
Abstract
Introduction:
Major depression is a common disorder affecting millions of adults each year. Many population-based surveys showed an increase in the number people with symptoms of depression at the onset of the COVID-19 pandemic. Our aim was to determine and compare the prevalence of depression risk in a primary care setting before and during the COVID-19 pandemic.
Methods:
We conducted a cross-sectional study based on retrospective review of medical records from a large suburban primary care clinic. Records of adults 18 years and older, seen between January 1, 2019 and December 31, 2020 and who had also been screened for depression using the 9-item Patient Health Questionnaire (PHQ-9) were analyzed.
Results:
Adults 18 years and older who completed the PHQ-9 assessment in 2019 and 2020 were 5078 and 4338, respectively. Risk of depression was 18.2% in 2019 and 14.8% in 2020 (P < .001). In adults under 50 years and those 50 years and older, depression risk was 20.7% versus 15.3% in 2019 (P < .001) and 17.3% versus 12.6% in 2020 (P < .001), respectively. In females, depression risk was 20.0% in 2019 and 16.8% in 2020 (P < .01), and in males, 14.1% in 2019 and 10.6% in 2020 (P < .01).
Conclusion:
Although our results did not reflect the published literature reporting a higher prevalence of depression during the COVID-19 pandemic, they were consistent with reports of increased risk in females and younger adults.
Introduction
Major depression is one of the most common morbidities in the United States. 1 A national survey in 2020 showed an estimated 21.0 million adults 18 years and older (ie, 8.4% of the U.S. adult population) had had at least one episode of depression in the past year. 1 Increased episodes of depression in the period 2020-2021 are thought to be related to the COVID-19 pandemic.2-6 While episodes of depression have increased, the number of providers caring for these patients has not changed. 7 The global burden of the impact of depression and anxiety disorder underscores the need to identify and take action to mitigate their impact on morbidity and mortality. 8 Furthermore, the increased rate of suicidality in adults and teens makes it urgent to identify these patients and intervene when appropriate.6,7,9 Primary care practices are often the first point of contact for patients suffering from depression and anxiety.
Various screening tools for early detection of depression exist, many of which are in the public domain and require no permission for use.10-12 The 9-item Patient Health Questionnaire (PHQ-9) is one of the tools validated as an appropriate screening tool to identify patients at risk for major depressive disorder and it is recommended for screening by the United States Preventive Services Task Force (USPSTF) for use in persons 12 years and older. 13
Several factors may influence the prevalence of mental health symptoms. Patients with diagnosed psychiatric disorders tend to show a high prevalence of anxiety and depressive symptoms. 14 Chronic morbidities may also be associated with depression and other mental health symptoms. 15 Racial/ethnic minorities had a higher prevalence of suicidal ideation in a national survey in 2020. 6 Studies have shown an association between sex and depression with females having a greater disease burden.16,17
In order to validate the need for more mental health services, we aimed to describe the prevalence of depression risk in a primary care setting and to compare the prevalence before and during the COVID-19 pandemic using clinic data for 2019 and 2020, respectively. We hypothesized that risk of depression would be higher in 2020 than 2019, the pre-pandemic period.
Methods
We conducted a cross-sectional study using medical records of patients 18 years and older who had been seen by their primary care physicians (PCPs) at a suburban academic family medicine clinic from January 1 to December 31 in 2019 and 2020. Patients who had not completed the PHQ-9 assessment were excluded from the analysis.
