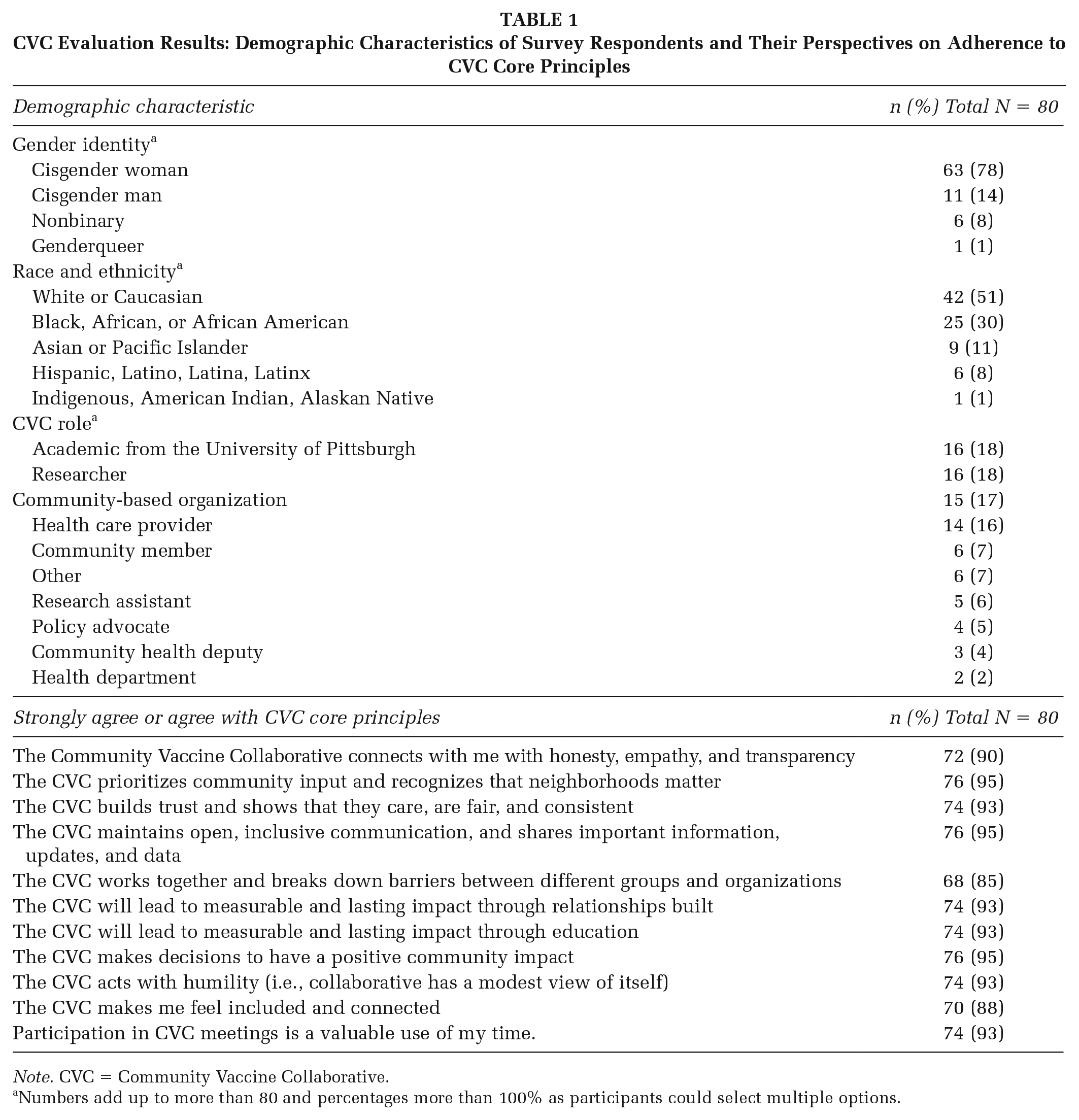
Note. CVC = Community Vaccine Collaborative.
Numbers add up to more than 80 and percentages more than 100% as participants could select multiple options.
Future Directions
A Shift from Vaccines to Vitality
We have transitioned the CVC from a specific focus on vaccines to thriving and vitality more broadly to transform our coalitional crisis response into a sustained community and justice-oriented response. Aligned with this mission change, we have changed our name to the Community Vitality Collaborative. The Youth Outreach group is developing ways to address stress and trauma experienced by young people due to violence and mental health crises. The Community Outreach group and Speaker’s bureau are expanding to focus on topics such as healthy eating and mental health. We are also well positioned to support new infectious disease concerns; as an example, we have already convened educational workshops on Monkeypox and are working together to expand testing and vaccine access. The Immigrant and Refugee group is focusing on language equity in research and health care. However, we also recognize that the COVID-19 pandemic is ongoing, and many are still at high risk for significant morbidity related to COVID-19. Therefore, we remain attuned to sharing COVID-19-related updates.
Developing New Workgroups to Meet Equity Needs
We are continuing to create new workgroups; most recently, we have convened an IRB group to increase inclusivity and transparency of the IRB, as well as amplify the voices of groups historically excluded or harmed by research (e.g., Black, immigrant and refugee, LGBTQIA+, those living with disabilities; Scharff et al., 2010). We continue to refine and discuss CVC goals to determine new or changing needs.
Systems-level factors contributing to our sustained collaborative effort: The CVC has worked together to secure funding from multiple internal and external sources to provide and sustain infrastructure. Equitable compensation of partners for their time and expertise was key to our success. Using project management tools to help people connect with opportunities and resources even when they could not attend meetings was critical for communication. Providing ample unstructured time during meetings to amplify community priorities and concerns was also vital to open dialogue and ongoing trust building.
Sustained Space for Healing and Atonement
As we reflect on the space we created and nurtured during multiple interweaving public health epidemics, we recognize that the CVC has become a space of healing and respite for those on the frontlines of health and health care crises. CVC members noted how this space helped them build networks, develop partnerships, share sorrows, and support each other during ongoing community and societal-level traumas. The CVC is also a place to discuss what repair and atonement may look like from community members’ perspectives, to reflect on the harm medical systems and research have caused communities, and to build a brighter future together. The Community Vitality Collaborative is committed to ongoing relationship building and creating a virtual community of people deeply dedicated to health equity.
Footnotes
Acknowledgements
We would like to acknowledge past and present members of the Community Vaccine Collaborative for their sustained work during the pandemic. The CVC received funding from a University of Pittsburgh Momentum Scaling Grant, a grant from the Allegheny County Health Department, and from Dr. Judy Martin.