Main outcome of interest was depression risk assessed by the PHQ-9 score. The PHQ-9 is routinely used in our clinic for screening adult patients for depression. This is completed by the patient on every visit to the clinic. Those found to be at risk of depression are then referred for management by mental health professionals. PHQ-9 is a self-administered instrument designed to make criteria-based diagnoses of depressive disorders and is valid for determining the depression severity. 18 It has a scale of zero to 27, with higher scores indicating higher risk. Using the PHQ-9 tool, depression risk is described as mild, moderate, moderately severe and severe, if scores are 5-9, 10-14, 15-19, and 20-27, respectively. Screening for depression is recommended by the USPSTF in all adults, children over the age of 12 and pregnant women. For the purpose of this study we defined depression risk as scores of 10 or higher. This was to ensure that we captured those most likely to be at risk of major depression. PHQ-9 score of 10 or greater has demonstrated a sensitivity of 88% and a specificity of 88% for major depression. 18 For patients who were screened multiple times with the PHQ-9 instrument in this study, depression risk was considered present the first time a score of 10 or higher was recorded. We conducted electronic chart review to collect data on demographics (age, sex, and race/ethnicity), presence of comorbidities (hypertension, hypothyroidism, and diabetes), and other mental health conditions (anxiety, schizophrenia, bipolar disorder). These demographic and clinical data were included in the study because of their known influence on depression.6,14-17 Age was defined as the completed years of life recorded in the patient’s medical records at the time of the relevant PHQ-9 score. Using age, we divided the study population into categories: 18 to 25, 26 to 49, and 50 years or older. Race/ethnicity information was used in classifying patients into Caucasians, African American, Hispanic and Other. Patients who did not fall into any of these 3 race/ethnicity categories were classified as Other, and included population groups such as Asian, Native American/Alaska Native, Pacific Islanders, etc. who were of small numbers.
The overall depression risk for each year was estimated using the total number of unique patients who scored 10 or higher on PHQ-9 screening on at least one occasion in the year as a percentage of the total number of unique patients seen. We also estimated the risk by age categories (18-25, 26-49, and ≥50 years), sex and race/ethnicity as available in medical chart (Caucasian, African American, Hispanic, and Other) for each of 2019 and 2020, and compared the figures using a 2-sample test of proportions. We also compared the mean PHQ-9 scores for 2019 and 2020 using a 2-sample T test. A 2-sided test with level of significance of 5% was used.
This study was determined to qualify for exempt status by our Institutional Review Board (IRB). All authors certify responsibility for the content of the manuscript.
Results
The number of unique patients 18 years and older who had completed the PHQ-9 assessment in 2019 and 2020 were 5078 out of 5261 (96.5%) and 4338 out of 4389 (98.8%) respectively, seen in the clinic. Subjects with no PHQ-9 information were not further analyzed. Table 1 shows the demographic and clinical characteristics of the participants for 2019 and 2020. While the population characteristics for the 2 years were largely similar, the proportion of patients 26 to 49 years were relatively fewer in 2020 than in 2019 (39.1% vs 42.4%, P < .01) while older adults 50 years or older were relatively more in 2020 than 2019 (52.1% vs 48.1%, P < .01). In addition, proportion of patients with diabetes and hypertension were significantly higher in 2020 than 2019 (19.8% vs 18.1%, P = .04 and 50.0% vs 45.3%, P < .01, respectively). Patients with PHQ-9 scores ≥10 were 922 in 2019 and 644 in 2020. Depression risk prevalence was 18.2% in 2019 and 14.8% in 2020 (P < .001). The PHQ-9 scores ranged from 10 to 27 for both years. Mean PHQ-9 scores were 14.9 (±4.2) in 2019 and 15.1 (±4.3) in 2020 (P = .36). Table 2 shows prevalence of depression risk among the patients who had PHQ-9 information for 2019 and 2020.
Participant Characteristics.

Prevalence of Depression Risk in Study Participants in 2019 and 2020.

Comparing risk prevalence between 2019 and 2020.
Age-specific depression risk for 2019 and 2020 were 24.0% versus 17.9% (P = .03) in the age group 18 to 25 years, 20.1% versus 17.2% (P = .02) in 26 to 49 years and 15.3% versus 12.6% (P < .01) in 50 and older years. When age was dichotomized into those under 50 years and 50 years and older, depression risk was 20.7% versus 15.3% in 2019 (P < .001) and 17.3% versus 12.6% in 2020 (P < .001). Depression risk in females was 20.0% in 2019 and 16.8% in 2020 (P < .01). In males, risk of depression was 14.1% in in 2019 and 10.6% in 2020 (P < .01).
Among racial and ethnic groups, depression risk in 2019 and 2020 was 18.4% versus 15.4% in Caucasians (P = .037), 19.5% versus 15.4% in African Americans (P < .001), 23.6% versus 13.7% in Hispanics (P = .015) and 14.6% versus 13.3% in Other (P = .354), respectively.
Depression risk was moderate in 54.5%, moderately severe in 29.6% and severe in 15.9% in 2019 and 52.3%, 30.9% and 16.8% in 2020, respectively. Figure 1 is a bar chart showing the depression risk severity for 2019 and 2020.

Bar chart showing depression risk severity for 2019 and 2020.
Figure 2 shows the prevalence of comorbidities in the patients with depression risk. In 2019, 10.5% had anxiety, 2.9% schizophrenia, and 14.1% bipolar disorder while in 2020, the prevalence of anxiety disorder, schizophrenia, and bipolar disorder was 12.3%, 3.1%, and 14.1%, respectively, with no significant difference between 2019 and 2020 values (P > .05). Prevalence of hypertension, diabetes and hypothyroidism among patients with depression risk was respectively 57.6%, 20.6%, and 8.6% in 2019, and 44.7%, 24.1%, and 8.7% in 2020.
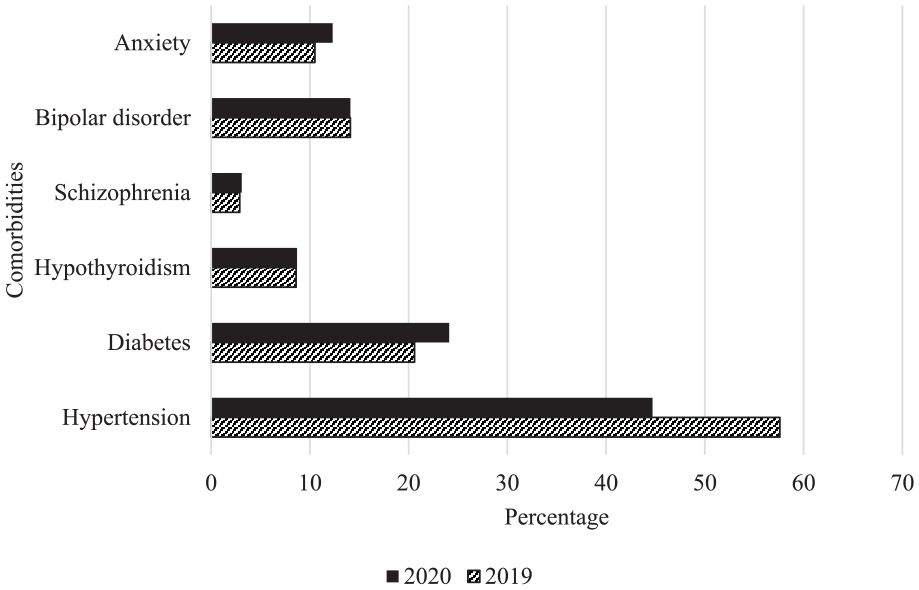
Prevalence of comorbidities in patients with risk of depression in 2019 and 2020.
Discussion
We assessed and compared the prevalence of depression risk in patients seen at a suburban academic primary care clinic in 2019 and 2020, that is, before and in the era of COVID-19. We found that the prevalence of depression risk was higher in 2019 than 2020. Depression risk was also higher in females than males in both years. All age group categories had a significantly higher risk of depression in 2019 than in 2020. Older adults (50 years and older) had lower depression risk than younger adults (under 50 years) in both years. Prevalence of anxiety disorder, schizophrenia and bipolar disorder among the patients in 2019 did not significantly differ from those in 2020.
Unlike many other studies, we used the PHQ-9 only as a screening tool so that those at risk of major depression would be evaluated further and managed appropriately. We therefore reported the prevalence of risk of depression. Many studies use a screening tool and report disease prevalence. This is likely to overestimate the true prevalence. 19
The finding of a higher depression risk prevalence in 2019 than 2020 was unexpected as a number of studies had reported an increased prevalence of mental health symptoms during, and particularly in the early part of the COVID 19 pandemic.3,4,8 In fact, several studies have found higher depression prevalence or symptoms of depression in 2020 than in 2019 due to, among other factors, the general environment of uncertainty and effects of the social restrictions associated the COVID-19 pandemic.4,8,20 One study that looked at the impact of COVID-19 on the global prevalence and burden of depressive and anxiety disorders in the general population, found an increased prevalence in both conditions in 2020. 8 It specifically found an association between the daily COVID-19 infection rates and associated reductions in human mobility to correlate with increased prevalence of major depression and anxiety. 8 Daly and Robinson found a small increase in mental health symptoms at the onset of the pandemic but decreased to pre-pandemic levels by middle of 2020. 21 A study by Fancourt et al reported the highest levels of depression and anxiety in their study population in the early stages of the pandemic which declined fairly quickly. 3 On the hand, one study did not find any significant change in the prevalence of depression and suicidal ideation before and after the COVID-19 outbreak. 22 While our results are counter to that which was expected, one must account for the fact that fewer patients were seen in 2020 than in 2019. Furthermore, during the beginning of the pandemic, there were approximately 6 weeks when patients were not seen in the office and questionnaires were not administered. Because our depression screening was administered in person, it is unclear whether our data missed the apparent surge in prevalence observed in the early part of the pandemic due to the more stringent social restrictions imposed, as reported in some studies. It is possible that the clinic failed to capture patients who were suffering from mental distress due to the COVID-19 pandemic as those patients might be more likely to stay isolated and not venture into public spaces for fear of the infection. It is unlikely that the few differences in the demographic characteristics of the patient populations in 2019 and 2020 could account for the decline in risk prevalence in 2020 as nearly every population category saw a decline in risk. It is uncertain if uptake of telemedicine was higher in patients with mental health symptoms and contributed the decline in numbers of such cases seen at the clinic in person. It must be noted that while many of the studies reporting higher prevalence of depression and other mental health symptoms in 2020 were population-based studies, ours was clinic-based and most likely captured patients who were seeking treatment for other illnesses.
Our finding of a higher risk of depression in females supports the general observation of a higher prevalence of depression among women than in men in the United States and globally. 1 For example, a national population based survey in the US population in 2019 found 21.8% of women had experienced depressive symptoms in the previous 2 weeks compared to 15% of men, while a 2002 Canadian survey, the Canadian Community Health Survey, found the annual prevalence of major depressive disease in women and men to be 5.0% and 2.9% respectively.16,17 The pandemic did not appear to have altered that pattern. Attempts to explain the sex disparity in depression has mainly been along the lines of socio-culture and biology although the evidence in support of the former is weak.23,24 In addition, the finding of younger adults being more at risk of depression than older adults in both 2019 and 2020 mirrors the reported prevalence of major depressive episodes in the U.S. 1 Reasons proffered to explain the age disparity in depression include more satisfaction with life in old age even in the face of more illnesses and physical challenges. It has been suggested that the observed low prevalence of depression in older adults may be a result of under-reporting due to confounding with somatic symptoms. 25 However, other studies do not support that notion.26,27
We did not analyze the data for associations of depression with chronic comorbidities. However, our data shows a large number of patients with hypertension and diabetes. This is unsurprising as our population consisted of patients seeking care at a primary care facility, many of whom were likely to have chronic comorbidities.
We looked at a patient population in a primary care clinic, the first stop where patients are screened for mental health and we report depression risk prevalence. Our results need to be interpreted with caution due to some limitations in the study. This was a single center study in a suburban academic primary care clinic using medical records. We were limited in the variables existing in the medical records. Our population comprised adults seeking care, primarily for other comorbidities and our findings may not be applicable to the general population. Our study did not use a longitudinal closed cohort of patients so the individuals studied in the 2 years could differ in various aspects and some may appear in both years. Although the population profiles for the 2 periods studied were reasonably similar, they were not the same.
We report a significant change in risk of depression using PHQ-9 screening tool among adult patients 18 years and older seen in a primary care clinic before and during the COVID-19 pandemic. Although our results do not reflect the published literature reporting a higher prevalence of depression during the COVID-19 pandemic, our findings were consistent with reports of increased risk of depression in females and younger adults. The relatively higher risk of depression among the patient population compared to findings in population studies, buttresses utilizing primary care providers in the management of depression.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.